
Abstract
Fatal road traffic accidents (RTA) have emerged as a major public health problem in the modern era. The present study conducted over a period of one year besides focusing on the demographic and medical aspects of head injuries due to fatal RTA is unique in sketching a pattern of head injuries. Males contributed to the majority (84.77%) of RTA while only 92 out of 604 (15.23%) victims were females. The majority of the victims were two-wheeler occupants with a total number of 317 cases (52.48%) who are followed by four-wheeler occupants with a total number of 152 cases (25.17%). The fatal head injury occurred on main road 320 (52.98%) which includes National and State highways, followed by the turning of main road I58 (26.16%). Sixty-three (10.43%) cases out of 604 cases alcohol was a contributory factor for the fatal head injury due to RTA. Extra-cranial injuries and scalp abrasion 594 (98.34%) were found in the majority of fatal head injury cases. Scalp laceration, 563 (93.21%) out of 604 cases, was the second most common extra-cranial injury observed in our study. Subdural haemorrhage 367 (60.76%) is the most common intracranial haemorrhage observed in the present study followed by sub-arachnoid haemorrhage 248 (41.06%) and intra-cerebral haemorrhage 195 (32.28%). The least number of intra-cranial haemorrhages observed was brain stem haemorrhage, that is, 54 cases (8.94%) out of 604 cases.
Introduction
A road traffic accident (RTA) is defined as any collision on the road involving two or more items, at least one of which must be a moving vehicle. RTAs are an unavoidable aspect of modernity. According to the National Adyisory of Neurological Diseases and Stroke Council, 'Head Injury' is a morbid condition arising from large or subtle structural abnormalities in the scalp, skull, and/or the contents of the skull, caused by mechanical forces. The most common cause of death in trauma-related fatalities is head damage. Accidents are considered to occur when there is a state of disequilibrium between man and his environment involving several causal agents. The vast majority of traffic accidents occur on roads, and they are regarded as the most significant issue of our century. It is important to note that when an accident happens in air or rail travel, a thorough investigation is conducted, but this is uncommon in the case of road accidents, even if the number of fatalities and injuries is far higher. On the autopsy table, a minor injury with a seemingly normal appearance may reveal itself as a catastrophic injury. To paraphrase, 'No brain injury is too little or terrible to be hopeless about'. The current research was undertaken with the aforementioned objective using medico-legal autopsies performed at the mortuary of Swaroop Rani Nehru Hospital, Department of Forensic Medicine and Toxicology, M.L.N. Medical College, Prayagraj, U.P.
Materials and Methods
All known fatal RTA cases among dead bodies were brought to the mortuary of Swaroop Rani Nehru Hospital, Prayagraj from 1st April 2021 to 31st March 2022. Cases for this study were selected from the dead bodies brought into the mortuary of the S.R.N Hospital; Moti Lal Nehru Medical College; Prayagraj for medico-legal postmortem examination; from the various police stations of Prayagraj district. A prospective study. All the cases for the present study will be selected from dead bodies brought to the mortuary of Swaroop Rani Nehru Hospital, Prayagraj for medico-legal autopsy examination, were included for the purpose of the study. Dead bodies were brought to the mortuary of Swaroop Rani Nehru Hospital, Prayagraj. All of these subject’s attendants will be interviewed using a structured pre-designed questionnaire, and information regarding preliminary information and data will be sought on that proforma.
Inclusion Criteria
All RTA sustained fatal head injuries cases brought to the mortuary of Swaroop Rani Nehru Hospital, Prayagraj.
Exclusion Criteria
Cases other than RTA and crushed injuries were brought to the mortuary of Swaroop Rani Nehru Hospital, Prayagraj.
Results
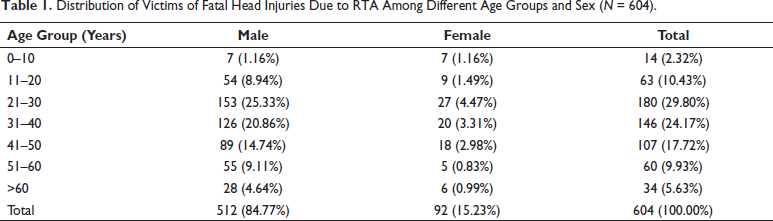
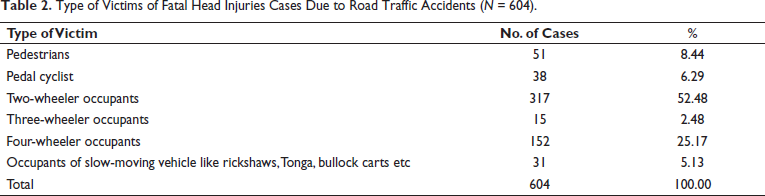
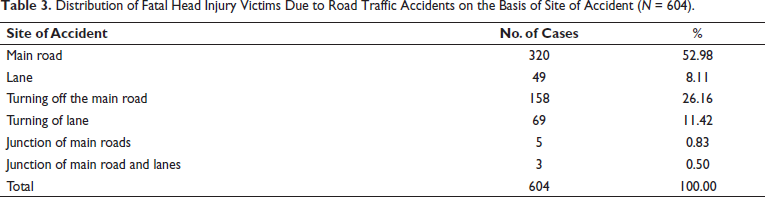
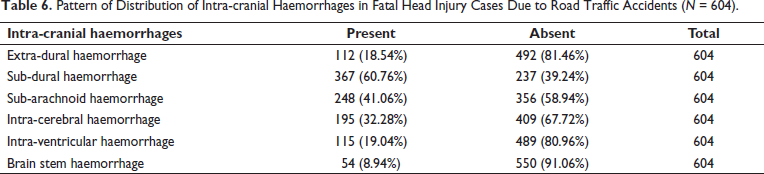
Table 1 shows that males contributed to the majority (84.77%) of RTA while only 92 out of 604 (15.23%) victims were females. It also depicts that the age group of 21-30 years has suffered the highest number of deaths due to fatal head injuries due to RTA 180 (29.80%) followed by the age group of 31-40 years 146 (24.17%) cases. Analysis of the data from Table 2 reveals that the majority of the victims were two-wheeler occupants with a total number of 317 cases (52.48%) who are followed by four-wheeler occupants with a total number of 152 cases (25.17%). Threewheeler occupants were the least victims of fatal head injury due to RTA with only 15 (2.48%) cases. As per Table 3, the majority of the accidents responsible for the fatal head injury occurred on main road 320 (52.98%) which includes National and State Highways, followed by turning of main road 158 (26.16%). The least number of accidents that contributed to fatal head injury occurred in junctions of main roads 5 (0.83%) and in junctions of the main road and lanes 3 (0.50%). Table 4 shows that in 63 (10.43%) cases out of 604 cases alcohol was a contributory factor for the fatal head injury due to RTA. It is observed from Table 5 that among the extra-cranial injuries, Scalp Abrasion 594 (98.34%) was found in majority of fatal head injury cases. Scalp laceration, 563 (93.21%) out of 604 cases, was the second most common extra-cranial Injury observed in our study. The least extra-cranial Injury noted in the present study was scalp contusion, that is, 463 cases (76.66%) out of 604 total cases. Table 6 shows that sub-dural haemorrhage 367 (60.76%) is the most common intra-cranial haemorrhage observed in the present study followed by sub-arachnoid haemorrhage 248 (41.06%) and intra-cerebral haemorrhage 195 (32.28%). The least number of intra-cranial haemorrhages observed was brain stem haemorrhage, that is, 54 cases (8.94%) out of 604 cases.
Distribution of Victims of Fatal Head Injuries Due to RTA Among Different Age Groups and Sex (N = 604).
Type of Victims of Fatal Head Injuries Cases Due to Road Traffic Accidents (N = 604).
Distribution of Fatal Head Injury Victims Due to Road Traffic Accidents on the Basis of Site of Accident (N = 604).
Presence of Contributory Factor (Alcohol) in Fatal Head Injury Victims Due to Road Traffic Accidents (N = 604).

Pattern of Distribution of Extra-cranial Injuries in Fatal Head Injury Cases Due to Road Traffic Accidents (N = 604).

Pattern of Distribution of Intra-cranial Haemorrhages in Fatal Head Injury Cases Due to Road Traffic Accidents (N = 604).
Discussion
In our study (Table 1), the incidence of sex of victims involved in RTA causing fatal head injuries is shown. Males outnumbered females by a very good margin. Males accounted for 84.77% (512 cases) of total fatalities. While for females, this figure was 15.23% (92 cases). Similar studies conducted in the United Kingdom - Kortor JN, et al., 1 (64.50%), and Kumar A, et al., 2 (88.22%), Kaul A, et al., 3 (75.05%) also observed that a maximum number of victims were males which is similar to this study. Also, it was determined that the age group of 21-30 years had the largest number of fatal head injuries due to RTA (180, 29.80%), followed by the age group of 31-40 years (146,24.17%). It demonstrates that the third decade, along with the fourth, is the most susceptible age group for fatal head injury due to RTA.
According to the Ministry of Road Transport and Highways, 4 India’s most exposed road users are walkers, bikers, and two-wheeler riders, who account for around 40% of all deaths. Analysis of data from our study (Table 2) shows that the majority of casualties were two-wheeler occupants with 317 instances (52, 48%), followed by four-wheeler occupants with 152 cases (25,17%). With only 15 (2.48%) instances, three-wheeler riders were the least likely to get a fatal head injury as a result of a collision. Similarly, Mahender, G & S, Thamizharasan, 5 reported 57% of the victims of RTA were of two-wheelers.
In the present study (Table 3), the majority of the accidents responsible for fatal head injury occurred on main roads 320 (52.98%) which includes National and State Highways, followed by turning of main road 158 (26.16%). The least number of accidents that contributed to fatal head injury occurred in junctions of main roads 5 (0.83%) and in junctions of the main road and lanes 3 (0.50%). This finding is in correspondence with Kaul et al. 3 Similarly, Ranjan et al., 6 also noted in their study that 83.05% of the Fatal RTA took place on highways. National highways have been constructed in rural regions in recent times as part of the national highway development programme. People living in this area are not yet adapted to such roads. Many times they are not repaired and fatalities happen on these roads, especially of farmers and pedestrians. Incidence of vehicular accidents on national highways was observed as 56.6%, Kaul A et al. 3 High speed, bad driving, and large vehicles like trucks and swiftly moving two-wheelers may be to blame for the high frequency of fatal head injuries that result from traffic accidents on roads in the Prayagraj area.
A common risk factor for RTAs is drunken driving. In a systematic review done by Das et al., 2012, 2%-33% of the injured and 6%-48% of killed RTA victims had consumed alcohol or drugs. In our study (Table 4), 63 (10.43%) cases out of 604 cases of alcohol were a contributory factor for the fatal head injury due to RTA. It is well proven that drinking impairs a driver’s ability to operate a motor vehicle. Also, impairment increases as blood alcohol concentration rises. In addition, the risk of accidents is greater for younger and older drivers with the same blood alcohol concentrations (WHO, 2020). 7 Drunk driving is well acknowledged to be very risky. The more alcohol in a person’s bloodstream, the more severe the consequences of intoxication and the greater the risk of accident. In the current study (Table 5), scalp abrasion 594 (98.34%) was present in the vast majority of instances of fatal head injury. Scalp laceration was the second most prevalent extra-cranial injury seen in our study, accounting for 563 (93.21%) of 604 cases. Scalp contusion, with 463 instances (76.66%) out of 604 total cases, was the least prevalent extracranial injury seen in this study. Similar to Ranjan et al. 6 it was observed that in 86% of instances, abrasions were seen, followed by lacerations in 75% of cases and contusions in 58% of cases. They also noted that abrasions constituted the highest percentage (86%) of all injuries amongst motorbikes as the victim was dragged on the road in roadside accidents. The injuries were caused by significant blunt forces observed in hit-and-run instances, crush injuries caused by the collision of the car, and uneven road surfaces. In contrast to the findings of the present study Jha, Saurav et al. 8 reported, that in decreasing frequency, the scalp exhibited laceration, contusion, and abrasion at 59.7%,27.3%, and 23.4%, respectively.
In our present study (Table 6), sub-arachnoid haemorrhage 248 (41.06%) and intra-cerebral haemorrhage 195 (32.28%) were the next most frequent types of intra-cranial haemorrhage reported in the present research, respectively. Intra-ventricular haemorrhage 115 (19.04%) and extra-dural haemorrhage 112 (18.54%) were seen in a number of instances that were practically the same. Brain stem haemorrhage was associated with the lowest number of intra-cranial haemorrhages, with 54 cases (8.94%) out of 604 cases. Similar results were noted in a study by Kumar et al., 2 Menon et al., 9 Das et al. 10 Tomar et al., 11 in which they observed that sub-dural haemorrhage was the most common intra-cranial Haemorrhage in RTA followed by subarachnoid haemorrhage, intra-cerebral haemorrhage and least by extra-dural haemorrhage. Arulmathikannan et al., 12 also had a similar observation, except that they observed that intra-ventricular haemorrhage was the third most common intra-cranial haemorrhage in RTAs. The findings of Sharma et al. 13 match our study as it shows that sub-dural haemorrhage and subarachnoid haemorrhages are the leading intra-cranial haemorrhage. However, it refutes our finding by showing a higher percentage of extra-dural haemorrhage than that of intra-cerebral haemorrhage. Modi et al. 14 observed that subdural haemorrhage was the most common intra-cranial haemorrhage as seen in our study, that study contrasts our study by showing extra-dural haemorrhage as the next mostly found intra-cranial haemorrhage whereas in our study the next most common intra-cranial haemorrhage was sub-arachnoid haemorrhage.
Conclusion
Road users should get this education since they are frequently injured in RTAs, making it urgently necessary.
To educate individuals on how to drive safely, we need an integrated curriculum. It is important to teach young children how to cross roadways and utilise sidewalks safely.
Road signs and bicycle safety should be taught to middle school students. High school students will study response times, defensive driving, and the perils of drinking.
To control traffic, the agencies in charge of issuing permits must enact stringent laws and regulations and invest in new technologies. Applicants should be required to undergo a first aid course before receiving a licence.
There is no doubt that implementing pedestrian-friendly routes, designating separate lanes for heavy and light cars, and strictly enforcing traffic laws would help to reduce the number of traffic accidents and fatalities.
Automobile fatalities are an unavoidable scourge of modernisation. They are the cost of our quick travel between sites.
Newspapers and television in particular are more successful in educating the public.
This emphasises how important it is to strictly enforce the laws limiting the limitation of vehicle speeds.
To identify regional safety issues, the authorities and the local population should collaborate.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Permission from the institutional ethical committee was obtained.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Written informed consent was taken from blood relatives of the deceased after explaining the purpose and procedure of the study.