
Abstract
Necrotizing fasciitis (NF) is a rare, fast-progressing soft tissue infection primarily affecting subcutaneous and fascial tissues, with significant risks of morbidity and mortality, including limb loss or death. Early diagnosis is critical but often limited due to the cost and availability of imaging techniques like CT, MRI, and frozen section biopsy. The Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) scoring system, based on routine and widely accessible lab tests, can facilitate early detection and improve outcomes. Our study aims to evaluate the correlation between this scoring system and patient outcomes, including survival, the necessity for surgical intervention, and mortality in cases of NF. This retrospective study analysed patients admitted to a tertiary care center with NF, myonecrosis, cellulitis, or Fournier’s gangrene between September 2018 and September 2023. Case records were reviewed to calculate LRINEC scores, which were compared with treatment outcomes. Patients were categorized into two groups: Survivors and non-survivors. The average LRINEC score was 3.7 ± 1.38 in the survivor group and 8.1 ± 3.2 in the non-survivor group, with a statistically significant difference (P = .003). The findings highlight that higher LRINEC scores are associated with poor outcomes, confirming its usefulness as a diagnostic and prognostic tool. By identifying at-risk patients early, clinicians can initiate timely and appropriate interventions, potentially reducing mortality and improving patient care.
Introduction
A rare yet fatal soft tissue necrosis, necrotizing fasciitis (NF) typically targets the subcutaneous and fascia tissues. Its rate of hospital mortality and morbidity is high. 1
Purpura, subcutaneous hemorrhage, bullae, necrosis, and gangrene are signs of NF. There are about 500 instances of this disease annually, and the mortality rate might reach 40%. 2
In 1783, French physician Claude Colles described NF. NF infection has been classified into two types: Type 1 (anaerobic and aerobic bacterial infection) and type 2 (Staphylococcus aureus and group A beta-hemolytic Streptococcus bacterial infections). 3
NF is a hazardous soft tissue infection that can result in damage to the limb or even death. CT, MRI, and frozen section biopsy can help detect NF early; however, their use is limited by cost and accessibility.
The primary reasons for the high death rates are delayed vigorous surgical debridement and difficulty in detection. Malnutrition, immunosuppression, and diabetes mellitus (DM) are well-known risk factors for developing NF. 4
Broad-spectrum antibiotics, vigorous serial debridement, early diagnosis, and a multidisciplinary critical care strategy are required for NF patients to have successful outcomes. 1 Without an accurate and prompt diagnosis and treatment, the death rate might potentially reach 100%. 1
Finding a quick, validated, and easy-to-use tool at the bedside to quickly classify patients who may have a life-threatening illness is a constant need.
The Laboratory Risk Indicator’s score system for NF makes sense in this way.
Wong and associates created LRINEC in 2004, and it is effective in distinguishing NF from other infections of the soft tissues. Additional research revealed that this score system can be applied to the early detection of NF. 5
The aim of our study is to determine the relationship between this scoring system and the likelihood of survival, the need for surgical intervention, or mortality in patients with NF.
Materials and Methods
Patients admitted to our Tertiary care Hospital from September 2018 to September 2023 (five years) with a diagnosis of NF, Fournier’s gangrene, and cellulitis, which had progressed to NF, were included in our study. The total sample size is 28. The complete case details of each case were gathered from the Department of Medical Records. Since this is a retrospective analytical study, institutional ethics committee ethical approval is not necessary, as it does not involve any investigational procedures of patients.
Our study also included patients who had received surgical debridement in another hospital and were subsequently referred to our hospital for intensive care assistance or follow-up. The study did not include patients whose data could not be accessed and who were absconded against medical advice, and patients with conditions like erysipelas, gas gangrene, pyomyositis, deep vein thrombosis (DVT), and compartment syndrome were excluded from the study.
The scoring of all the patients were calculated using the LRINEC Scoring scale as mentioned in Table 1.
LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) Scoring Parameters.
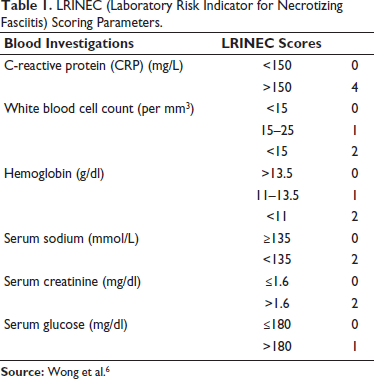
Based on the outcome of their treatments, the total samples were classified into two groups: Living (Group 1) and deceased patients (Group 2). This scoring system analyses the simple six parameters, namely CRP, TLC, Hb, Sr. Na, Sr. creatinine, and blood glucose. If the score is six or higher, NF needs to be taken very carefully. 6 According to validation research, patients with an LRINEC score of ≥6 are more likely to die. 7
A thorough perusal of their case sheets, including basic investigations, was undertaken, to do the LRINEC Scoring for each patient separately.
Following their entry into pre-made forms, the collected data was imported into the SPSS (Version 16, SPSS Inc. Chicago, IL) software. Mann–Whitney U-test was utilized. For statistical significance, a P value of <.05 was considered.
Results
The age range of the study’s patients was 18–72 years old, including 15 male patients and 13 female patients. Patients whose illness/death was suspicious, including death due to NF following trauma, including (road traffic accident [RTA], assault, or machinery injuries), gluteal injections were made as medicolegal cases and if dead, were subjected to autopsy, following which the study was initiated. Regarding average age or gender between the two groups, there was no statistical significance (P = .721 and P = .363, respectively). It was found to be associated with several comorbidities, most of which had a covert or contemporaneous onset, including peripheral vascular dilatation (PVD), chronic kidney failure (CKD), DM, and hypertension. Of these all, DM was found to be the most commonly associated with aggressive disease. A statistically significant difference was not present between the groups (P = .643).
The most common etiological factors were soft tissue infections of the femoral, scrotal, and inguinal areas, which affected ten individuals (35.7%). Four patients (21.4%) got gluteal intramuscular injections for each abscess.
After receiving an intramuscular injection, NF appeared in the gluteal area in four people, two of whom had passed away. At the relatives’ request, an autopsy was performed on two of the patients.
Three patients experienced deep lacerations in their lower leg muscles following accidents; a 22-year-old male patient with orchitis and two middle-aged male patients with perineal apse due to shaving are also presented. A case of HIV positive male patient with development of Fournier’s gangrene, and another three patients had developed NF during the hospital stay following late treatment of snake bite.
In deep tissue culture, the most commonly cultured bacteria were S. aureus, Escherichia coli, Klebsiella pneumoniae, and Pseudomonas aeruginosa. LRINEC score averages were 3.7 ± 1.38 in Group 1 and 8.1 ± 3.2 in Group 2, respectively. Group 2’s (Dead patients) average LRINEC score was noticeably higher than Group 1’s (Live patients) (P = .003).
In five cases, the defects were repaired with a partially thick skin flap. Images of two patients with severe uncontrolled rapidly spreading NF who have died even after surgical debridement are shown in Figures 1 and 2.
Patient 1—Autopsy Image of a Patient Who Died Due to NF Following IM Gluteal Injection, Showing the Extensive Disease of the Left Lower Limb.

Patient 2—Autopsy Image of a Patient Who Died Due to NF Following IM Gluteal Injection Showing Multiple Fasciotomy Wounds.

Discussion
The early skin changes of NF resemble cellulitis or an abscess, making an early diagnosis challenging. Nonetheless, there are a few traits that strongly support the identification of NF from the development of bullae, bleeding beneath the skin, a blood artery thrombosis-related change in skin tone from red to purple to black, and diminished or absent skin sensation due to underlying nerve necrosis. 8
Due to their inability to accurately rule out necrotizing alterations, medical imaging modalities are not very useful in the diagnosis of NF in the early stages of the disease. Every imaging modality has the following restrictions: Ultrasonography—Development of superficial abscess; plain radiography—subcutaneous emphysema; CT scan—Development of abscesses, edema, subcutaneous gas, and fascial thickening. If an MRI reveals fluid accumulation and deep fascial involvement during contrast injection, NF is quite likely to be diagnosed. 9
Broad-spectrum antibiotics that target gram-negative, gram-positive (including MRSA) and anaerobic bacteria could be given early on to halt the infection in its tracks. However, vigorous surgical wound debridement is the standard treatment for NF when the disease progresses.
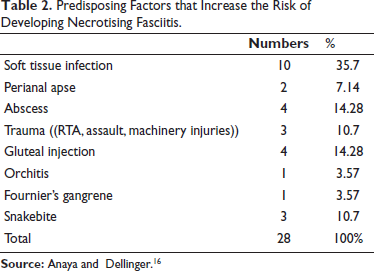
Research indicates that NF is more prevalent in men between the ages of 50 and 60. The patients with NF in our study had an average age of 55.6 years, and our results agree with those of prior studies. Our study shows a predominance of male patients. DM, atherosclerosis, underlying malignancy, chronic kidney disease, and immunosuppression are common co-morbid diseases. seen in NF patients. 10 Other common predisposing factors in our study were trauma, burns, and even following intramuscular injection as mentioned in Table 2.
Predisposing Factors that Increase the Risk of Developing Necrotising Fasciitis.
Two cases of intramuscular injection-induced NF have been subjected to autopsy, as a request from the relatives due to a suspicion of medical negligence against doctors. Hence, this created curiosity in the author to carry out research on NF and its unfavorable effects on doctors, including the medicolegal litigations against the doctors. For the same, right to information (RTI) was filed (Registration No MOHFW/R/E/23/02967/2, DATED 08/10/2023) to study the burden of this condition national wide, only few institutes across India were able to provide exact details required as such, total number of live or dead patients over January 2020 to January 2023, but unfortunately no data concerning trends, preventive measures, any reports, studies or documents related to the causes, trends and preventive measures for NF in India during the specified period, hence this research article was initiated to rule out association between the LRINEC Scoring and the severity of the disease for predicting the disease at early stage, thus reducing the burden of the disease.
Rayamane AP et al. 11 in 2016 found 20 dead cases out of 41 proven cases among 100 medical negligence cases filed against doctors from 2009 to 2013, as well as overall more than 25% of cases were due to a lack of standard care and skill. Rani M et al. 12 in 2016, addressed 4 out of 30 medical negligence cases filed against medical professionals filed during 2001 to 2012 in the consumer forum of Varanasi jurisdiction were administration of wrong injection by Para-medical staff.
Diabetes is not a predictor of death as demonstrated by Kalaivani et al. 13 among 60 patients in succession, which was the same in our study. The amount and type of isolated microorganisms can vary, according to the literature. The most frequent monomicrobial contributions are Streptococcus pyrogens, S. aureus, E. coli, K. pneumoniae, Bacteroides, and P. aeruginosa, and additionally, factors are typically polymicrobial. 14 The most often identified microbiological agent in our investigation was P. aeruginosa, which was also the most prevalent component in the Fustes-Morales A et al. study. 15
Wong et al. Su et al. and Corbin et al.’s research revealed that patients with an LRINEC score of six or higher were at a significantly increased risk of developing unfavorable outcomes including death. According to Clayton et al. younger individuals, who have a BUN of 50 mg/dl or less and do not have active sepsis, have much decreased mortality. According to a validation analysis, patients with an LRINEC score of ≥6 were more likely to die and have an amputation, 7 which is similar to our study findings, which demonstrated that patients with a mean LRINEC value of 3.7 ± 1.38 were alive, but the mean LRINEC score of died patients was 8.1 ± 3.2.
Conclusion
This comprehensive three-year retrospective analysis provides compelling evidence that the LRINEC scoring system is a useful tool for predicting NF, supporting its importance.
The results show that the LRINEC score displayed an admirable level of reliability in detecting cases of NF, providing doctors with a standardized and structured method in the initial evaluation of suspected cases, thereby it can reduce mortality and morbidity as well as improving the quality-adjusted life year QALY and decreases the disability-adjusted life year DALY of any patient.
So, our study concludes that there is a strong association between LRINEC scoring and the severity of NF, which implies that the higher the score is associated with more severe and unfavorable outcomes.
Therefore, its incorporation into clinical practice aids in expediting diagnosis and timely intervention, which is pivotal in the management of this potentially lethal condition. Furthermore, the LRINEC score is a cost-effective and easily applicable tool that can be readily implemented in various healthcare settings. This study reinforces the importance of the LRINEC scoring system as an essential component in the diagnostic armamentarium for NF, providing clinicians with a reliable and efficient means of identifying this critical condition.
Footnotes
Acknowledgement
The authors express sincere thanks to the faculties and residents of Forensic Medicine & Toxicology, KAHER’s Jawaharlal Nehru Medical College, Belagavi, Karnataka.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.