
Abstract
Palatal rugae are distinctive to an individual and likened to finger patterns in forensic Medicine. It is known as Palatal rugoscopy or Palatoscopy, which helps to establish the victim’s personal identity when there is an existing antemortem record. Our study aims to determine the predominant palatal rugae configurations in the children and adolescent age group population of the Southern part of India and to assess the gender-wise differences. One hundred and twelve subjects were included according to the inclusion criteria, excluding subjects with previous orthognathic or palatal surgery histories. Alginate impression material was utilized for making maxillary impressions and study models were obtained using green and yellow dental stone material. Rugae patterns were marked and Trobo’s classification was utilized to identify rugae patterns. The recorded data were studied using SPSS statistical software, version 20.0. Among 112 subjects, wavy, diverging and straight were the most predominant palatal rugae patterns observed. Under males, the most dominant pattern identified was circular, converging and straight, whereas, among females, curved, wavy, and diverging were the most common. The frequent rugae patterns detected in our study were wavy, diverging and straight. The present study demonstrated the uniqueness of rugae patterns in different individuals and between genders. Thus, it is a valuable and reliable source of identification, provided when antemortem records are available.
Highlights
Palatal rugae patterns can also help to discriminate between twins.
Gender identification can be made by studying the palatal rugae pattern.
The study of palatal rugae patterns can also serve as proof of the identity of edentulous people.
Introduction
Palatal rugae are distinctive to an individual and have been compared with finger patterns in forensic science.1, 2 It is also called as rugae palatine or plica palatine transverse, which denotes the ridges on the anterior palatal mucosa behind the incisive papilla on each side of the median palate. 3 Identification of the victim is a primary goal of forensic science. Proper identification of the deceased is essential to claim death certification and for personal, social, and legal reasons.
Recognition of individuals by visual identification and fingerprint comparison is limited by postmortem alterations associated with time duration, temperature and moistness. 4 Due to their internal position and shelter provided by the mucosa of lips, cheek, the buccal pad of fat, teeth, tongue, and surrounding bone, palatal rugae are protected from accidental trauma and elevated temperatures and withstand postmortem barriers.5–7 Thus, palatal rugoscopy or hard palate anatomy helps to establish the victim’s identity. 8 Due to their significant landmarks, palatal rugae are vital in clinical dentistry, like prosthodontics and orthodontics. It is also utilized in various fields, such as anthropology, comparative anatomy, forensic odontology and genetics. However, it is essential in forensic identification only when ante-mortem information, such as dental records, model casts, or digitalized rugae patterns, is accessible for comparison.9, 10
A study in 1978 by van der Linden proved that the palatal raphe does not change in length after 10 years of age. 11 Even in the case of twins, studies have indicated that the palatal rugae patterns are alike but not identical. 12
Palatal rugae patterns are a reliable forensic identification parameter due to their distinctiveness, postmortem alteration resistance, stability, and inexpensive methodology. 13
Although a considerable amount of literature exists, only a few data are available among the Southern Indian Pediatric age group population. Therefore, the present study aimed to delineate different types of rugae to see if there is any gender difference in rugae pattern and their prevalence in the pediatric age group population in Southern India.
Methodology
The impression was taken in pediatric patients after obtaining consent from the parent/guardian/legal authority. They were also requested to fill out a proforma, including age, sex, date of birth, native place, history of orthodontic treatment, orthognathic surgeries, congenital anomalies, palatal surgeries, etc. The participants who qualified for the selection criteria were enrolled in the study group. The patients who reported a previous history of orthodontic or orthognathic treatment, palatal surgeries or congenital anomalies/malformations were excluded from the study participants. Four male and four female candidates in all age categories were selected for the study.
The participants were examined clinically, and an appropriate perforated metal tray (ETN, Germany) was selected for the maxillary arch and palatal prints were obtained. The Alginate impression was mixed and loaded in the selected tray. A small amount of alginate was placed firmly against the rugae in the palate after drying with cotton. The participant’s palatal prints were then registered with minimal pressure to avoid distortion. The impression is washed under tap water to remove debris and disinfected by immersing in sodium hypochlorite (1% NaOCl) for half an hour. The impressions were then allowed to dry naturally. Type III dental stone was mixed and poured using the vibrator. The set cast was removed from the tray and assessed for distortion and air bubbles. All the casts were made free of air voids and bubbles, especially at the anterior one-third of the palate. If distorted and air bubbles were present, a fresh impression or model was made. Thus, maxillary study models were obtained and numbered accordingly on which to place the Calcorrugoscopy for interpretation.
The elevations on the cast were highlighted by a sharp graphite pencil (2 HB) under adequate brightness and magnification loop (2.5× Keeler, Britain) (Figure 1). The highlighted rugae were interpreted on the study cast according to Trobo’s classification (Figure 2). The data was recorded in separate data sheets and the association between rugae shape with ethnicity and gender was evaluated by statistical analysis using SPSS statistical software, version 20.0.

Maxillary Study Model with Palatal Rugae Patterns.

Results
The current study evaluated the shape of palatal rugae distributed among the pediatric population and determined the dominant rugae pattern among genders.
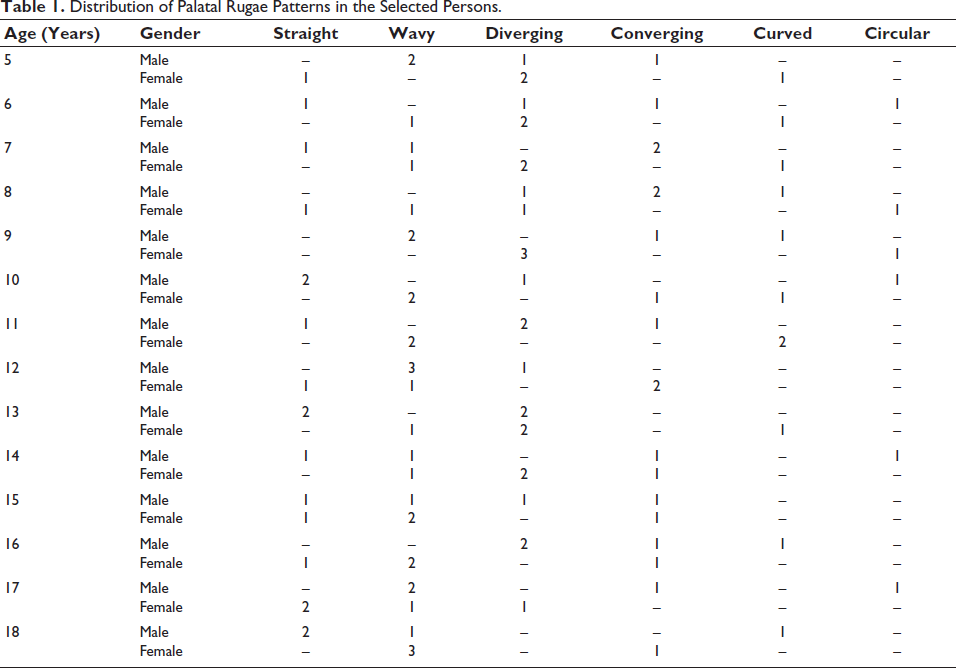
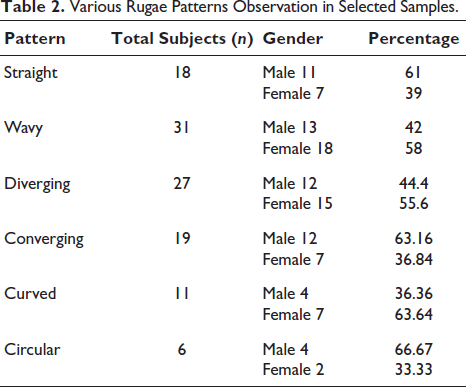
Table 1 shows the distribution of samples. Our study included eight persons under each age category from age 5 to 18, out of which four were male and the remaining four were female. Table 2 shows a wavy (n = 31) pattern as a predominantly observed type of palatal rugae, followed by diverging (n = 27), straight (n = 18), converging (n = 19), curved (n = 11), and circular (n = 6).
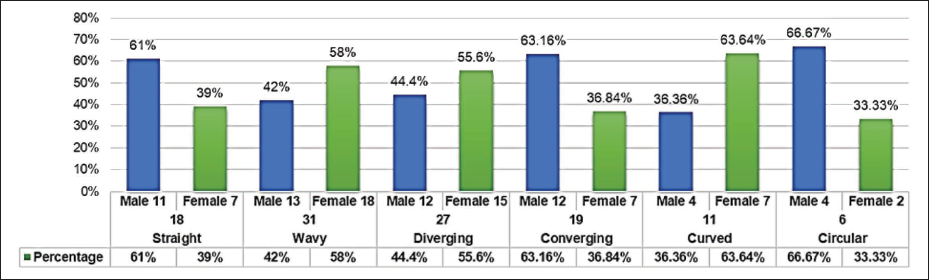
Among 31 subjects with a wavy pattern, 13 were male and 18 were female. Likewise, among 27 subjects with diverging patterns, 12 were male, and 15 were female (Figure 3).
Distribution of Palatal Rugae Patterns in the Selected Persons.
Various Rugae Patterns Observation in Selected Samples.
Graphical Representation of the Presence of Various Palatal Rugae Among Children and Adolescent Age Groups of Tamil Nadu State Population.
Our study concluded that among 112 subjects, wavy, diverging and straight are the most frequently observed palatal rugae patterns. Under males, the most common pattern identified was circular, converging, and straight, whereas curved, wavy and diverging were the most common among females.
Discussion
Forensic dentistry is a branch that involves odontological evidence, that is, soft tissues and hard tissues, antemortem and postmortem records in establishing identity. Palatal rugae develop as localized regional epithelial thickenings and proliferation in the hard palate. The orientation and forms of palatal rugae are governed by the core fibers running antero-posteriorly in concentric rings below each rugae. Among the oral soft tissues, palatal rugae have significant distinguishing features as they are unique in their pattern in every individual. 10 Therefore, palatal rugoscopy (rugae pattern analysis) can be used for individual identity by matching postmortem rugae records with antemortem details.
Our study concluded that among 112 subjects, wavy, diverging and straight were the most predominant palatal rugae patterns observed. Under males, the most dominant pattern identified was circular, converging and straight. Furthermore, curved, wavy, and diverging were the most predominant patterns among females.
Studies have been carried out on rugae patterns, pointing out that there are no two similar structured palatal rugae patterns; they do not endure changes except length due to normal growth periods and persist in the same position throughout the patient’s life.
A study by Shetty et al. concludes that the diverging pattern was more common in females than males, which is analogous to the present study. 14 Also, a study by Rajan et al. (2013) concluded that wavy and curve patterns were more predominant in 5–15-year-old children. 15 However, the wavy, divergent and straight rugae were the most commonly observed palatal patterns in the present study.
An observational study by Sumathi et al. (2014) evaluated the uniqueness of palatoscopy in 40 participants between 15 and 25 years and concluded that wavy patterns were observed to be more predominant, followed by straight, curved and circular patterns. 16 However, the present study concludes that the curved and wavy pattern predominantly occurs in females. Palatal rugae patterns show specific associations with racial and geographical variations and are also applicable for gender differentiation.17, 18
Shubha et al. (2013) stated that the number of palatal rugae was slightly more in South Indian females than males, while North Indian men had more rugae than their counterparts. 18
Therefore, it can be proposed that certain rugae structures are specific and distinctive to a particular population. We believe that rugae shape is genetically controlled. Hence, carefully assessed rugae patterns may primarily be used in forensic identification. 19
Limitations
The small sample size limited the present study. Further research should be conducted on a larger population to validate the findings. Evaluation of other geographical regions would give a better appreciation of ethnic variations. A databank for securing the palatal rugae patterns needs to be established. The stored anterior palatal patterns may serve as ante-mortem records, which could be used in the victim’s identification processes.
Conclusion
The predominant rugae patterns in the present study were wavy, diverging and straight. The dominant pattern in males was circular, followed by converging and straight. The frequently identified female rugae pattern was curved, followed by wavy and diverging. The present study demonstrated the distinctiveness of rugae patterns in different individuals and between genders. Thus, it is a valuable, reliable source of identification, provided when antemortem records are available.
Author Contribution
CK and KM: Conceptualization. CK: Methodology. CR: Validation. SR and IB: Formal analysis. KC: Investigation. KC and KM: Resources. Original draft preparation: Writing. All: Review, editing, and supervision. All the authors have read and finalized this version of the present manuscript.
Footnotes
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
The present study was carried out as a prospective observational methodology after obtaining prior ethical approval from the Institutional Ethical Committee of Sree Balaji Dental College and Hospital, Chennai, India. (No. SBDCECM104/13/04). The impression was taken in pediatric patients after obtaining consent from the parent/guardian/ legal authority.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article. It was self-funded by the authors.