
Abstract
Age estimation is a critical component in forensic investigations. The fusion stages of bones, particularly the medial clavicular epiphysis, offer reliable markers for estimating age, especially in individuals below 25 years. Despite the available data in the literature, population-specific standards should be developed and validated using the contemporary geographical population. This study aimed to investigate the fusion patterns of the medial clavicular epiphysis in the North Indian population using post-mortem computed tomography (PMCT) scans. This study comprised 500 samples (327 males and 173 females) with ages below 25 years. Using PMCT scans, the ossification patterns of the medial clavicular epiphysis were classified into four stages: Stage 0 (absence of ossification center), Stage 1 (appearance without fusion), Stage 2 (partial fusion), and Stage 3 (complete fusion). This study revealed a significant correlation between fusion stages and chronological age, with Spearman’s correlation coefficients of ρ = 0.819 for males and ρ = 0.797 for females, and statistically significant gender differences. Linear regression models were developed for both sexes, predicting age with mean absolute errors (MAEs) of 1.36 for males and 1.88 for females. Validation of these models demonstrated their utility in estimating age with high accuracy, though the models tended to slightly underestimate age, especially in females. This study confirms that medial clavicular epiphyseal fusion patterns are reliable indicators for age estimation in the North Indian population. The findings emphasize the importance of population-specific criteria in forensic age estimation, providing a precise tool for forensic practice.
Keywords
Introduction
Age estimation is essential in various fields, including age verification for legal compliance, identifying missing persons in law enforcement, immigration purposes, educational placement, fair sports competition, demographic research, and social service eligibility. It is a critical component of forensic investigations, particularly in establishing the identity of individuals. Forensic anthropology and radiology have made significant strides in utilizing the fusion stages of various bones as reliable indicators for age estimation.1, 2 Among the various bones of the human body, the clavicle has gained importance due to its relatively consistent fusion patterns, making it a useful indicator for age estimation, especially in young individuals. 3 The clavicle, commonly known as the collarbone, is a long, slender bone with two ends, the medial and lateral ends articulating with the sternum and acromion process of the scapula, respectively. The fusion of the medial clavicular epiphysis, where the epiphysis fuses with the diaphysis, provides crucial insights into an individual’s age. 4 This progressive fusion process, which transitions from the absence of an ossification center to complete fusion, follows a predictable sequence that can be effectively assessed through radiological methods such as post-mortem computed tomography (PMCT) scans.5, 6 Understanding the fusion patterns of the medial clavicular epiphysis within specific populations is essential for precise age estimation in forensic contexts. In the context of the Indian population, characterized by its unique genetic and environmental factors, the development of a reliable age estimation method holds paramount importance. This study aims to investigate the fusion stages of the medial clavicular epiphysis in individuals aged 0–25 years within this population. By employing a brief four-stage classification system, this study seeks to evaluate and validate the medial clavicular epiphysis as a tool for accurately estimating the age of individuals below 25 years.
Methods
This retrospective study was performed using PMCT scans of cases brought for medicolegal autopsies at the Department of Forensic Medicine and Toxicology of our institute. This retrospective study comprised 500 samples (327 males and 173 females) with an age below 25 years belonging to the North Indian population. All cases brought for autopsy with a valid proof of age were included in this study. Cases with thoracic trauma, thoracic surgeries, developmental disorders, malignancies involving bone or bony metastases, and advanced decomposition were excluded from the study. The ossification patterns of the medial clavicular epiphysis were assessed. This study employed the following four-stage classification system to evaluate the PMCT scans of the clavicle (Figure 1).
PMCT Scans Showing Stages of Fusion of Medial Clavicular Epiphysis: A, Ossification Center Not Appeared; B, Ossification Center Appeared, Not Fused; C, Ossification Center Partially Fused; D, Ossification Center Completely Fused.
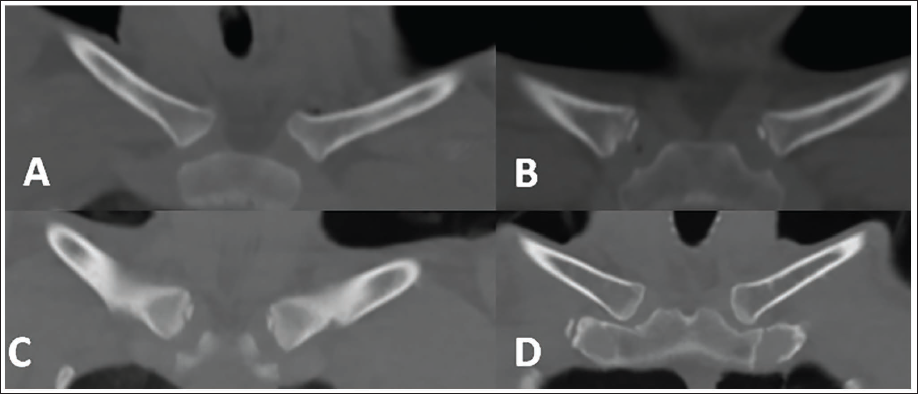
Stage 0: The ossification center has not appeared.
Stage 1: Ossification center appeared, but fusion has not started.
Stage 2: Partial fusion of the ossification center.
Stage 3: Complete fusion of the epiphyseal ossification center with diaphysis. The epiphyseal scar might still be appreciable.
This system was employed in view of the image resolution generated by the specified technical parameters of the computed tomography (CT) scan machine. Non-contrast PMCT was done using a 16-slice multi-slice CT spiral scanner, Aquilion Lightning TSX-035A CT (Toshiba America Medical Systems, Tustin, CA). The scanner was operated at 120 kV with automatic mA settings. The bodies were scanned in a supine position with arms placed beside the body. The maximum dose length product (DLP), computed tomography dose index (CTDI) of the cases extended up to 1342.37 mGy.cm and 7.96 mGy, respectively. The scan covered the upper body in a single series, starting from the neck to the mid-chest (scan length varied in different individuals). The machine had a collimation of 16 × 1 mm, and image reconstruction employed the whole-body filter (FC18 Kernel) with a 1 mm slice thickness. The raw data were subsequently reconstructed into multiplanar and volume-rendered images, which were examined using the bone window of Vitrea 7.10 software. The collected data were statistically processed using STATA statistical software version 11 (StataCorp LLC, Lakeway Drive, College Station, Texas, USA).
Results
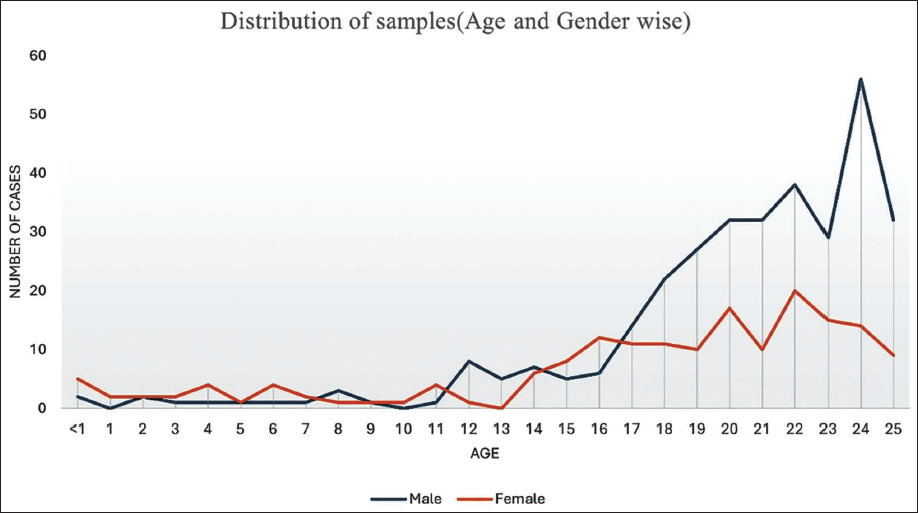
A total of 500 cases were evaluated, comprising 327 males (65.4%) and 173 females (34.6%). It is noteworthy that there was variability in the number of participants across different age groups. The majority of cases were in the older age categories, with the highest number of participants in both sexes falling within the 18–25 years age group. Figure 2 presents the number of male and female participants in each age category, providing insights into the demographic composition of our sample population.
Line Chart Depicting the Distribution of Samples According to their Age and Sex.
For Males
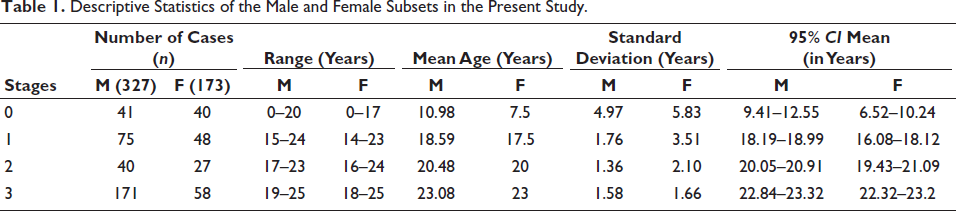
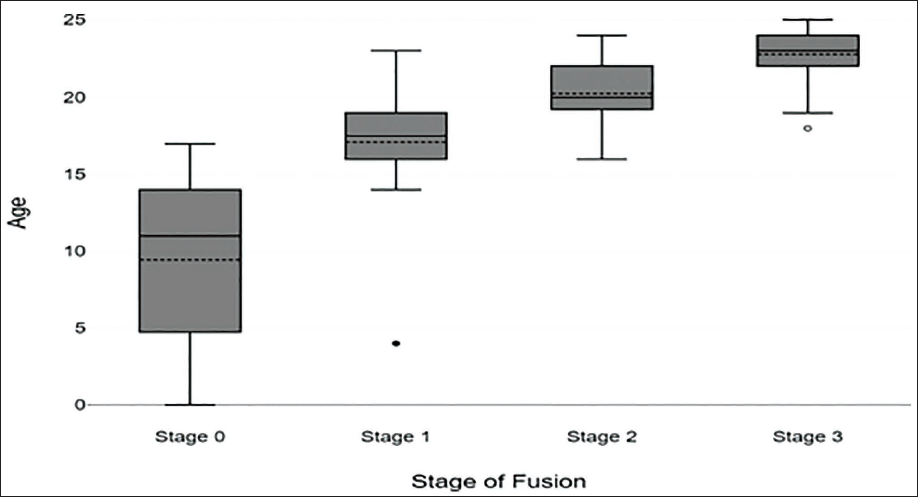
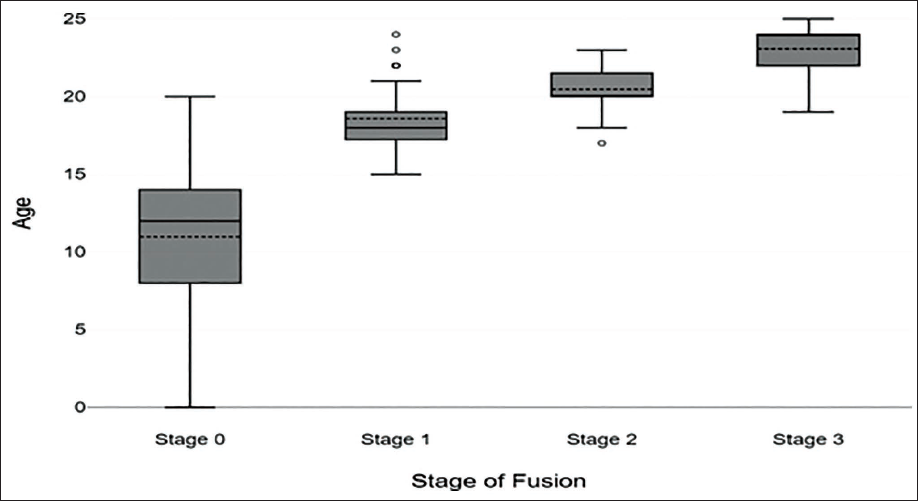
The mean age of the male population was 19.264 years (SE = 0.245). The distribution of ages exhibited a median of 21 years and a mode of 24 years. The descriptive statistics for male participants across the four fusion stages are detailed in Table 1. The mean age progressed predictably from Stage 0 (x̄ = 10.98 years, SD = 4.97) to Stage 3 (x̄ = 23.08 years, SD = 1.58). The widest age range (0–20 years) and highest variability (SD = 4.97) were observed in Stage 0. Conversely, the fusion stages, particularly Stage 2 (x̄ = 20.48 years, SD = 1.36) and Stage 3 (x̄ = 23.08 years, SD = 1.58), exhibited lower variability, reflecting a narrower age window for active fusion and completion of growth. The distribution of cases per stage is visually represented in Figure 3.
Descriptive Statistics of the Male and Female Subsets in the Present Study.
Stage-wise Age Distribution of Males.
For Females
Table 1 presents the descriptive statistics for the female cohort. The mean age similarly showed a progression, beginning at Stage 0 (x̄ = 8.38 years, SD = 5.83) and culminating at Stage 3 (x̄ = 22.76 years, SD = 1.66). Stage 0 displayed the greatest age range (0–17 years) and the highest standard deviation (SD = 5.83). The fusion stages showed reduced variability, especially Stage 2 (x̄ = 20.26 years, SD = 2.10) and Stage 3 (x̄ = 22.76 years, SD = 1.66), indicating a more consistent age of maturation. The age distribution across stages is visualized in Figure 4.
Stage-wise Age Distribution of Females.
Interobserver reliability was calculated using Cohen’s κ, which amounted to 0.82, indicating near-perfect agreement. Spearman’s correlation (ρ) was calculated between the fusion scores and the chronological age. Statistically significant correlation (p < .001) was observed in both sexes, with ρ = 0.819 in males and ρ = 0.797 in females. Using the Mann-Whitney U test, sex differences were assessed, and these were found to be statistically significant (Z = 4.84; p = .001). However, the magnitude of this difference (effect size: 0.22) is relatively small. Linear regression models were generated using the medial clavicular epiphyseal fusion score of the left clavicle for both males and females as:
Where SF is the stage of fusion.
The generated regression equations were validated on 50 cases (25 males and 25 females) by quantifying the mean deviation and mean absolute error (MAE). The MAE of the males was 1.36, the MAE of females was 1.88, and that of combined males and females is 1.62 (Table 2).
Mean Difference and Mean Absolute Errors Calculated After the Application of the Proposed Regression Model on a Test Set.

Discussion
The need for novel methods of age estimation and refining the existing criteria is increasing in forensic practice. Most law enforcement agencies seek the opinion of forensic pathologists for age estimation in both living and dead bodies or skeletal remains. This is especially common in developing and underdeveloped countries where the rate of institutional births is relatively lower. Disputes regarding age occur most commonly in respect of criminal and civil responsibilities, which vary in every country. In India and most other countries, the age of 18 is considered a cut-off where individuals attain legal adulthood, civil rights and liabilities, and criminal responsibility. Hence, in age estimation scenarios, the forensic pathologists require reliable criteria to assert the age range in the later stages of the second decade. Nevertheless, multiple researchers have defined criteria for estimating age from ossification centers of the medial end of the clavicle; the geographical variation in anthropological studies should also be accounted for. 1 The present study is focused on addressing the reliability of existing criteria of age estimation using ossification of the medial end of the clavicle in the native Indian population. Radiological techniques such as X-ray, CT, and MRI are preferred tools for age estimation in both living and the dead. Computed tomography with minimal slice thickness is the preferred tool in current age estimation scenarios. Wittschieber et al recommended using <1 mm slice thickness in CT for evaluation of the medial ends of the clavicle. The present study has also used CT scans of 1 mm slice thickness to determine stages of ossification. 7
The present study adopted a simplified four-stage classification (Stages 0–3) to ensure high interobserver reliability and consistency, given the retrospective nature and standardized CT parameters. Effectively, it is a pragmatic modification of the widely used Schmeling five-stage classification (Stages 1–5) and the even more granular Kellinghaus nine-substage system, both of which are central to the guidelines of the Arbeitsgemeinschaft für Forensische Altersdiagnostik (AGFAD). 8 Our Stage 3 (“Complete fusion of the epiphyseal ossification center with diaphysis; epiphyseal scar might still be appreciable”) effectively consolidates the final stages of complete fusion (Schmeling’s Stages 4 and 5: complete fusion with scar present and complete fusion with scar obliterated, respectively). While this simplification facilitated near-perfect interobserver agreement (κ = 0.82) and robust age estimation, it is noted that the exclusion of the final stage differentiation (Schmeling Stage 5) and the exclusion of Kellinghaus’s sub-stages (e.g., subdivisions of partial fusion/Stage 2) represent a trade-off. The more granular stages (Schmeling 4/5, Kellinghaus 3c) are specifically designed to increase precision when assessing the critical legal age thresholds of ≥18 and ≥21 years. The minimal slice thickness used in our study (≤1 mm) supports high-resolution assessment, which is necessary for applying these sub-stages, but we prioritized the established four-stage classification for broad applicability across our large sample. Future work could specifically evaluate the utility of the Kellinghaus sub-stages on our data to determine if they provide a significant improvement in the MAE for age prediction in this population.
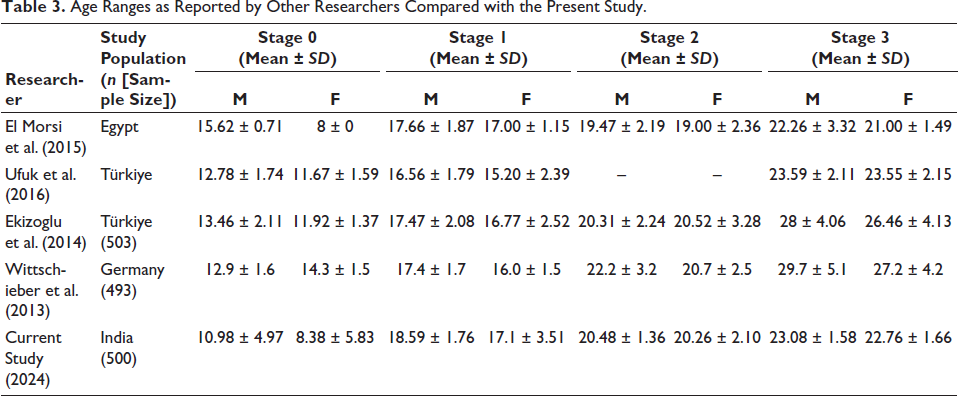
In our study, the mean age of Stage 0 for males is 10.98 (±4.97), and that of females is 8.38 (±5.83). These values are considerably lower than the age ranges reported by other researchers; Ufuk et al from Türkiye (males: 12.78 ± 1.74; females: 11.67 ± 1.59), Ekizoglu et al. from Türkiye (males: 13.46 ± 2.11; females: 11.92 ± 1.37), El Morsi et al. from Egypt (males: 15.62 ± 0.71; females: 8 ± 0) and other studies.9–12 However, in Stage 0, the age range of females in this study (8.38 ± 5.83) is almost similar to the findings of El Morsi et al. This difference can be explained by the variations in the lower age limits and the variable sample population in the lower ages. In our study, 37 cases were included in the under-10 age group, which is significantly higher than in other studies. The sample size has also been kept at a much higher level so as to reduce the overcrowding of samples in any specified age category. This also explains the high standard deviation restricted to Stage 0, while the SD in other stages is almost concordant with results reported by other researchers. Based on our study, the fusion patterns of males and females were distinct from birth to 25 years of age. Ekizoglu et al. reported significant differences between males and females in Stage 1 and Stage 4. In contrast, we observed significant differences between sexes only in Stage 1. Table 3 shows the comparison of age ranges of different stages in different populations. 13
Age Ranges as Reported by Other Researchers Compared with the Present Study.
The regression equations can effectively age individuals with remarkable accuracy. The overall trend shows that the regression equation shows a tendency to underestimate actual age, with error rates particularly higher for females. The MAE of females (1.88) is considerably higher than that of males (1.36), which is almost similar to the pattern reported by Shedge et al. However, the combined MAE in this study is slightly higher than that of Shedge who also studied the Indian population.
Tozakidou et al. recommended the acquisition of CT scans in an arms-up position, as it decreases the patient dose (dose of X-rays required for penetrating the body) and provides better image quality. 4 Such dose regulations are a concern in clinical age estimation scenarios, which do not bother forensic age estimation practices using PMCT. Though scan parameters were specified in our study, no attempts were made to reduce the effective dose (CTDI/DLP) as obtaining high-resolution images was the only objective. Considering the AGFAD, (Study Group on Forensic Age Diagnostics) recommendations in the context of forensic age estimation, four parameters were implemented: (a) Schmeling et al main stages (though Stage 5 was not included separately); (b) utilizing ≤ 1 mm CT images; (c) using axial/coronal reformats; and (d) using bone window for interpretation. Kellinghaus et al. sub-stages could not be included in this study. Ruder et al. stated in their systematic review that patient position on the CT table and CT scan parameters were often heterogeneous and incomplete in the literature. To support further reviews, all the scan parameters and CT acquisition technique are specified in the present study. 14
Conclusion
This study successfully investigated the fusion patterns of the medial clavicular epiphysis in a large North Indian cohort (n = 500) using PMCT. We observed distinct and predictable fusion patterns between males and females from birth to 25 years of age.
The fusion scores demonstrated a statistically significant, strong correlation with chronological age for both sexes, with Spearman’s ρ coefficients of 0.819 for males and 0.797 for females. Despite the presence of statistically significant gender differences in fusion timing, the small effect size (0.22) implies a minor practical influence on the age estimation outcomes. The derived linear regression models for age prediction proved to be highly reliable, yielding low MAEs of 1.36 years for males and 1.88 years for females. These MAE values underscore the reliability of medial clavicular epiphyseal fusion as a key forensic age marker in the North Indian population. In summary, the research provides a region-specific and gender-based tool for age estimation, emphasizing the crucial need for population-specific criteria in forensic contexts.
Footnotes
Authors’ Contribution
Dr. Balaji. D: Conceptualization, methodology, writing-original draft, visualization. Dr. Zahid Ali CH: Conceptualization, formal analysis, validation, writing-original draft. Dr. Gokul. G: Conceptualization, methodology, writing-original draft, visualization, formal analysis. Dr. Abilash Srinivasa Murthy: Methodology, writing-original draft, visualization. Dr. Raveena Divya: Visualization, validation. Dr. Swati Tyagi: Visualization, validation. Dr. Abhishek Yadav: Resources, supervision. Dr. Sudhir K Gupta: Resources and supervision.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for Publication
Consent for participation in the study and publication was obtained from the first-degree relatives (legal heirs) of all subjects.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Informed Consent
The ethical clearance was granted by the All India Institute of Medical Sciences Institutional Ethics Committee (IEC 577/02.11.2018, RP-29/2018).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.