
Abstract
Age estimation is vital in medico-legal and forensic contexts, particularly in developing countries like India, where reliable birth documentation is often lacking. Accurate age determination supports legal decisions in criminal responsibility, marriage eligibility, civil rights, and identity verification. This study aimed to assess skeletal maturity through radiological evaluation of epiphyseal fusion in the humeral head, iliac crest, and ischial tuberosity among individuals aged 16–21 years in south-east Rajasthan. An observational, cross-sectional study was conducted at Jhalawar Medical College’s Department of Forensic Medicine, including 100 individuals (67 males, 33 females) aged 16–21 years. Participants underwent clinical and radiological examinations, with digital X-rays of the shoulder and pelvis analyzed for epiphyseal fusion by a blinded radiologist. Data were statistically analyzed using Microsoft Excel and relevant software tools; p < .05 was considered significant. Radiological findings demonstrated progressive fusion with age. In females, complete humeral head fusion was observed in all individuals aged 20–21, with an overall 60.61% showing complete fusion. The iliac crest and ischial tuberosity showed 30.30% and 21.21% complete fusion, respectively. In males, humeral head fusion was complete in 77.61% overall, including all those above 18. Iliac crest and ischial tuberosity fusion were complete in 47.76% and 37.31%, respectively. Fusion occurred earlier in females across all sites. The study confirms a consistent and age-progressive pattern of epiphyseal fusion, with earlier completion in females. Radiographic assessment of specific skeletal sites proves to be a reliable method for age estimation, particularly valuable in the 16–21-year age group in medico-legal investigations.
Keywords
Introduction
Age estimation plays a pivotal role in personal identification in both civil and criminal proceedings, especially in developing countries like India, where birth records are often unreliable despite laws such as the Registration of Births and Deaths Act of 1969. Accurate age determination is essential in legal matters involving criminal responsibility, civil rights, and marital eligibility. 1
Various methods are employed for age estimation, including general appearance, dental, and skeletal examinations. While general appearance and body measurements are unreliable due to individual variations, and dental data is limited after the eruption of most teeth by age 16, skeletal examination stands out as the most systematic and legally accepted approach. Radiological assessment of bone ossification, particularly epiphyseal union, is widely recognized for its accuracy. 2
Key skeletal markers such as the ischial tuberosity and iliac crest are significant for determining the legal age for marriage in India—18 years for girls and 21 years for boys. These indicators are also valuable in resolving civil and criminal cases involving property disputes, passport verification, insurance claims, disputed identity or sex, and missing persons. For individuals above 16, radiographic analysis of the pelvis and shoulder bones becomes crucial. 3
Ossification timing varies due to climate, heredity, race, nutrition, and socioeconomic factors, necessitating population-specific studies. earlier bone union in Indians than in Western populations, highlighting regional differences. 4 The ischial tuberosity, maturing post-18 years, serves as a reliable marker in legal assessments. The constancy in ossification age makes epiphyseal union a dependable legal standard, with faster fusion observed in females and in tropical regions. 5
Modi’s textbook emphasizes that regional differences within India complicate the establishment of uniform age standards. Reddy KSN noted earlier epiphyseal union in females, whereas skull sutures close more slowly. Radiology remains a reliable method for tracking ossification progression until full skeletal maturity. 6
Materials and Methods
Study Overview
This observational, cross-sectional study was conducted at Jhalawar Medical College’s Forensic Medicine Department with radiological support. After receiving ethical approvals, around 100 individuals aged 16–21 were enrolled. Participants included patients visiting the hospital for treatment or routine check-ups and students undergoing medical examinations. The study aimed to assess age-related parameters through radiological evaluation.
Inclusion Criteria
Only individuals aged between 16 and 21 years from south-east Rajasthan were included. Participants had to possess valid age proof, such as a birth certificate or matriculation certificate issued by a competent authority and must have given informed consent.
Exclusion Criteria
Subjects were excluded if they lacked valid age proof, were outside the 16–21 age range, or had severe malnutrition, chronic illness, endocrine disorders, or deformities in limbs or pelvis.
Data Collection Method
Written informed consent was obtained from all eligible participants. A general physical examination was performed to evaluate overall health and rule out deformities. Only those meeting the inclusion criteria and not meeting the exclusion criteria proceeded to the next stage of the study. All the eligible students who came for a routine check-up were sent for radiological examination after explaining the complete process and obtaining consent.
Materials
The study utilized X-ray films, a view box, a magnifying lens, height and weight measuring machines, and a pre-designed Performa for data recording.
Method
Personal information was documented. Participants were briefed about age estimation and radiation exposure risks. Clinical and dental examinations were conducted, and data were recorded. Digital X-rays of the shoulder and pelvis joints were taken and analyzed by a blinded radiologist to assess ossification center fusion. Findings were compared with existing regional studies.
Statistical Analysis
Data were compiled in Microsoft Excel and analyzed using statistical software, which is age estimation software. Qualitative data were presented in groups and percentages, while quantitative data were expressed as mean and standard deviation. Chi-square tests were used, and a significance level of p < .05 was considered.
Result and Observations
Radiological Age Distribution (in Years) Fusion of Head of Humerus (Female).
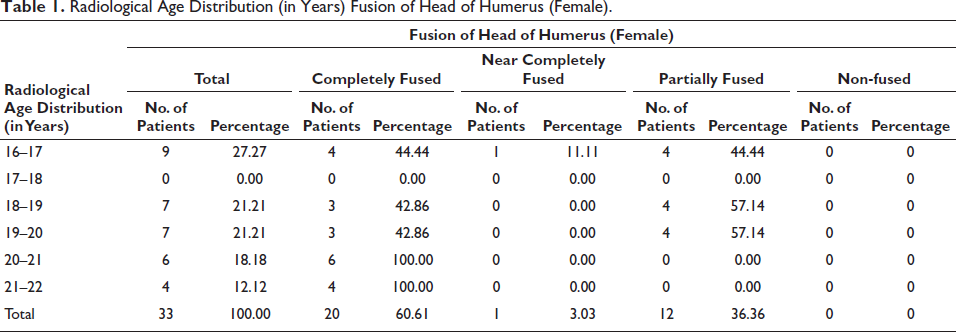
The study analyzed humeral head fusion in 33 females. Complete fusion was seen in 60.61%, partial in 36.36%, and near-complete in 3.03%, with no non-fusion cases. Fusion patterns varied by age: mixed stages appeared in 16–17 years, while from 20 years onward, 100% showed complete fusion. Findings suggest that in females, complete fusion of the humeral head typically occurs between 20 and 22 years of age.
Distribution of Cases According to X-ray Findings.
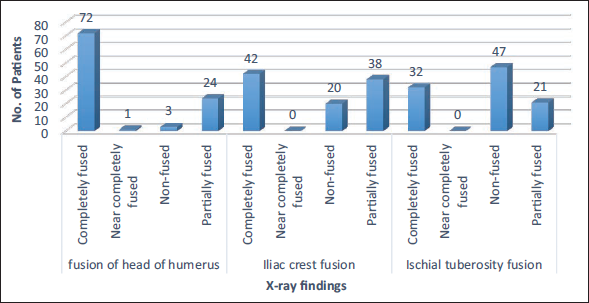
X-ray findings showed complete fusion in 72% (humerus head), 42% (iliac crest), and 32% (ischial tuberosity), with varying degrees of partial or no fusion in the remaining cases across these anatomical sites. The study involved 100 cases with a mean age of 18.31 ± 1.85 years, mostly aged 16–21. Males comprised 67% and females 33%. Among males, most were 16–17 years (44.78%), while among females, 18–19 years (42.42%) was most common. Rural and urban representation was nearly equal (52% vs. 48%).
Radiological Age Distribution (in Years) Based on Iliac Crest Fusion in Female Cases.
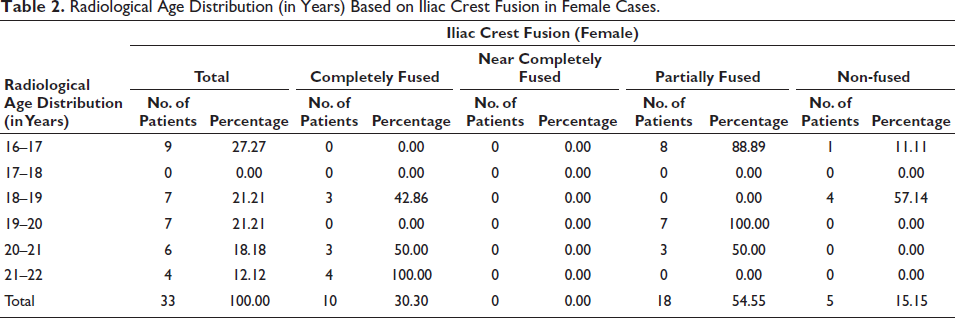
The study examined iliac crest fusion in 33 female subjects. Partial fusion was most common (54.55%), followed by complete fusion (30.30%) and non-fusion (15.15%), with no near-complete cases. In the 16–17-year group, partial fusion predominated (88.89%), with no complete fusion observed. Complete fusion increased with age, appearing in 42.86% at 18–19 years and reaching 100% by 21–22 years. These findings indicate that iliac crest fusion in females typically begins after age 17 and is completed by 21–22 years.
Radiological Age Distribution (in Years) Based on Fusion of the Head of Humerus in Male Cases.
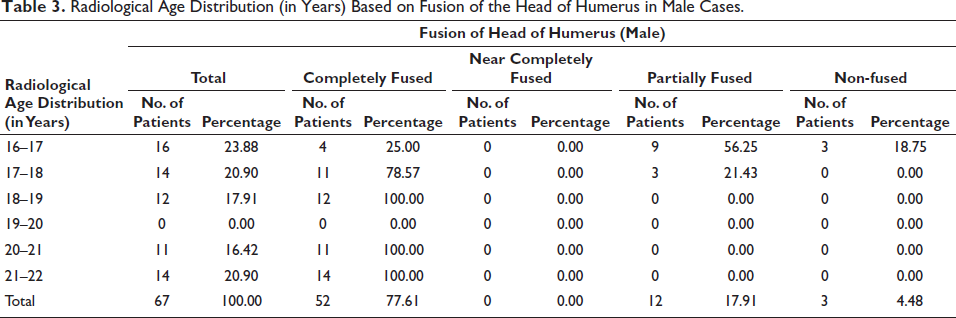
The study evaluated humeral head fusion in 67 males. Complete fusion was found in 77.61%, partial fusion in 17.91%, and non-fusion in 4.48%, with no near-complete cases. At 16–17 years, most had partial (56.25%) or no fusion. Fusion increased significantly at 17–18 years, with 78.57% complete. By 18–19 years, 100% showed complete fusion, a trend consistent in older age groups. These results indicate that humeral head fusion in males typically occurs between 17 and 19 years of age.
Radiological Age Distribution (in Years) Based on Iliac Crest Fusion in Male Cases.
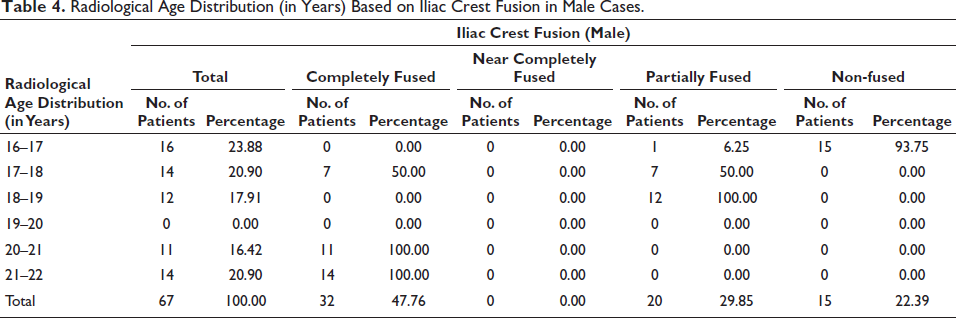
The study examined iliac crest fusion in 67 males. Complete fusion was observed in 47.76%, partial fusion in 29.85%, and non-fusion in 22.39%, with no near-complete cases. Most 16–17-year-olds (93.75%) showed non-fusion. Fusion advanced at 17–18 years, with equal cases of complete and partial fusion. At 18–19 years, all had partial fusion. Complete fusion was universal from age 20 onward. These findings indicate iliac crest fusion in males typically starts after 17 years and is completed by 20–22 years.
Radiological Age Distribution (in Years) Based on Ischial Tuberosity Fusion in Male Cases.
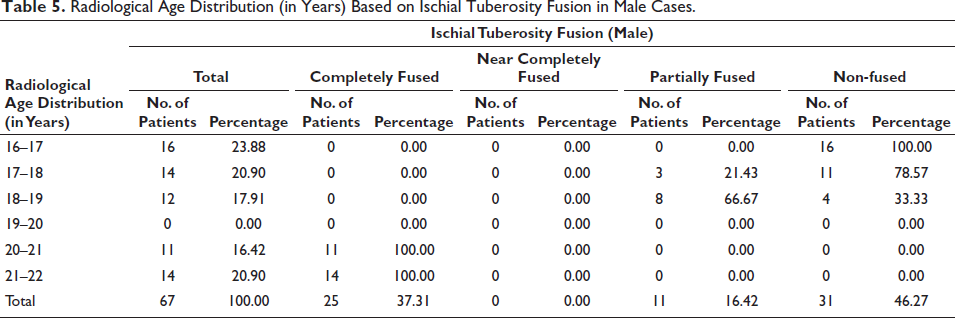
The study assessed ischial tuberosity fusion in 67 males. Non-fusion was most common (46.27%), followed by complete fusion (37.31%) and partial fusion (16.42%), with no near-complete cases. At 16–17 years, all showed non-fusion. Fusion activity began at 17–18 years, increasing at 18–19 years, with 66.67% partially fused. Complete fusion was observed in all individuals by 20–21 years and beyond. These results indicate that ischial tuberosity fusion in males typically begins after 17 and completes by age 20.
Discussion
Among 33 female subjects, complete humeral head fusion was seen in 60.61%, partial in 36.36%, and near-complete in 3.03%, with no non-fusion cases. Fusion stages were mixed at 16–17 years, while partial fusion predominated at 18–20 years. From 20 years onward, all showed complete fusion, indicating typical fusion completion between 20 and 22 years. In a similar study, Dalal D et al. 7 reported that the femoral head in females typically began to appear around age 8, with six early cases noted. By age 12, approximately 70% (21 cases) had visible ossification centers. The onset of fusion occurred near age 13, although the majority of cases remained in the “fusion not started” stage (62%) or the “fusion in progress” stage (28%). As age advanced, particularly after 16 years, a noticeable increase in complete fusion was observed, with several cases reaching full fusion by age 17. Likewise, Shivkumar K T et al. 8 documented rapid epiphyseal union at the lower end of the humerus among females. Complete fusion was noted in 100% of cases in the 15½–16, 16–16½, and 16½–17-year age groups, indicating a consistent and early pattern of skeletal maturity. These findings highlight a trend of accelerated and uniform fusion in the humeral epiphysis among females, aligning with the progressive increase in complete fusion observed in the current study.
Radiographic analysis revealed site-specific fusion patterns: the humeral head showed complete fusion in 72%, partial in 24%, no fusion in 3%, and near-complete in 1%. For the iliac crest, 42% had full fusion, 38% partial, and 20% none. At the ischial tuberosity, 32% were fully fused, 21% partially, and 47% remained unfused, with no near-complete cases noted. In a similar study, Naik S et al. 9 reported that none of the participants had visible ossification centers at the outset. As development progressed, early ossification (A stage) was seen in 6.67% of cases, while 20% reached the + stage, and another 6.67% showed partial fusion (++). Altogether, 26.67% attained at least the + stage, but full fusion was not seen in any patient. A significant portion, approximately 66.67%, exhibited either absent ossification or incomplete fusion throughout the study. Likewise, Dalal D et al. 7 observed the appearance of the femoral head in all study subjects, with 60% showing its presence. While some signs of fusion initiation were noted, the majority of cases remained either in the pre-fusion stage (78%) or at the early phase of fusion (11%), suggesting that most participants had not yet reached advanced stages of skeletal maturation.
In 33 female subjects, iliac crest fusion was complete in 30.30%, partial in 54.55%, and absent in 15.15%, with no near-complete cases. Partial fusion dominated at 16–17 years (88.89%), while complete fusion appeared from 18 to 19 years (42.86%). All 19–20-year-olds showed partial fusion. Fusion was evenly split at 20–21 years, and by 21–22 years, all showed complete fusion, indicating fusion typically begins after 17 and completes by 21–22 years. Similarly, Kumar R et al. 10 reported that younger females in the 12–15 years group had no appearance or fusion of the ossification center. Fusion activity initiated in the 16–17 years range, where 88.88% had partial fusion and 11.11% showed complete fusion. The trend of increased fusion with age continued, with 90% of females in the 17–18 group and all in the 19–24 age range achieving complete iliac crest fusion. Their overall findings noted complete fusion in 44.21% of cases, partial fusion in 17.89%, and unfused ossification centers in 24.21%. In a similar study, Singh P et al. 11 analyzed iliac crest fusion across five age groups. Among females aged 16–17 years, 50% had begun but not completed fusion, and 40% showed center appearance without union. By 18–19 years, 70% demonstrated incomplete fusion, and 30% had completed fusion. A marked increase was seen in the 20–21 years group, where 90% achieved full union, followed by 80% at 22–23 years. Complete fusion was universal by 24–25 years, confirming skeletal maturity in the mid-twenties.
Among 67 males, ischial tuberosity fusion was complete in 37.31%, partial in 16.42%, and absent in 46.27%, with no near-complete cases. All 16–17-year-olds were non-fused. Fusion began by 17–18 years (21.43% partial) and advanced at 18–19 years (66.67% partial). Complete fusion was seen from 20 years onward, indicating that fusion typically begins after 17 and completes by age 20 in males. Kumar R et al. 10 found no fusion between 12 and 15 years, with partial fusion in 86.67% by 16–17 years, and complete fusion by 20–21 years. Maqsood M et al. 12 showed 79.51% complete fusion by 22–25 years, with an average age of full fusion at 21.52 years. Naik S et al. 9 noted ossification beginning at 15–16 years, with partial fusion by 16–17 years. Dalal D et al. 7 observed fusion activity starting around 12 years, with most individuals remaining in early stages until later adolescence. Shivkumar K T et al. 8 reported complete fusion by 16½–17 years, further confirming the trend of advancing ossification with age.
Conclusion
The study reveals a consistent age-related epiphyseal fusion pattern in the humeral head, iliac crest, and ischial tuberosity among south-east Rajasthan individuals. Fusion occurs earlier in females, especially in the humeral head. The iliac crest and ischial tuberosity exhibit gradual fusion in both sexes, typically completing in the early twenties. Radiographic evaluation proves reliable for age estimation in forensic and medico-legal settings. Gender differences and regional variations are important factors in interpreting skeletal maturity accurately.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was ethically cleared by IEC, Jhalawar Medical College, Jhalawar & Associate Hospital, Jhalawar vide letter no 39 dated June 11, 2024.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable.