
Abstract
This research aims to identify the elements accountable for retaining talent among home healthcare nurses in Chennai. The researchers adopted a descriptive approach. The sample size of this research study is 217 respondents who are nurses from the micro, small and medium enterprises (MSME) corporate centre at Nandanam, covering its areas within Chennai city. The tool used for this study purpose was the questionnaire, consisting of eight constructs: training, compensation, cohesion, autonomy, workload, non-monetary benefits, nurses’ satisfaction and nurses’ retention. The socio-demographic factors such as age, gender, qualification, annual income, employment type, experience, marital status and designation were considered. Data analysis was done using SPSS 21.0. The reliability measures ensured the consistency of the data set. Percentage analysis, descriptive statistics, Pearson correlation and multiple regression are the statistical tests used. Important discussions were given in the article related to the Indian healthcare sector.
Keywords
Introduction
Home healthcare centres in India are now booming. It not only requires to be understood from an Indian context but also from a global perspective. Primarily, it is good to know what is home healthcare. It is a system of care given by skilled practitioners or nurses to those inflicted with illness in their homes. It is done with the direction of a physician. The services are nursing care, physical, occupational and medical social services. Once, it was seen as a need of the developed nations; now, it has also become a need for a country like India, which is a developing nation in the world. Slowly, home healthcare concept is also found in all metro cities and other cities in India. It happens due to various reasons. Family structure has faced relentless changes over the decades. Modern society is formed by nuclear families against joint families. The fundamental structure of society, that is, family, is at stake, wherein no care for one another has been largely shown, especially to the elderly. Everyone has become busy in the modern world, forgetting to care for their parents, and as a result, they become abandoned and looking for homecare centres.
Technology is much more advanced than before, and people are looking for a modern concept of healthcare to have better healthcare. Through technology, people are adept with the knowledgeability about the best care and its treatment. Home healthcare centres have become an alternative to traditional centres. In such centres, it could be found that investment is done concerning the understanding of micro, small and medium enterprises (MSME), that is, ₹5 crores investment is done on equipment. Cost-effectiveness is another element people are looking for. The healthcare system is affordable and able to save money for healthcare facilities. People need not invest so expensively in illnesses that they could save money. The MSME-run centres also provide a cost-effective method of reaching the patients.
The type of illnesses becomes a major reason why people prefer to have home healthcare. Because of this type of illness, people would like to have better care at home. The nurses reach home and provide treatment. By this, time is saved, and they become free from traffic congestion on the roads, pollution and noise. Personal care becomes a de facto element in home healthcare. Everyone is provided with personal care and develops a feeling of receiving the best care. The MSME-run centres, with areas covered in metro cities like Delhi, Mumbai, Kolkata and Chennai, have already started offering their services with the best care.
It is ironic that as more and more home healthcare is established in India, an equal number of nurses are leaving the country and seeking employability in other countries, especially in Gulf countries, the United Kingdom, Australia and Canada. Perhaps the researchers would like to raise the following research questions:
What makes them leave India and seek jobs elsewhere? What are the retention strategies followed by organisations?
In answer to the above questions, the MSME Act 2006 was passed by the Indian government. The objective of the MSME Act 2006 is to facilitate the promotion and development of small and medium enterprises, as well as to enhance competition among such enterprises. These enterprises are of two types: manufacturing enterprises and service enterprises. The manufacturing enterprises include companies that produce manufactured goods and are listed in the first schedule of the Industries Development and Regulation Act, 1951. It also includes investment in plant and machinery of the manufacturing industries. Service enterprises include the businesses that take part in offering services. Such businesses are categorised based on investment in equipment.
After more than a decade since the MSME Development Act came into existence in 2006, an upgrade in MSME definition was initiated in the Aatmanirbhar Bharat Package on 13 May 2020. As per this initiation, the definition of micro-manufacturing and services units was increased to ₹10 million of investment and ₹50 million of turnover. The limit of small units was increased to ₹100 million of investment and ₹500 million of turnover. In the same way, the limit of medium units was enhanced to ₹200 million of investment and ₹1,000 million of turnover. The Indian government, on 01.06.2020, decided to further revise the MSME definition. For medium enterprises, it will now be ₹500 million of investments and ₹2,500 million of turnovers.
The home healthcare unit has invested ₹5 crores and is running services in Chennai, Coimbatore and Bangalore. Providing nursing care, mobile X-ray, scanning, testing lab, electrocardiogram (ECG), mini post-operative care, ICU, etc., to the home where the patient is being treated at their home itself. Since the home healthcare business is in the budding stage in India, awareness and skill are lacking. That is the major challenge to retaining talent. The researchers would like to quote the following literature being done on home healthcare centres at the global level. They illustrate how the countries are related to this.
The corporate identity of a company displays its trustworthiness and lasting presence in the business world (Murali et al., 2022). This identity is achieved by retaining the best home healthcare professionals in the industry. It is crucial for all organizations, including home healthcare companies.
Home Healthcare: A New Avenue
The home healthcare area in India represented about 3.6% of the country’s general healthcare industry as of 2019. The industry will grow at a compound annual growth rate (CAGR) of 18.91% during the 2020–2025 period. The novel coronavirus flare-up seriously affects the home healthcare market. In the next years of the term, the market will grow abundantly and become a fast-growing segment in the healthcare market. Standard operating procedures (SOP) and social distancing practices are a little complex in hospitals, as well as making them costlier. Telemedicine arrangements have become an advantageous option. This has produced more prominent interest in home healthcare arrangements. This is the right time for policymakers to frame a unique HR policy for the home healthcare market to attract and retain the best talents in the industry. There is no doubt that healthcare employee satisfaction will bring successful patient outcomes.
Problem Statement
Not only has the healthcare sector, but even the general public have also understood the critical contribution of healthcare employees after this COVID-19 scenario. The entire healthcare infrastructure will be in trouble if there are no talent management practices implemented. In the next few years, the healthcare sector will see a twofold growth. The same growth shall not be stopped only because of a shortage in the labour force. While India has a higher young population than any other country, labour shortage problems should not be an issue hereafter. Unvaryingly, workers are the greatest asset of any company. ‘Healthcare companies’ are not exceptional to that case.
Like any other industry, the workforce is not so fixed in this healthcare industry in terms of age. The young workforce is gifted in this industry. This young and charming workforce is attracted to this industry because of the high salaries given by the Middle Eastern countries. For this reason, nursing migration is high in our country. Identified turnover reasons are disrespect, inadequate management, work–family conflicts, job difficulty and job availability (Mittal et al., 2009).
Importance of Nurse Retention
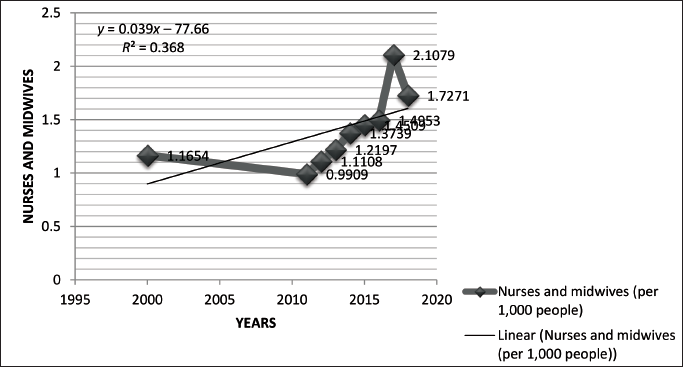
The nursing profession’s ratio of 1.7 per 1000 people, as illustrated in Figure 1, shows a relatively low level, which is not in accordance with the norms established by the World Health Organization. Healthcare employee retention focuses on preventing turnover and keeping the nurses and other healthcare workers in an organization’s employment for a long time. Here are five ways to improve nurse retention and implement easy retention strategies. The nursing workload is directly linked to the satisfactory outcomes of the patient. Estimating adequate staffing is a very tedious process and requires close monitoring and coordination between management and nursing managers based on patient acuity and turnover, availability of support staff and skill mix and many other factors (Needleman et al., 2011). The attrition rate of nurses is between 28 and 35% in India, and it is 10.1% for the healthcare sector on the whole (Lakshman, 2016).
Literature Review
Al Zamel et al. (2020) have done a review study on intention to leave and intention to stay. This study investigated how to review, critique and synthesise the determinants of nurses’ intention to stay or leave the organisation. It was an integrative review study dealing with the past studies, either empirical or concept study. It was done with the search result of 512 articles: PubMed (36 studies), Science Research (9 studies), Science Direct (6 studies), Open Access Library (9 studies), Sage journal (3 studies), Web of Science (6 studies) and Google Scholar (443 studies). Among them, 209 studies were reviewed, 45 studies were removed because of the duplicates, and 127 studies were rejected for irrelevant content. In the end, exactly 37 articles related to factors influencing nurses’ intention to leave and to stay in the organisation were published. Out of these, five studies were mixed-method, two studies were qualitative and 30 studies were quantitative. It was concluded that job satisfaction was considered to be a serious factor affecting the intention to leave, with varied categories such as pay, work environment, workload, profession, peer support, family support and problem-focused coping.
Dhanpat et al. (2019) aimed to find out the relationship between employee retention and job security. It was a cross-sectional design done from three public hospitals in Johannesburg, South Africa. About 320 questionnaires were distributed, and only 203 were complete and considered for the study’s purpose. Nurses faced a low level of job security. There was a lack of career opportunities and career development. To feel secure, retention strategies were to be prioritised. Training and development were the best predictors of job security. A secure and conducive work environment led the nurses to develop a sense of belonging and increased job security.
Van Waeyenberg et al. (2015) conducted a research study on home nurses’ turnover intentions: the impact of informal supervisory feedback and self-efficiency. It was done in Flanders, Belgium, to examine the relationship between home nurses’ turnover intentions and frequency of supervisory feedback and self-efficiency. The authors have administered a cross-sectional survey design. The questionnaire was distributed to 476 home nurses, and only about 312 home nurses returned it. The response rate was above the mean response rate found in organisational sciences (Anseel et al., 2010). The nurses were selected from a large home healthcare organisation in Flanders. This study revealed that informal supervisory feedback and self-efficacy have influenced home nurses’ turnover intentions. It also revealed that high-quality feedback decreased home nurses’ turnover intentions by enabling home nurses’ self-efficacy. It was also found that there was a direct negative relationship between favourable feedback and turnover intentions.
Tourangeau et al. (2013) identified the factors affecting Canadian home healthcare nurses’ intention to remain employed. It was done in Ontario, Canada, with approximately 27 for-profit and not-for-profit home care organisations giving nursing services. Those organisations employed registered nurses (RNs) and registered practical nurses (RPNs). Convenience sampling was employed. Six categories of influencing factors were considered: job characteristics, work structures, relationships, communication, work environment and nurse responses to work and employment conditions. It was found that autonomy, flexible scheduling, reasonable and varied workload, supportive work relationships and receiving adequate pay and benefits influenced the nurse’s intention to remain in their profession.
Cowden et al. (2011) aimed to find out the relationship between managers’ leadership practices and staff nurses’ intent to stay through a systematic review. The researchers have used databases like Medline, Education Resources Information Center (ERIC) and Scopus. The variables considered for this study are organisational commitment, job satisfaction, leadership practices, work environment, individual nurse characteristics, career development and opportunities elsewhere. It resulted in a positive relationship between leadership, work environments and staff nurses’ intentions to remain in their current positions.
Wang et al. (2011) carried out a study in mainland Chinese nurses to find out the degree of satisfaction, intention to stay and commitment towards the profession. The sampling size was 560 nurses. They were working in a large hospital in Shanghai. A higher level of occupational commitment, with great enthusiasm for their work, led them to remain in their job. Demographic variables like age and job position were significantly related to the level of intent to stay.
Stordeur and D’Hoore (2007) did a study with the RNs amounting to 2,065 nurses from the European context through a self-structured questionnaire. The significant difference was that nurses’ perception towards three components: work environment, exposure to physical health-related factors, work schedules and job demands and stressors. In attractive hospitals, lower health hazard exposure has been reported. Job demands and stressors were also lower compared to conventional hospitals. Balancing factors like job latitude (the amount of discretion that workers have when and how they perform their work) and rewards are found to be favourable. This is because the increase in job control helps nurses in coping and maintaining high job satisfaction.
Armstrong-Stassen and Cameron (2005) have done a study on concerns and retention of Canadian Community Health Nurses. This study was done in Ontario, Canada. Its purpose was to find out the work-related concerns of nurses involved in community healthcare. In Ontario province, most of them were employed in public health, homecare and community care access centres. The sample was 1,044 participants, of which public health had (n = 386) respondents, home care had 410 respondents and community care access centres had 248 respondents. This study concluded that home care nurses were less satisfied with their pay and benefits. The increases in workload and job insecurity were created by the managed competition system.
Methodology
This part consists of research objectives, hypotheses, pilot study, sampling method and data analysis. The data have been analysed with SPSS 21.0. The results are arrived at the end of the study.
Research Objectives
To study the socio-demographic factors of the home healthcare nurses of Chennai city
To find the predictors of nurses retention in the home healthcare sector
To provide valuable insights that contribute to the home healthcare sector.
Research Hypotheses
H1: Continual reskilling and upskilling positively impact home healthcare nurses retention.
H2: A transparent and fair compensation/promotion system is positively associated with home healthcare nurses retention.
H3: Cohesion with physicians significantly predicts home healthcare nurse retention.
H4: Autonomy and the ability to intervene in patient improvement positively influence home healthcare nurses retention.
H5: Equitable distribution of workload among home healthcare nurses is linked to higher retention rates.
H6: Non-monetary/gratitude for exceptional services contributes to home healthcare nurses retention.
H7: Increased home healthcare nurse satisfaction is impacting higher retention rates of nurses.
Sampling Method
A descriptive design has been adopted in this study. The researchers have adopted a simple random sampling method, considering Nandanam in Chennai city as the corporate centre. This corporate centre includes area coverages for the study purpose: Anna Nagar, Ashok Nagar, Vadapalani, Alwarpettai, Parry’s Corner, Adyar, Thiruvanmiyur, Velacherry, East Coast Road (ECR), Tambaram, Puzhal, Porur, Adambakkam, Valasaravakkam and Purasaivakkam. Both the registered and unregistered nurses were considered for this research study. The questionnaire is constructed following the scale validated by Tao et al. (2010). The tool consisted of eight constructs: training, compensation, cohesion, autonomy, workload, non-monetary benefits, nurses’ satisfaction and nurses’ retention. The researchers reached out to the nurses’ respective areas, distributed the questionnaire and got them filled in. Collected data had been codified and analysed with SPSS, and results were drawn from it. Each construct statement was tested with the alpha Cronbach test to check the internal consistency of the questionnaire. The results are illustrated in Table 1.
Reliability Measures.
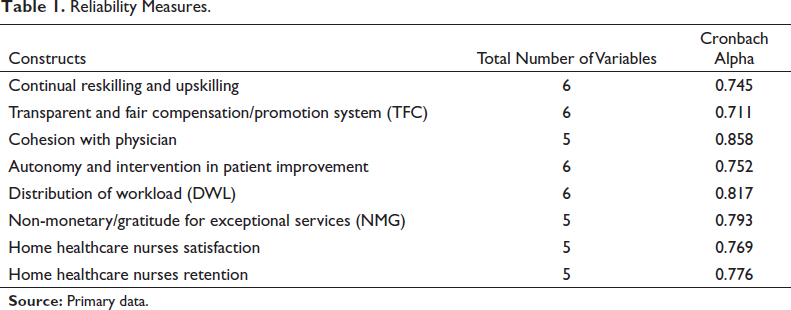
Table 1 shows the home healthcare talent retention constructs and the corresponding Cronbach alpha scores computed. Cronbach alpha is a measure of internal consistency. Cohesion with physician (0.858) and distribution of workload (0.817) are the constructs having attained the highest Cronbach alpha scores. A transparent and fair compensation/promotion system (0.711) and non-monetary/gratitude for exceptional services (0.793) show a satisfactory score of 0.7 and above. Thus, it shows that there is internal consistency between each construct and responses involved in it. It also shows that the statements are logically built. Perhaps it is worth undertaking such a study.
Data Analysis and Results
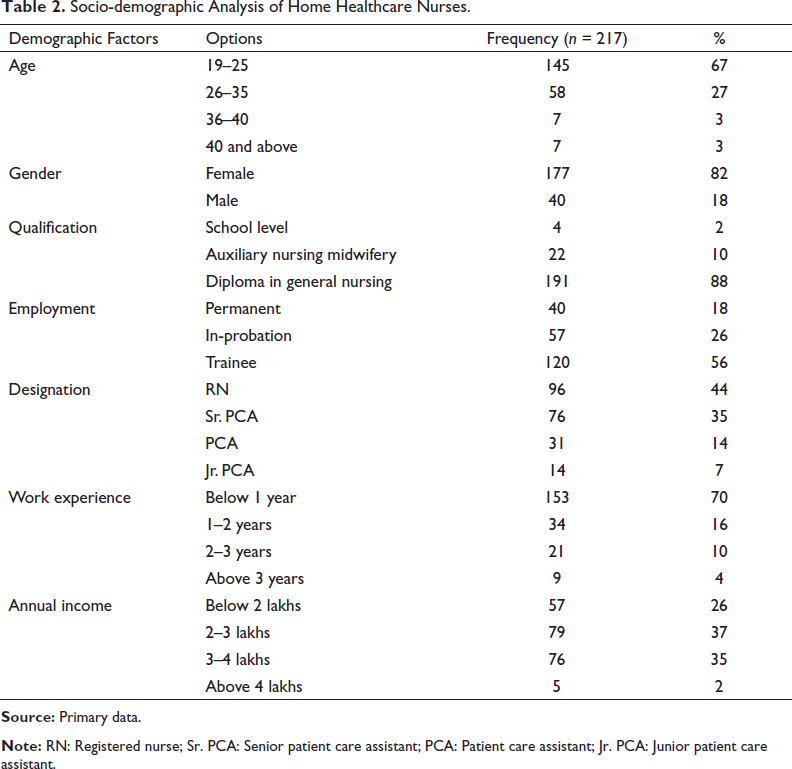
In the context of Table 2, 82% of the home healthcare nurses in the sample are females 67% are between the ages of 19 and 25, and 88% hold a diploma in general nursing. About 18% of nurses are working permanently, while the remaining nurses are either ‘in-probation’ or ‘trainees’. Registered nurse (44%) is the most popular title, followed by senior staff nurse (35%) and junior staff nurse (7%). The majority of nurses (71%) have less than 1 year of work experience, followed by those with 1–2 years (16%), 3–4 years (10%) and more than 3 years (4%). Below 2 lakhs is the most prevalent yearly income level (26%), followed by 2–3 lakhs (36%), 3–4 lakhs (35%) and beyond 4 lakhs (2%).
Socio-demographic Analysis of Home Healthcare Nurses.
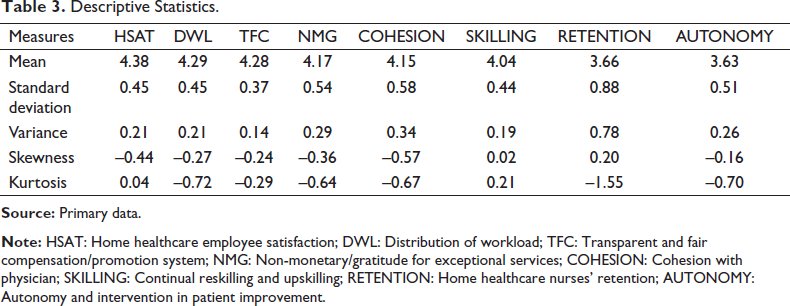
As per the descriptive statistics illustrated in the Table 3, the home healthcare nurses are satisfied in their jobs as the mean score is 4.38, which is the highest in the study. The standard deviation (SD) for the distribution of workload is 0.45, which shows there is more perception variation among the nurses in the distribution of work. The skewness score for the nurses is computed as –0.44, which shows that most of the nurses are less satisfied. The kurtosis value generated for all the constructs is nearer to zero, which shows that the data is normally distributed. The descriptive statistics show that, in principle, the nurses are satisfied; however, the areas of workload allocation, training and relationship with doctors need to be improvised.
Descriptive Statistics.
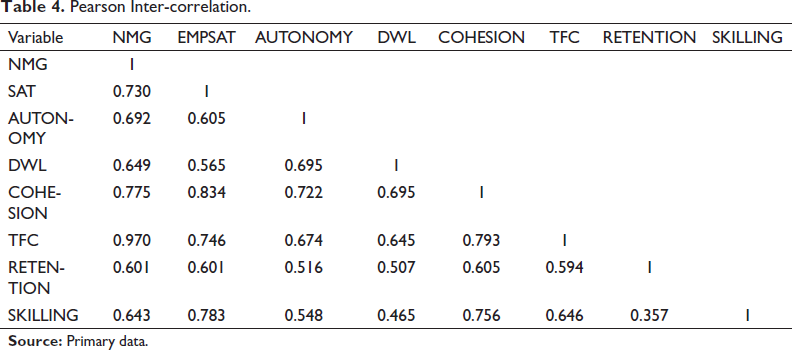
NMG (non-monetary/gratitude for exceptional services) is strongly correlated with EMPSAT (nurses’ satisfaction) (r = 0.73), AUTONOMY (autonomy and intervention in patient improvement) (r = 0.69), SKILLING (continual reskilling and upskilling) (r = 0.64) and RETENTION (home healthcare nurses’ retention) (r = 0.60). This means that nurses who feel appreciated for their work tend to be more satisfied with their jobs, have more autonomy, are more likely to be upskilled, and are less likely to leave their jobs.
Nurses’ satisfaction is also strongly correlated with TFC (transparent and fair compensation/promotion system) (r = 0.74) and COHESION (cohesion with physicians) (r = 0.83), which shows that nurses who are satisfied with their pay and promotion opportunities, and who have good relationships with their physicians, are also more expected to be satisfied with their healthcare job. DWL (distribution of workload) is negatively correlated with nurses’ satisfaction (r = –0.56) and RETENTION (r = –0.51), which shows that nurses who feel that their workload is too heavy are less likely to be satisfied with their jobs and are more likely to leave their jobs. Pearson inter-correlation in Table 4 portrays NMG (non-monetary gratitude for exceptional services) is strongly correlated with EMPSAT (nurses’ satisfaction) (r = 0.73), AUTONOMY (autonomy and intervention in patient improvement) (r = 0.69), SKILLING (continual reskilling and upskilling) (r = 0.64) and RETENTION (home healthcare nurses’ retention) (r = 0.60). It is concluded that the nurses who feel appreciated for their work tend to be more satisfied with their jobs, and those who have more autonomy are more likely to be upskilled and are less likely to leave their jobs.
Pearson Inter-correlation.
Regression Equation
Table 5 provides insights into the factors influencing home healthcare nurse retention, as determined by the regression analysis. Home healthcare nurses retention = (−0.543) + 1.368 × home healthcare employee satisfaction + 0.447 × non-monetary/gratitude for exceptional services + 0.126 × autonomy and intervention in patient improvement + 0.072 × distribution of workload − 0.033 × cohesion with physician − 0.319 × transparent and fair compensation/promotion system − 0.534 × continual reskilling and upskilling.
Factors Predicting the Retention of Home Healthcare Nurses.
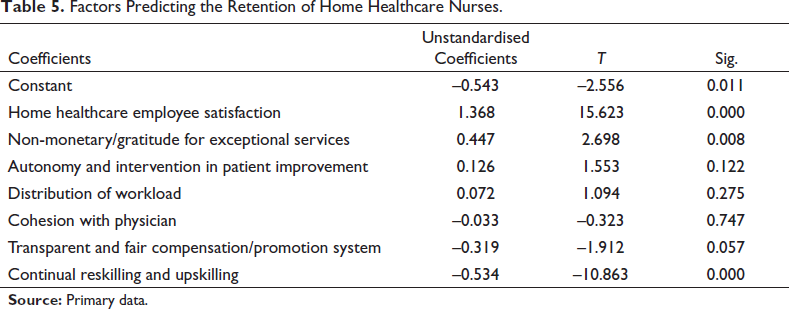
Home healthcare employee satisfaction (1.368) has a positive effect on nurses’ retention, followed by the construct continual reskilling and upskilling (–0.534), where the p value is <.001. A unit increase in home healthcare employee satisfaction is associated with a 1.368 unit increase in employee retention, holding all other independent variables as constant. Non-monetary/gratitude for exceptional services (0.447) shows a positive effect on the nurse’s retention as the obtained p value is <.001. Autonomy and intervention in patient improvement, distribution of workload (0.072) and cohesion with physicians (–0.033) have no significant effect on employee satisfaction. H1, H6 and H7 alone are accepted, and others are rejected.
Results and Discussion
From the demographic profile of the respondents, it is shown that 82.0% of the respondents are females, while the remaining 18.0% are males. It is quite obvious that most of the persons employed in the nursing profession are found to be females from India. From this study, the H1, H6 and H7 have been accepted.
The descriptive statistics in Table 3 have shown that, in principle, the nurses were satisfied; however, the areas of workload allocation, training and relationship with doctors need to be improved. Nurses’ satisfaction is also strongly correlated with TFC (transparent and fair compensation/promotion system) (r = 0.74) and COHESION (cohesion with physicians) (r = 0.83), which shows that nurses who are satisfied with their pay and promotion opportunities, and who have good relationships with their physicians, are also more expected to be satisfied with their healthcare job. DWL (distribution of workload) is negatively correlated with nurses’ satisfaction (r = –0.56) and RETENTION (r = –0.51), which shows that nurses who feel that their workload is too heavy are less likely to be satisfied with their jobs and are more likely to leave their jobs.
India is not only rich in its legacy and diversity, but it is also famous for its skilled workforce. Indian workers are perceived to be talented, hardworking and result-oriented by nations around the world. This has been proven many times. However, the healthcare workforce we have in India is not sufficient, and we still have miles to go. The shortage of nurses has forced hospitals to frame new strategies and interventions to improve healthcare quality. Healthcare management should consider investing in talent management practices for the nurses to make them more engaging (Karamaliani et al., 2016). The pandemic situation also highlighted the same. We have resources, manpower and infrastructure in the healthcare setup. The only thing is, we have to scale up the operations by fulfilling the needs. Implementation of better compensation packages is suggested. A high level of a skilled and diverse workforce is needed in a sector like healthcare. The quality of the healthcare human source is affecting the delivery of service and patient satisfaction (Sarma & Barua, 2018). Performance-based financing to the healthcare workers will improve job satisfaction and reduce attrition (Shen et al., 2017). The system of personnel management, talent-based incentives and focused training will strengthen the nursing workforce (Wang et al., 2021).
‘
While we say great progress in improving the healthcare system in India, we have a shortage of healthcare workers. Our healthcare workforce is not as recommended by the WHO, as the number of active doctors and nurses is very low. Not only the domestic patient traffic, but we are also globally viewed as a ‘Medical Tourism’ hub, as international medical tourists prefer our country for the quality, affordability and hassle-free visas. In the forthcoming years, the Government of India and healthcare administrators should focus on attracting and retaining a talented workforce. Rural India is greatly affected by this shortage and derisory healthcare services (Motkuri et al., 2017). World countries are very interested in welcoming Indian nurses to their countries by giving attractive salaries and perks to them, as the nurses from India are skilled, English-speaking and hardworking. We lose our potential nurses because of the low salaries paid in our country (Gill, 2011). Our country has very less nurses than the WHO recommended standards. (WHO recommends three nurses per 1,000). The doctor–patient ratio is much lower in India than the standard of 1:1,000. India needs an immediate upscaling process to increase the healthcare workforce in the country. The medical graduates produced every year and the nurses completing the courses in India are much lower in our country than in other countries. The COVID-19 pandemic outbreak has highlighted the importance of healthcare workers. Patient safety, timely treatment and operational planning are the factors that depend upon the talent management of the healthcare workers (Taha et al., 2015). Healthcare organisations should develop a rigid policy to attract, develop and retain talented healthcare workers (Bibi, 2019). Healthcare managers should develop plans to boost job satisfaction and workplace incentives, encouraging recent graduates to consider long-term care positions (Moyle et al., 2003).
Conclusion
This study concluded that continual reskilling and upskilling have positively impacted home healthcare nurses retention. A transparent and fair compensation/promotion system has also been positively associated with home healthcare nurses retention. Cohesion with physicians has significantly contributed to being a predictor for home healthcare nurses retention. Since the duration of the nurses’ stay in the nursing job was very minimal, all the Indian staff are likely to earn quick money in less time. Like in other countries, they are paid salary on an hourly basis rather than a monthly basis in Chennai. The problems and challenges could be overcome by concentrating and improving on the above-mentioned variables. Thereby, the home healthcare centres could overcome the retention challenges and minimise the staff going to other countries. Research studies could be undertaken in the above areas, which would be of greater concern for an Indian context.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.