
Abstract
Electrocution injuries are associated with high morbidity and mortality, most deaths occurring instantly due to cardiac arrhythmias or respiratory arrest. Delayed deaths and rare organ complications are seldom reported in the literature. We present a case of a 70-year-old woman who survived for five days following an accidental domestic electrocution and subsequently died due to interstitial pneumonitis (IP) and renal tubular necrosis. This case highlights the unusual pulmonary sequelae of electrocution and underscores the importance of meticulous histopathological examination in forensic practice.
Introduction
Determining the cause and manner of death is the critical role of the forensic expert, aiding investigating authorities in distinguishing between natural and unnatural deaths. Electrical injuries, though uncommon, carry high morbidity and mortality with a unique pathophysiology. They may result from lightning, high-voltage, or low-voltage currents, producing manifestations from transient tingling to fatal arrhythmias.1–4
In India, 9,986 electrocution deaths were reported in 2015 (NCRB). Approximately 1,000 deaths and 3,000 burn-centre admissions occur annually due to electrical injuries, with up to 40% of serious cases proving fatal. 5 Around 20% of injuries occur in children, mostly from household appliances and outlets, while workplace exposures remain the fourth leading cause of occupational traumatic death.
Common causes of death include ventricular fibrillation, respiratory paralysis, cerebral anoxia, burns, or secondary trauma. 6 Intestinal perforations, along with necrosis of the intestines and arteries, are considered to be more frequent complications of electrocution.6–8 Wanton et al. (1988) also showed the incidence of myocardial infarction subsequent to electrocution. 9 In addition, Sprecher et al. showed the rupture of an intracranial aneurysm as a complication of electrocution. 10 Sparse literature exists on the studies determining the changes in organs in electrocution deaths. 11 However, pulmonary sequelae like interstitial pneumonitis (IP) are rarely reported. This prompted us to present this case, where delayed fatality occurred due to pulmonary and renal complications of electrocution.
Case Report
A 70-year-old female accidentally sustained an electrocution injury while doing cleaning work at her home when she held a live wire with her right hand on 19 March 2016, at 06
On External Examination
Injuries were as follows: (a) Electrocution injury with crater formation present over the proximal and distal phalanx of the right thumb measuring 3 cm by 1 cm, suggestive of an entry wound (Figure 1). (b) Electrocution injury with blackening evident over the distal phalanx of the right index finger measuring 1 cm × 1 cm suggests an entry wound (Figure 1). (c) An electrocution injury with flattening of skin creases, hard to touch, measuring 2 cm by 1.5 cm, was present over the proximal phalanx of the right middle finger, palmar aspect, suggesting an entry wound (Figure 1). Electrocution injury present over the left heel measuring 3 cm × 2 cm, area hard to touch, pale, flattening of skin creases present associated with the surrounding area showed a hyperaemic border suggestive of an exit wound. Internal examination showed that the brain was markedly congested and oedematous, the lungs were congested and oedematous, and other organs were congested. The samples from various organs were preserved for histopathological examination. Histopathological findings: The cerebrum showed hypoxic changes. The lung showed a feature of IP with areas of pulmonary haemorrhage (Figure 2). The kidney showed focal tubular necrosis (Figure 3). Skin from the heel epidermis lining was not seen; sub-epithelial tissue showed few congested vessels. No abnormality was detected in the heart. Opinion as to the cause of death was furnished as IP, and tubular necrosis of the kidney as sequelae and complications of electrocution.
Photograph of an Electric Entry Wound as a Joule Burn (Arrow) Present Over Palmer Aspect of Right Hand.

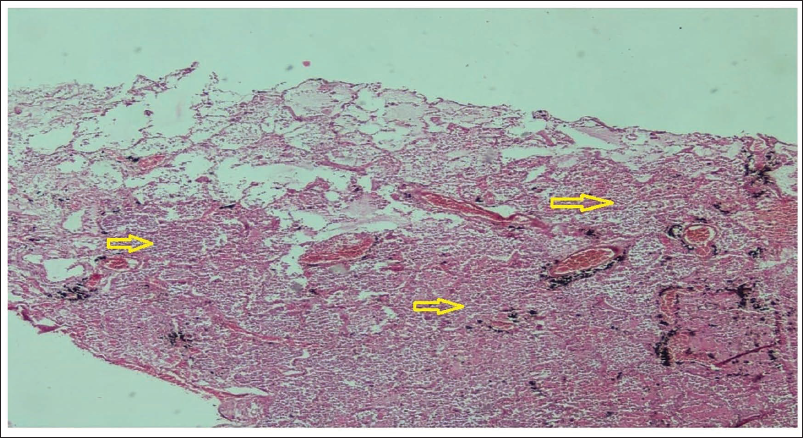
Microscopic Image of Lung Tissue Showing Interstitial Pneumonitis (Arrow) with Areas of Pulmonary Haemorrhage.
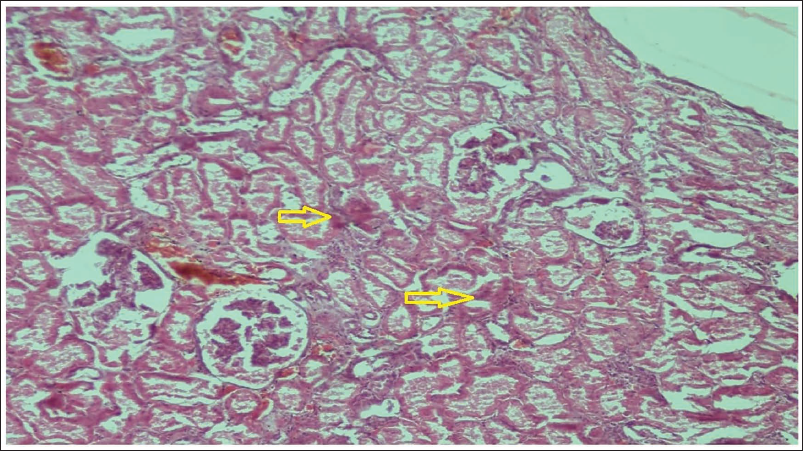
Microscopic Image of Kidney Tissue Showing Renal Tubular Necrosis (Arrow).
Discussion
Since the advent of electricity, both fatal and non-fatal injuries due to electrocution have increased.12, 13 Immediate deaths usually result from cardiac arrhythmias (especially ventricular fibrillation when current traverses the thorax) or respiratory arrest due to brainstem involvement. 6 Joule burn is considered to be a very specific and diagnostic finding of death due to electrocution seen at the site of contact with a live electric conductor. These are round or oval-shaped craters and have a ridge of skin about 1-3 mm in the whole circumference or part of the circumference. 6
Delayed fatalities occur in 7%–22% of cases, commonly from sepsis, haemorrhagic shock, anoxic encephalopathy, or multisystem failure. Pulmonary involvement is seldom described.14–16
IP refers to inflammation of the lung interstitium, usually linked to autoimmune disorders, environmental toxins, radiation, or drugs. Acute IP is rare and often fatal. Global incidence of ILD ranges from 1 to 31.5 per 100,000 person-years, with hypersensitivity pneumonitis forming nearly 47% of Indian cases. 17 Throughout the world, the relative frequency of connective ILD reported an enormous variation, with the least in Belgium (7.5% of cases) and greatest in Canada (33.3%) and in Saudi Arabia (34.8%). Pulmonary findings directly caused by electrocution are seldom reported in literature. Though pulmonary contusions can be found due to a fall from heights subsequent to electrocution. 18 Acute IP is considered to be a rare reported disease which is associated with a higher mortality rate. 19
Studies by Masanes, Michui, and Kanchan have reported pulmonary oedema, alveolar haemorrhage, congestion, and mild fibrosis.20–22 Singh et al. documented non-cardiogenic pulmonary oedema in a child. 23 However, IP specifically following electrocution has not been described widely.
In the present case, the victim was previously healthy, with no risk factors for IP (no smoking, toxins, autoimmune disease, radiation, or drugs). The only plausible trigger was electrocution, leading to delayed pulmonary injury and renal tubular necrosis. Thus, electrocution can induce atypical inflammatory responses in the lung parenchyma, culminating in fatal IP.
Most electrocution deaths are immediate; delayed sequelae complicate cause-of-death determination. Absence of classical skin burns can obscure diagnosis, making histopathology vital. Establishing accidental origin influences insurance claims, compensation, and liability.
Conclusion
Electrocution typically causes sudden cardiac or neurological death, while pulmonary complications are rarely encountered. This case documents IP as an unusual, delayed sequela of electrocution, leading to death five days after injury.
Awareness of such complications is crucial for forensic experts, particularly when classical electrical marks are minimal. Histopathology plays a decisive role in attributing death to electrocution in these scenarios. Preventive household electrical safety measures and awareness campaigns remain essential to reduce such avoidable fatalities.
Footnotes
Abbreviations
IP: Interstitial pneumonitis
ILD: Interstitial lung disease
DILD: Drug-induced interstitial lung disease
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
The consent for the study was taken from the participants.