
Abstract
This paper contributes to anchor institution, migrant and refugee integration, skills utilisation and inclusive growth debates. Via a pioneering innovative approach to inclusive urban development linking together physical infrastructure development and neighbourhood management approaches to urban regeneration, it explores the potential for micro assets within communities to be linked to macro assets of large spatially immobile anchor institutions. Through a case study, it draws on experience, and identifies transferable learning points, from a skills-matching element of a large European Union funded project in a superdiverse inner-city deprived neighbourhood in Birmingham, UK. In contrast to the typical emphasis of area-based employment initiatives on people with low skills, the skills-matching initiative focuses specifically on connecting skilled overseas migrants and refugees to skilled and highly skilled jobs in a large local hospital. It underlines the central role of local partnership working and highlights the role of skills utilisation, not merely skills development, in inclusive growth. The evidence suggests that three components underlie success in unlocking and catalysing links between micro assets and a macro asset to realise anchor institution potential: (1) institutional entrepreneurship, which provides the strategic buy-in from the anchor institution; (2) innovative entrepreneurship, which provides the delegated responsibility for implementation; and (3) vision and place leadership, which provides the strategy and resources to build the bridge between the macro asset and the local community to help realise inclusive growth.
Keywords
Introduction
Inclusive growth has emerged as a concept and agenda for reconciling ambitions to reduce inequalities and raise productivity. As such, it has been the subject of extensive critique (Lee, 2018). The concept has risen up the international agenda and has been adopted sub-nationally at the city level. While there are different interpretations of inclusive growth (Green et al., 2017), for the Organisation for Economic Co-operation and Development (OECD, 2017) the key issue is economic growth that is distributed fairly across society and creates opportunities for all. In an extensive review of the concept, Lupton et al. (2019) conclude that inclusive growth is economic growth that creates broad-based opportunities and benefits for all. They argue that inclusive growth policy and practice includes working towards economic structures and activities that are more inclusive by design as well as making sure local people are connected to economic opportunities.
These interpretations of inclusive growth describe outcomes contrary to prevailing trends in UK cities, where there is little relationship between economic growth and poverty reduction (Lee and Sissons, 2016). Consequently, people and places have been ‘left behind’ (Rodríguez-Pose, 2017). Pinoncely (2016: 3) asserts that ‘making a real impact on poverty and inequality will require a new focus on promoting fairness, opportunity and social mobility through more concerted and coordinated efforts to improve the places and communities in which people live’.
While debates on inclusive growth often focus on regional and city-regional scales, concerns about socio-economic inequalities are evident across geographical scales. Often, inequalities are most evident as neighbourhood concentrations of extreme and persistent disadvantage within cities contrasting with much more prosperous neighbourhoods (Social Exclusion Unit, 1998). This paper adopts a neighbourhood lens in the inclusive growth debate and brings urban regeneration policy to the fore.
Viewed in a broader historical context, urban regeneration policy in the UK in the early 1980s focused on creating conditions for economic success through large-scale physical regeneration activity. In the 1990s there was a move towards partnership approaches to regeneration and more focus on economic and social factors. A National Strategy for Neighbourhood Renewal in 2001 introduced new initiatives to regenerate deprived neighbourhoods physically, economically, socially and environmentally (Syrett and North, 2008). From 2010 there has been a shift back towards private sector-led physical regeneration and inward investment-driven economic development through City and Growth Deals. While a variety of approaches have been used with varying degrees of success, spatially concentrated urban poverty persists.
Connecting people to jobs is a central feature of inclusive growth policies, area regeneration and local economic development policies and is the focus of attention in this paper. Orthodox approaches have tended to view disadvantaged people and places as ‘deficient’ subjects of policy initiatives. A more fruitful approach is to consider them as areas of transformation and potential. For place-based policy this puts a premium on understanding how stronger place-based initiatives can recognise and nurture existing assets to support and promote employment, educational achievement, better health and improved social mobility (Pinoncely, 2016). A key issue is how to generate systemic change that will continue to create positive outcomes for the longer term. Theoretically, there is potential for system change to occur when large local organisations (i.e. ‘macro assets’) seek to enact their role as anchor institutions by prioritising and resourcing engagement with ‘micro assets’ in the local area as part of their business activities.
Adopting a neighbourhood perspective, through a single case study, 1 this paper provides insights into the potential for micro assets within communities to be linked to place-based macro assets to deliver inclusive growth. It draws on the experience of a three-year European Union (EU) Urban Innovative Action project aimed at pioneering innovative approaches to inclusive urban development in a superdiverse inner-city deprived neighbourhood in Birmingham, UK. 2 The paper focuses on one specific strand of broader project activity: connecting residents (notably migrants and refugees) to jobs in large spatially immobile anchor institutions. This is a topic of international interest, as the literature on large educational and medical institutions (‘Eds and Meds’) in the USA (Dubb and Howard, 2012; Fulbright-Anderson et al., 2001; Harkavy and Zuckerman, 1999) and the concentration of migrants and refugees in many European cities exemplifies (OECD, 2018). However, there are notable differences in foci of anchor institution literature, with a greater neighbourhood focus in the USA and a more regional focus in much of Europe (Ehlenz, 2018), likely reflecting (in part) differences in the state’s role in communities and anchor institution governance structures.
The analysis presented here concentrates specifically on how a macro asset (a particular hospital) realises an anchor institution role by connecting residents to opportunities. As such, it relates to growing interest in anchor operations at the neighbourhood level and anchor–community partnerships (Belongie and Silverman, 2018). In contrast to many urban regeneration programmes that concentrate primarily on supply-side skills development programmes to address challenges in accessing employment for those with no/low qualifications, the article is concerned with a topic that has been more neglected in the literature: better utilisation of higher-level skills. Specifically, it focuses on the opportunities, challenges and lessons learned from implementing an initiative to recruit highly qualified migrants and refugees to hospital jobs in which they can utilise their skills. The novelty of the article’s contribution lies in investigating the role of improved skills utilisation in inclusive growth, the role of partnerships in providing skills-matching services and the different geographical scales at which inclusive growth policy needs to operate, while adding to debates on neighbourhood regeneration, urban poverty, local community development and migrant and refugee integration. As such, it provides crucial lessons for asset-based community development (ABCD) / anchor institution development within European cities that have received many new migrants over the past decade. It also focuses on hospitals, which are often overlooked within anchor institution studies.
The remainder of the article is structured as follows. The next section discusses the background to ABCD, the role of anchor institutions – with a particular focus on the role of hospitals as anchors – and issues pertaining to migrant and refugee integration in cities. This is followed by discussion of the data and research methods used. The next section sets out the context of the case study, including the background to, and the philosophy and scope of, the urban regeneration initiative in question. It also outlines the characteristics of the case study neighbourhood. The main substantive section presents the case study initiative to place skilled overseas migrants and refugees in skilled hospital jobs. This includes the rationale for the particular focus adopted, the aims and achievements of the programme and associated learning points. The final section comprises a broader discussion and concludes.
Asset-based development, the role of anchor institutions and migrant/refugee integration in cities
Traditional policy approaches often see people and places of concentrated disadvantage as ‘problematic’/‘deficient’ subjects of policy initiatives. By contrast, ABCD builds on existing (sometimes hidden) resources and aims to mobilise them to strengthen the neighbourhood/local economy (Kretzmann and McKnight, 2003; Mathie and Cunningham, 2003). It facilitates sustainable community-driven development by using the capacities of local people and connecting them to the resources of local places, including those of public, private and non-profit institutions. In an ABCD approach linking micro assets to macro assets, well-being is not solely an individual responsibility, but a shared responsibility with the (local) state and civic society. ABCD develops and embeds interventions relationally within communities, by strengthening the assets themselves and, importantly, the links between them. In the context of the case study presented here, the ABCD approach is closely aligned to community wealth building. At the heart of this approach is the principle that the assets of a place can be leveraged for local economic benefit (Centre for Local Economic Strategies, 2019). The actions of anchor institutions are of key importance here.
Anchor institutions tend to operate on a not-for-profit basis and have two key features. Firstly, they are spatially immobile with strong ties to the geographic area in which they are based. Although displaying potential for playing a highly localised role, often their functions are multi-faceted and multi-scalar in that they are also networked strategically in regional, national and international research, innovation and human capital development collaborations and partnerships (Addie, 2019). Their second key feature is their large size in employment and purchasing power. As such, place-bound anchor institutions potentially provide considerable resources and institutional capacity for community economic development, but it is insightful to consider them as macro assets as opposed to fully fledged anchor institutions until their potential is realised. Their activities can range from the redevelopment of neighbourhoods and provision of investment resources and contributions to building workforce skills. Often workforce development programmes associated with community economic development concentrate on low-skilled workers (Nelson and Wolf-Powers, 2010; Schildt and Rubin, 2015) and involve community–labour coalitions (Doussard and Fulton, 2020), whereas labour unions are notably absent in the case study presented here. A key contribution of this article is to focus on a different, often neglected, group of more highly skilled individuals, specifically migrants and refugees.
A significant increase in arrivals of migrants and refugees in 2015–2016 brought migration and asylum policies to the centre of political debate in the EU and across all levels of government and society, especially in cities where migrants overwhelmingly congregate (Bamberg et al., 2020). Municipalities and community groups in cities play a key role in the provision of training (especially for hard-to-reach groups) and facilitating access to services to meet immediate needs (Galera et al., 2018). When asylum seekers and refugees access work they are often engaged in jobs below their skills levels. They could offer new opportunities for deprived areas if initiatives were introduced to help them access work commensurate with their skills and qualifications (Phillimore and Goodson, 2006). Yet, with few exceptions (e.g. Butt et al., 2019 on refugee healthcare professionals in London), professional skills initiatives focusing on labour market integration for refugees/migrants face barriers such as conversion of professional qualifications and a lack of familiarity with recruitment processes that are relatively under-developed.
The focus of this article is on one particular type of macro asset/anchor institution: hospitals. Scholarship on this topic has a longer pedigree in the USA than in the UK and Europe, but there is a growing body of evidence on their potential in generating social value within a community wealth building framework (Centre for Local Economic Strategies and The Democracy Collaborative, 2019). In contrast to the UK, there is no universal healthcare in the USA. Rather, most healthcare facilities are owned and operated by private sector businesses. Following the 2010 Affordable Care Act requiring all non-profit hospitals in the USA to conduct a Community Health Assessment at least every three years, there is increasing interest in looking beyond the traditional focus of hospitals on providing direct care for patients towards looking at their role as urban institutions, including on improving health and examining the social determinants of health in their surrounding local communities, and involving groups and organisations not typically represented in the healthcare delivery system in understanding the needs of geographic areas (Franz et al., 2019; Kaplan and Gourevitch, 2020; Wahowiak, 2017). Yet, analysis suggests that their contribution as anchor institutions in the USA varies by size and type of hospital (Cramer et al., 2017; Sherman and Doussard, 2019).
In the UK hospitals are exploring their potential as anchor institutions to use their financial, employment and other assets to support local economies and tackle social determinants of health (Vize, 2019). The National Health Service (NHS) is the largest employer in the UK, employing more than 1.6 million people across the skills spectrum from consultants to cleaners. There is synergy between the place-based lens of the NHS and broader policy that emphasises localism in shaping the socio-economic environment. The NHS Long Term Plan (NHS, 2019) has an objective exploring the potential of the NHS as an anchor institution. However, a review of NHS initiatives benefiting their surrounding communities notes that while there are promising activities where anchor practices are happening, they tend to be discrete, narrow in scope and not intentionally applied or integrated into central and local systems or organisational strategies (Reed et al., 2019). This highlights a gap in building more systemic approaches.
The emphasis here is on workforce strategies. Anchor institution workforce strategies typically fall into one of three categories (Reed et al., 2019). The first is widening workforce participation, including targeting positions for local people, understanding local demographics and opportunities and creating pre-employment programmes, work placements and volunteering opportunities. The second is building the future workforce, notably through apprenticeships. The third subsumes ‘good employer’ initiatives, including supporting the well-being of staff, fair pay and employment conditions and professional development and career progression. The case study presented in this article falls broadly into the widening participation category, with an extension to include paid employment positions and a novel focus on skills utilisation.
Data and methods
This article adopts a case study approach (Yin, 2014). The object of the case study is a specific initiative within a neighbourhood-based project: USE-IT! The real-world context of this initiative is outlined in the next section.
The case draws on a mix of data sources and methods. Firstly, it uses secondary data sources, specifically the Census of Population (CoP) and the Annual Survey of Hours and Earnings (ASHE), to profile the Birmingham neighbourhood that is the focus of attention for the case study. The CoP is the most comprehensive source of information available on the demographic and socio-economic structure of the neighbourhood at the micro scale, albeit its decennial frequency means that it does not capture short-term changes, which is a clear disadvantage in the context of new arrivals and other demographic changes. The ASHE contains information from employers on levels and distribution of earnings. Secondly, it draws in part on in-depth findings from an initial skills mapping exercise undertaken in the neighbourhood using a survey co-designed by the University of Birmingham and ‘community researchers’ (i.e. members of the community trained to conduct research on the local area as part of the project), which provided very detailed information on the qualifications, previous experience and current circumstances of 118 households. This detailed information was invaluable, but the representativeness of the relatively small achieved sample is unclear. Thirdly, it utilises an analysis of administrative records relating to implementation of activities to place skilled migrant workers and refugees in hospital jobs. These records are from a local organisation set up by the NHS to help residents into local NHS employment. They include information on citizenship, right to work in the UK, qualifications (and where they were gained), previous work experience, English language competence, etc., for all individuals it engaged with, plus details of specific training, work placements and employment outcomes resulting from the organisation’s support. Fourthly, it draws on testimony collected on a monthly basis throughout the initiative from interviews with individuals engaged in the strategic direction of the initiative and its management (most notably the Project Co-ordinator and Manager) and community organisations delivering related training and support, and from participants (mainly via focus groups covering over 40 participants conducted and coded by graduate placement students) and individual interviews focusing on life stories. Finally, it utilises evaluation insights from the broader urban regeneration project (see below for further details). The case study is situated in a broader theoretical and policy context drawing from the academic and policy literature.
Tackling urban poverty in a Birmingham neighbourhood
The remainder of this article focuses on one case study initiative within a broader project to tackle urban poverty: USE-IT! (Unlocking Social & Economic Innovation Together). To set the context, this section provides some key details about USE-IT! and its theory of change before describing the location of the USE-IT! area and its demographic and socio-economic profile.
The USE-IT! project
USE-IT! was a £3 million three-year project (running from 2017 to 2019 3 ) aimed at tackling urban poverty through innovative solutions. It involved innovative approaches to inclusive urban development in a superdiverse area of persistent poverty and deprivation in inner-city Birmingham (outlined in more detail below).
Before USE-IT!, two contrasting and separate approaches to urban regeneration had been trialled in Birmingham with partial success. The first involved physical interventions through large infrastructure investments to attract further investments into specific neighbourhoods, with the expectation that through these investments the neighbourhoods would be regenerated with the community benefitting through trickle down processes. The second neighbourhood management approach involved trying to empower people and organisations in the neighbourhood, mainly focusing on social and cultural issues. The USE-IT! theory of change brings together these two approaches by recognising and building the ‘micro assets’ of the local community (i.e. the [latent] skills of people, neighbourhood groups, etc.) in the area and connecting them with the resources of ‘macro assets’ (notably infrastructure projects and anchor institutions) in order to maximise economic and social benefits for local communities (Scheffler, 2017). This necessitates a partnership approach. The USE-IT! partnership comprised 15 organisations including a local authority, a hospital trust, two universities, national and local organisations, economic development specialists and neighbourhood organisations. Many of these organisations had not worked together before the project began; some had no previous experience of area-based regeneration.
The USE-IT! project comprised several elements, including training community researchers, skills mapping (i.e. matching skills in the community with jobs), social enterprise and social finance. The specific focus here is on the skills-matching element of USE-IT!: connecting people with unrecognised high-level skills and qualifications to a local hospital with a chronic skills shortage. This specific element is outlined in more detail next.
The local area and neighbourhood
Birmingham is England’s second city, occupying a central location in the West Midlands region. Historically in the heartland of UK manufacturing, it is now a major services centre; the health and education sectors are major employers. The USE-IT! area covered an inner urban transect of around 50,000 residents at the time of the 2011 Census, situated immediately to the west of (but not including) Birmingham city centre. At the start of the USE-IT! project it was an area of large-scale urban regeneration, with substantial house-building planned and with a new hospital under construction to replace the existing City Hospital located in the area. Such new developments have the potential to provide better work, education and well-being opportunities for residents in the local area. However, many jobs in the existing City Hospital are filled by workers from elsewhere in Birmingham and beyond, rather than by residents from the immediate vicinity.
The 2011 Census 4 statistics show that the population of the USE-IT! area is younger than across the city as a whole and nationally, with over 40% aged under 25 years (see Table 1). The share of the population aged 25–64 years is similar to the city average at 51%. The USE-IT! area population is more ethnically diverse than the city and nationally. In 2011, nearly 60% defined themselves as Asian/Asian British or Black/African/Caribbean/Black British. These broad ethnic groupings disguise a diverse range of nationalities and geographical origins. Between 2001 and 2011, the shares of the population from all Black and minority ethnic groups increased at the expense of the White group to a greater extent than in several other superdiverse neighbourhoods in Birmingham. Ongoing change in the population since 2011 is not captured by official sources.
Socio-demographic characteristics of the USE-IT! area, 2011.
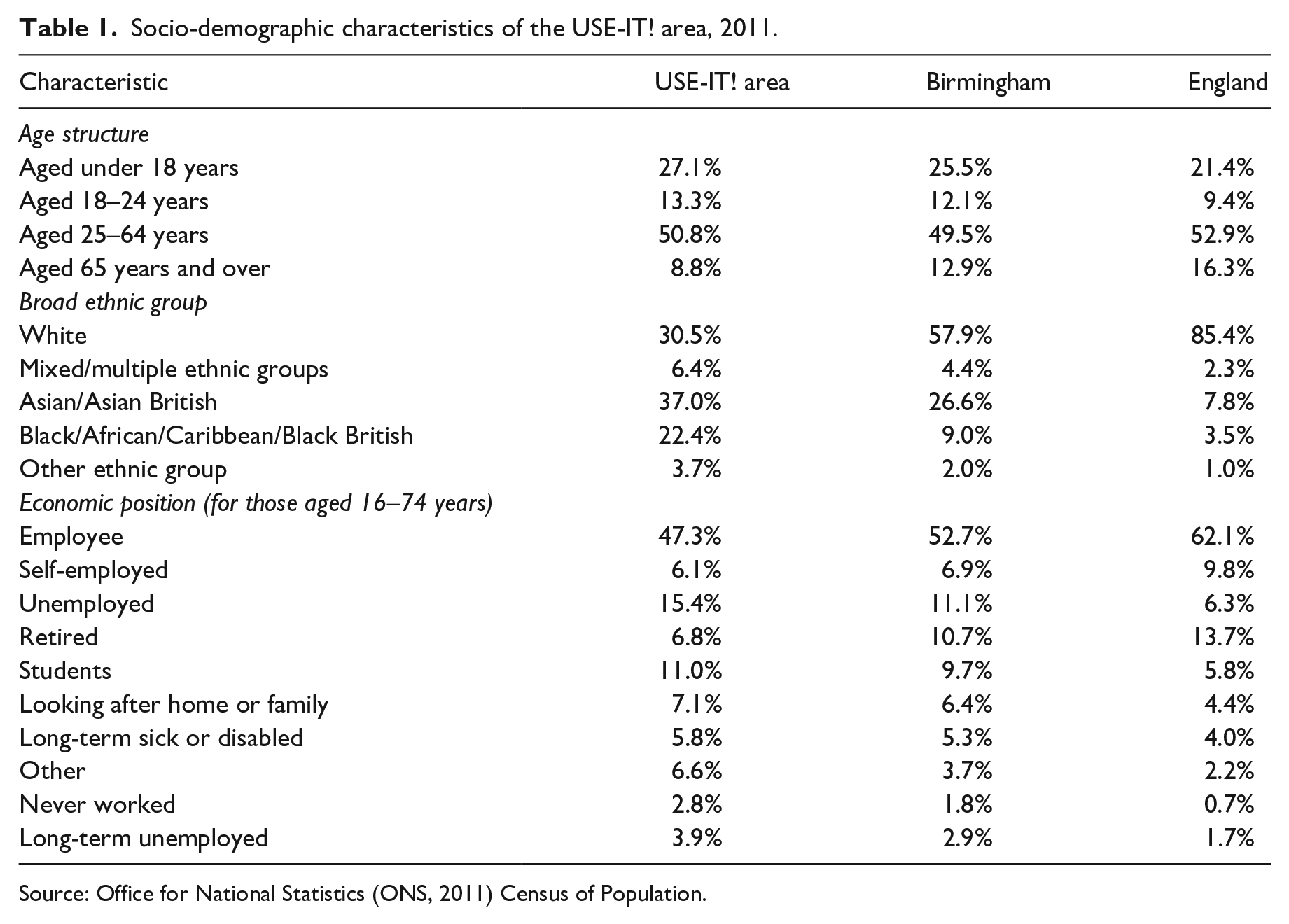
Source: Office for National Statistics (ONS, 2011) Census of Population.
According to the 2015 Index of Multiple Deprivation (the most up-to-date available at the conception of the USE-IT! initiative), 56% of the USE-IT! area fell within the 10% most deprived areas in England, compared with 40% across Birmingham as a whole (Ministry of Housing Communities Local Government [MHCLG], 2015). These statistics identify the USE-IT! area as a transect of the city suffering significantly high poverty with a superdiverse population.
In 2011, nearly 63% of USE-IT! area residents aged 16–74 years were economically active (slightly less than in Birmingham and England), with just over half in employment (a smaller proportion than in Birmingham or nationally) and just over 15% unemployed (a higher percentage than in Birmingham or nationally). The unemployment rate was highest for those with no/low qualifications, but was still around 9% for those with degree-level qualifications, compared with less than 4% for those with higher-level qualifications across England as a whole. Non-comparable time series data on benefit claimants shows that unemployment fell between 2011 and 2019, but remained above the city and national average in the USE-IT! area. Amongst economically inactive residents of the USE-IT! area aged 16–74, retirees comprised a smaller share than in Birmingham or England, but more were students, looking after the home or family, long-term sick or disabled or had never worked.
Figure 1 shows the occupational structure of usual residents in employment in the USE-IT! area in 2001 and 2011. In 2001, the two largest occupational groups were elementary occupations and process, plant and machine operatives, both of which are associated with lower than average skills levels. In 2011, the occupational structure was more clearly bi-modal, with 18% of residents in employment in elementary occupations and 17% in professional occupations. This is reflected in a bi-modal qualification profile, with 29% of residents in the USE-IT! area having no qualifications (down from 42% in 2001) and 23% having qualifications at degree level or above (up from 16% in 2001).
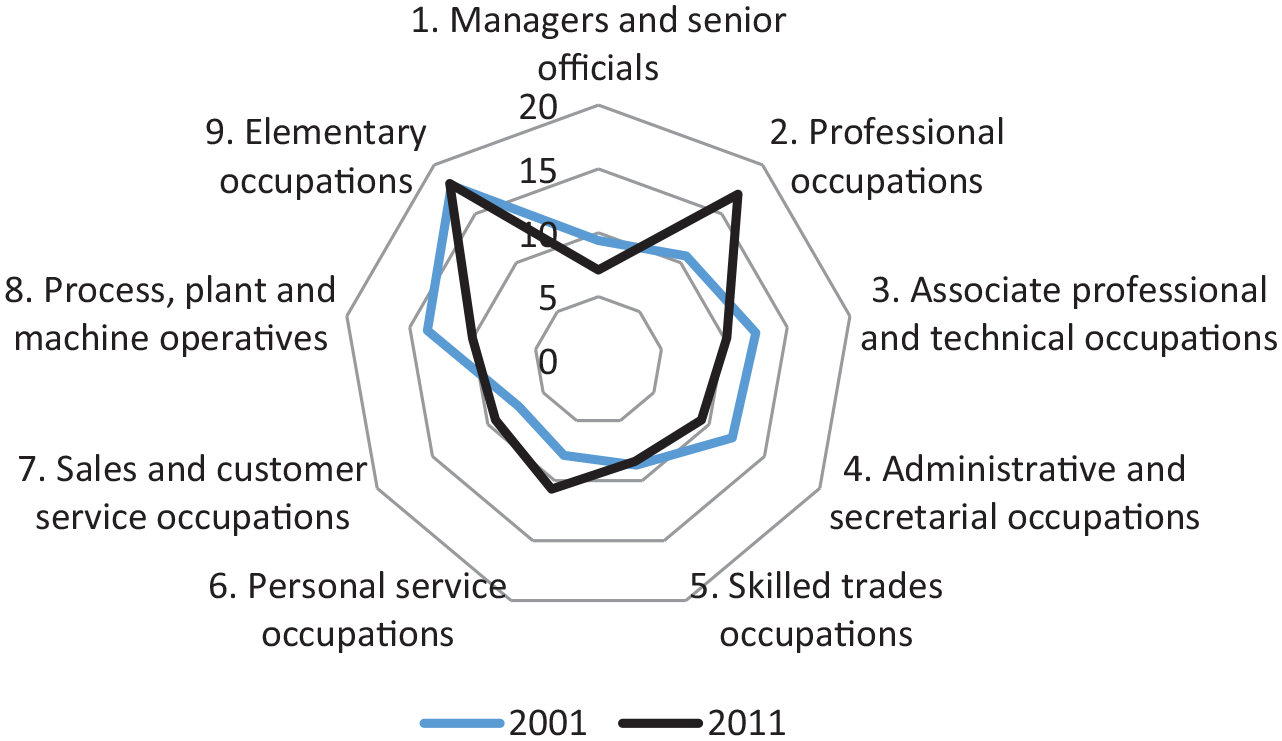
Percentage of employed residents aged 16–74 years in the USE-IT! area by occupation, 2001 and 2011.
Yet, the USE-IT! area has plenty of job opportunities. A jobs ratio of 2.17 indicates that there are more than double the number of jobs than employed residents. Moreover, the USE-IT! area is adjacent to the city centre, providing many jobs within relatively easy physical reach that residents can connect to.
Turning to the composition of employment in the USE-IT! area, data from the Business Register and Employment Survey 2016 shows that public sector employment comprised 24% of the total (compared with 23% in Birmingham and 17% in England) (ONS, 2017). The health sector was easily the largest sector in the USE-IT! area, accounting for just over 20% of employees. Hence, the health sector has potential to provide local jobs for local residents.
The case study: Skilled overseas migrants and refugees and hospital jobs
Context
The NHS is more reliant than the UK economy as a whole on workers who are non-UK nationals. Amongst doctors this reliance is particularly high: 29% of doctors in hospitals and community health services are not UK nationals. Some 38% nationally (46% regionally) gained their primary medical qualification outside the UK (Baker, 2020). Even with overseas labour, the NHS in England faces an ongoing staffing crisis, with around 100,000 vacancies nationally and a skills deficit – especially for high-level skills. Estimates indicate that in 2018 around 80% of nurse vacancies and 90% of doctor vacancies were filled by agency staff (NHS Improvement, 2019), so contributing to overspending.
The usual model of employment support initiatives in ‘deprived areas’ focuses on skills development (i.e. boosting supply of skills), targeting those with no/low qualifications. However, in the USE-IT! area a substantial minority of residents are qualified to degree level, including – as revealed by the survey co-designed with community researchers – some with medical specialities in short supply locally, so justifying a focus on seeking to recruit and utilise higher-level skills. Any intervention focusing on ‘better use of skills’ will likely involve a broader consideration of the recruitment process, recognition of overseas qualifications and a focus on possibilities for progression.
Skills matching
The focus here is on the skills-matching element of the USE-IT! project that aimed to connect skilled migrants and refugees with a medical/health background to hospital jobs. The local NHS Trust that manages City Hospital was the key organisation involved. For the USE-IT! Project, the local NHS Trust sought primarily to provide overseas migrants and refugees with the support required to move into employment opportunities within the NHS. Emphasis was placed not on lower-skilled employment (e.g. cleaning and catering), but on harnessing the previously unrecognised existing higher-level medical skills of local residents, including doctors, pharmacists and nurses, where skills shortages are acute in the NHS. An initial three-year target was set for 60 USE-IT! area residents with overseas medical qualifications to be ‘job-ready for a career in the NHS’. Importantly, the interest of USE-IT! was wider than progressing people along the journey towards employment. Rather, there was a wider strategy to realise the potential of NHS organisations as assets and anchor institutions, so that they bring maximum benefits for the communities in which they are based.
If there are local residents with shortage skills the question arises as to why previously there were not concerted attempts to address the mismatch, leaving a gap for this initiative in the USE-IT! project to fill. This situation can be explained by the fact that although the pieces of the ‘puzzle’ were in place, the mechanisms required to join them up were missing. In disadvantaged communities, available employment support tends to focus on low skills, while other personal support is often confined to ‘crisis intervention’ rather than other support that individuals might need to help them in other aspects of their lives to enable them to take advantage of available opportunities. For overseas migrants/refugees, the processes for accreditation of qualifications gained outside the UK and for meeting other requirements to work in clinical roles are not transparent. Furthermore, they are complex and costly. The hospital’s foremost objective is to provide medical care. Other considerations are of second-order importance (at least in the short-term) and are outside their primary area of experience.
In this case study, the process of linking the micro assets to the hospital (a macro asset) is shown in Figure 2. Starting on the left, the process involves engagement (including attending to basic needs) by frontline or specialist organisations that crucially have the trust of overseas migrants/refugees. These are pre-existing organisations that are active in the area. For example, in the frontline/specialist organisation panel, Ileys is a community organisation that was established in 2007 to meet the needs of the growing refugee population, Restore has welcomed refugees and assisted their integration since 1999, while EMCONET (Emerging Communities Network) is a multi-cultural organisation that was established by East European migrants to provide a range of advice on integration to UK society and economy.
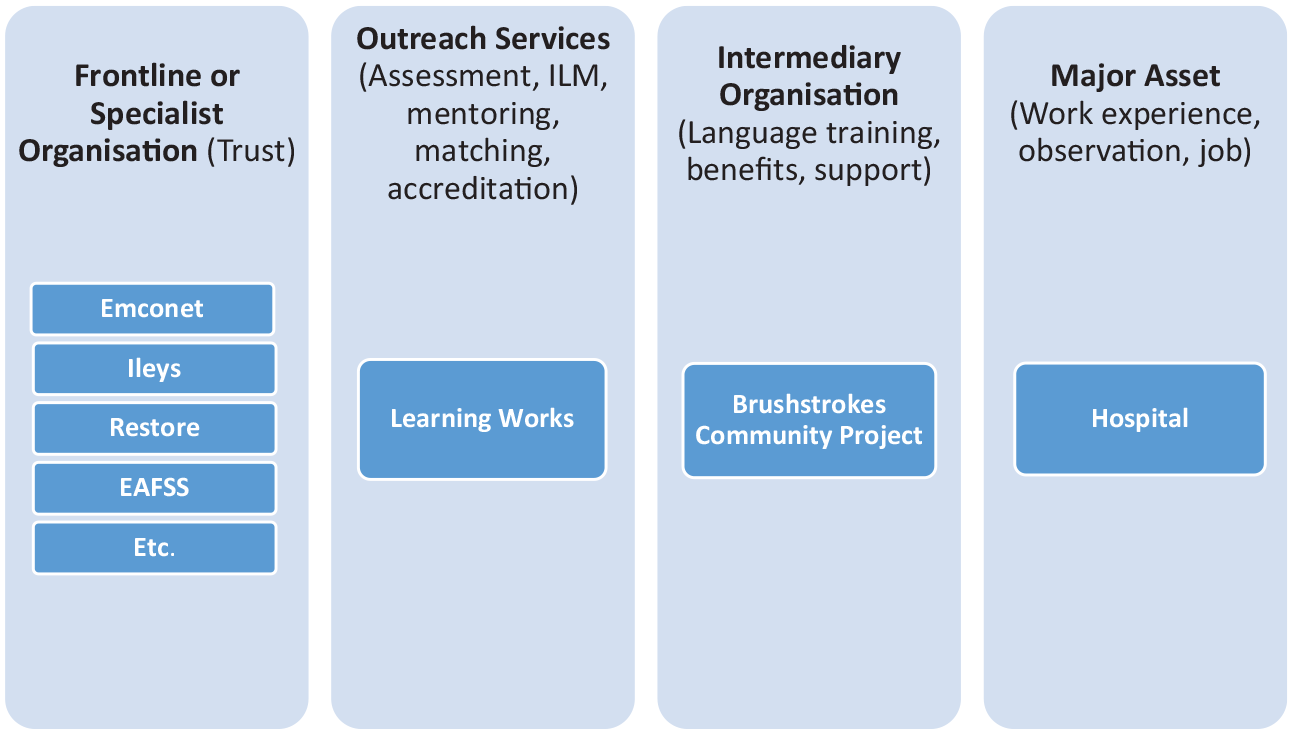
Elements of the USE-IT! skills-matching project for linking micro and macro assets. ILM: intermediate labour market.
In the next panel comes Learning Works, an organisation developed by the local NHS Trust to provide members of the community with access to professional employment opportunities and training. It is concerned with getting local people into local employment. Its establishment and activities pre-dated the USE-IT! Project, and its previous endeavours included recruiting local people into apprenticeships. Essentially, Learning Works is a one-stop shop for access to training, development and employment opportunities in the NHS. It has a physical presence in the USE-IT! area and is separate from the hospital. For the USE-IT! skills-matching initiative, Learning Works’ objective was to bring local skilled overseas migrants and refugees into jobs in the NHS. At the outset of USE-IT!, Learning Works was initially responsible for four activities: workforce skills shortage analysis and evaluation; community skills mapping; a new arrival support programme (for individuals with the right to work); and a mentoring service to provide tailored support to individuals on what the job of a doctor in the UK entails and personalised advice on career options in the NHS. For many individuals moving directly into a job commensurate with their overseas qualifications is not possible immediately, so the initial emphasis needs to be on further development of necessary skills and attributes for working in highly skilled jobs in the NHS. In practice, in several instances the delivery team at Learning Works facilitated volunteering opportunities and/or work experience in social care (where there are also labour shortages) as a precursor to moving into NHS jobs. Hence, for Learning Works working in partnership is crucial.
Learning Works connects with an intermediary organisation (see the third panel in Figure 2) to deliver benefits and other (non-clinical) support to the individuals they are working with. Here, the Brushstrokes Community Project, part of the USE-IT! project partnership, is central. Brushstrokes started in the 1990s by providing family activities, ESOL (English for Speakers of Other Languages) and IT classes for migrants and refugees, and subsequently developed to become an approved centre for immigration advice. In the context of USE-IT!, it has been responsible for the delivery of International English Language Testing System (IELTS) training. Such training turned out to be fundamentally important for skills matching. While basic support with integration was required less than initially anticipated at the outset of the initiative, the key barrier (which was greater than first expected) faced by overseas migrants/refugees wanting accreditation to move into skilled hospital jobs was the cost of the training required to gain an IELTS level 7 pass (Foord, 2019). This training costs approximately £2000 per person.
The final element in the pathway outlined in Figure 2 is the major asset: the hospital. Here work placements and observations are precursors to moving into a (permanent) skilled job as a doctor (or another specialist role).
Costs and benefits
A first step in an initial estimation of the impact of the skills-matching element of USE-IT! activity involves taking the number of current health professionals (by occupation) enrolled in the programme (as at August 2019), along with 2018 average salary figures from the local NHS Trust, examined for plausibility alongside 2018 mean salary estimates from the ASHE (the key data source on earnings in the UK). Selected key health professional roles filled by USE-IT! skills-matching participants are presented in Table 2 (and it is notable that there are 183 individuals recorded here, which is around three times the initial target of 60), alongside the number of recruits in each category. 5 The health professionals are from a range of countries, including Sudan, Somalia, Iraq, Afghanistan, Syria, Iran, Yemen, Nigeria, Eritrea, Algeria and Cuba. The final column presents a crude measure of the value to the local economy of utilising these skills if all individuals are gainfully employed in the profession that they are qualified for.
Participants in selected professions in the skills-matching work strand and salaries (summer 2019).
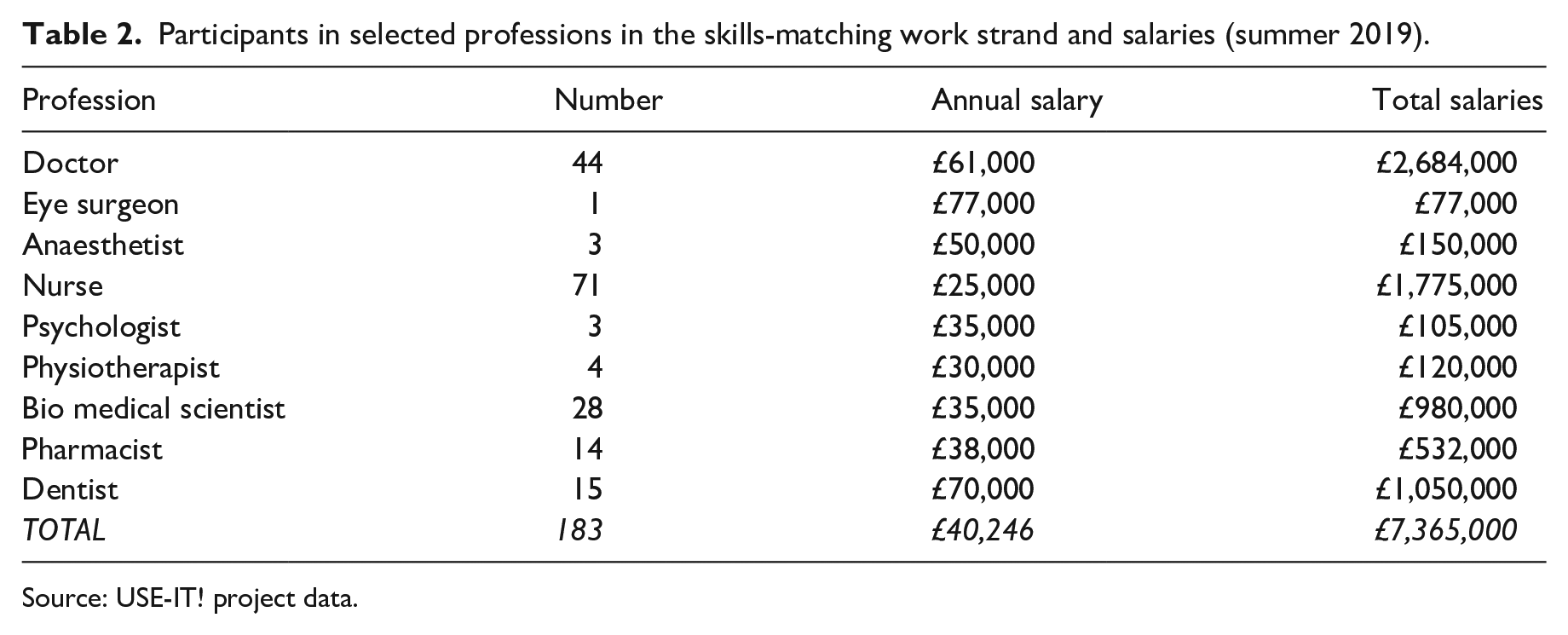
Source: USE-IT! project data.
From the hospital perspective, figures from summer 2019 suggest that the local NHS Trust spends £570,000 monthly on temporary doctors and £550,000 monthly on nursing/midwife/ambulance/technical vacancies. This corresponds to around 6% of the Trust’s monthly expenditure on salaries. Given that temporary staff are paid at a premium rate, there would be a cost saving from engaging more staff on a permanent basis. There are also cost savings in terms of benefit payments foregone from moving migrants/refugees into professional roles in the NHS. A community organisation supporting new arrivals estimated that on average a new arrival to the UK in the USE-IT! area would receive the following benefit income in summer 2019 (albeit there will be variations according to household circumstances): £317 in Universal Credit, £350 in Housing Benefit and £50 from other specialist allowances, making £717 per month and £8604 per annum in welfare benefits. Assuming that all 183 migrants/refugees in Table 2 depend on welfare benefits, total benefit costs for these 183 individuals engaged by Learning Works via the USE-IT! skills-matching initiative would be £1,574,532 per annum.
There are costs incurred in moving migrants and refugees into employment because of the need for English language training and certification. With an average cost of IELTS training of £2000 per person, the cost of this for the 183 individuals in Table 1 is £366,000. While a full assessment of the costs and benefits of delivering the skills-matching element of the USE-IT! project is not available (and would need to take account of staff delivery costs), the simple cost and benefit estimates outlined above indicate that there is a clear economic case for looking to residents to help address skills shortages, while at the same time raising incomes (and hopefully expenditure) in the local area, so lifting residents out of poverty.
Specific learning points
A key feature of the skills-matching element of the USE-IT! project is partnership working, including community sector organisations and networks alongside the macro asset of the hospital (see Figure 2). As noted by Scheffler (2019), the advantage of such community organisations is that they are locally anchored and already have the trust of the local community. These local community organisations helped to connect individuals with Learning Works, in some instances accompanying them on initial visits there. In several cases, involvement with USE-IT! enabled such organisations to develop their capacity and extend their influence more broadly within the city and beyond. Within the hospital, initiative activities involved in securing work placements, etc., for overseas migrants/refugees encouraged cross-departmental working within the hospital – especially with regard to workforce planning (which is of key importance given the skills shortages faced).
For the overseas migrants/refugees themselves, feedback indicated that participation in the skills-matching element of the USE-IT! project provided a range of benefits including (some or all of) improved social skills and linkages, enhanced communication skills, improved self-confidence and esteem, greater knowledge of the UK healthcare system, improved mental health and access to volunteering and employment opportunities. Evidence from interviews with selected beneficiaries of the skills-matching work indicated that Learning Works provided clarity on how to proceed to better utilise their existing skills: ‘Without [the] USE-IT! project I was lost. I didn’t know from where to start to be honest. . .it was really difficult. Here. . .everything [is] clear. I’m going to pass the IELTS, and after that I will start the clinical attachment’ (a participant on the programme) (Foord, 2019: 19). The bespoke nature of the support provided was regarded as crucial by beneficiaries and staff at Learning Works, with existing medical professionals providing vital mentoring support. As the quote above illustrates, a key challenge facing overseas migrants/refugees is the complexity of existing employment support services and their generic and siloed nature, as opposed to the more bespoke nature of skills-matching support in developing individualised learning and support pathways, involving the NHS and community partners, as developed in the USE-IT! project.
The activities that participants engaged in also have the potential to lead to a range of knock-on benefits for their families, economically through higher income from sustainable employment within the NHS and socially through more effective links to voluntary and community sector organisations in the local area, providing a range of wraparound support services. For the neighbourhood itself, an increase in residents’ earnings can have subsequent knock-on effects for local shops and services. 6
Arguably, perhaps the key learning point from the skills-matching work strand is the importance of English language skills support to enable skilled migrants and refugees to enter NHS jobs commensurate with their skills. While the importance of English language skills has long been recognised as important for successful labour market engagement in most occupations and sectors, by far the most important and effective support mechanism offered was English language classes, training and qualifications.
The approach and system pioneered in the skills-matching element of USE-IT! in terms of realising the hospital’s role as a macro asset, in joining up local organisations and in providing targeted support has been rolled out further in the Greater Birmingham area. The local NHS Trust has worked with some adjacent Hospital Trusts on rolling out a new project – Healthcare Overseas Professionals (HOP). Principles of the learning are also being extended to groups disadvantaged in the labour market, including ex-offenders and care leavers, with support from Health Education England (a body concerned with developing the current and future healthcare workforce). This underlines the broader applicability of the approach.
Discussion and conclusion
The skills-matching element of the USE-IT! project provided dedicated resources to help the identification, engagement and support of migrants/refugees living in the local neighbourhood who had medical qualifications (i.e. micro assets) but who were not working in the NHS, and sought to link them to job opportunities in the NHS commensurate with their skills. By summer 2019 it had placed 183 migrants and refugees with medical qualifications (from outside the UK) – more than three times the initial target – in health-related jobs commensurate with their skills, so increasing their earnings while also helping the NHS to address skills shortages. Provision of English language support, work placements, peer mentoring and other wraparound support (as necessary) from community organisation partners was crucial in facilitating the services necessary to enable this utilisation of higher-level skills.
This case study highlights that several policies need to be in place to catalyse links between micro assets and a macro asset (in this case the hospital), if the latter is to realise its full potential as an anchor institution. The evidence suggests that three components linked to different forms of entrepreneurship and leadership are needed, chiming with Sotarauta et al.’s (2021) investigation of the role different actors play as agents of change in the rather different context of green path development. The first component in the USE-IT! case study initiative is strategic buy-in from senior managers at the hospital as they re-evaluated their anchor institution role as a key employer within the local community. This may be considered as institutional leadership. The second component is what Sotarauta et al. (2021) refer to as innovative entrepreneurship, which provides the delegated responsibility (with investment) for implementation. Here, an important feature in the USE-IT! case was that Learning Works was already established in the community, representing a significant shift in the management approach of the hospital in relation to local people and their employment. Adaptation of human resources policies and processes enabled a change in organisational strategy to develop mutually beneficial relationships with the local community, including voluntary organisations. The third key component is the vision and place leadership that provided the strategy, resources and boundary spanning activities that were critical in constructing and maintaining a new diverse partnership (Beer et al., 2019) that was central to building the bridge between the macro asset and the local community. In resource terms, the availability of European funding (awarded before Brexit) for the USE-IT! project was especially pertinent. The funding enabled the public sector and the voluntary and community sector to come together to work towards common outcomes, and act (at least at the outset) as an interpreter between the local community and the hospital. The challenge moving forward is to devise an operating model that can be sustained without a one-off relatively large volume of funding, especially given that seemingly all three components identified above needed to be in place to unlock the hospital’s potential as an anchor institution to address employment and other local inclusive growth issues. Further research, including in different institutional contexts, would be valuable here to build knowledge on possible ways forward to sustain, further embed and scale up examples of good practice.
The case study highlights that the necessary resources to link micro and macro assets already existed in this particular local area in Birmingham – and will also exist in many other areas in the UK and elsewhere, including in European cities that have attracted migrants/refugees and face similar challenges of governance and management in the face of increasing diversity (Raco and Tasan-Kok, 2019) and where work integration initiatives are predominantly implemented at the local level (Syrett and Sepulveda, 2012). This means that learning points from the USE-IT! skills-matching work strand are likely to be transferable, so providing crucial lessons for performing ABCD/anchor institution development elsewhere. What was lacking at the outset in the case presented here was the mechanism to join up the assets. It was not that the will to join up did not exist; rather, it was that individual organisational priorities were paramount. There was insufficient time and no obvious space in which to build up the relationships of trust that needed to be in place across a partnership of diverse actors to build an effective bridge between micro and macro assets. Building the capacity of all local actors is important for inclusive growth and can take a long time.
The article has shown how a macro asset (a particular hospital) located in a deprived superdiverse neighbourhood has gone some way to realising its anchor institution role by connecting local residents (i.e. micro assets) to employment opportunities. Importantly, it has not focused solely on those with no/low skills who are the traditional subject of regeneration programmes in areas of concentrated spatial disadvantage. Rather, it enhanced its awareness of the skills available amongst local residents and sought to utilise them. As such, the case study underscores the efficacy of neighbourhood regeneration approaches that look beyond a traditional emphasis on those in skills poverty to focus instead on improved skills utilisation and its contribution to inclusive growth. To do so, it acted to hone and mobilise those skills by adapting and extending its conventional skills development and recruitment activities to work in partnership with local community and intermediary organisations (to provide wraparound and targeted language support and source work experience placements) and its own workforce (to provide mentoring). In so doing, it demonstrated that anchor institutions need to be agile and responsive to changes in circumstances in their own neighbourhoods and cities if they are to move from a position ‘in the city’ to one ‘of the city’. Hence, this article contributes to a growing literature on a positive role for anchor institutions in urban economic development and also underscores the point that the collaborative relationships required for interventions that have potential to enhance cities need to be actively constructed by diverse actors (Vallance et al., 2020). This is an area ripe for further research, especially given growing interest in local anchor networks and community wealth building.
While the case study material presented in this article relates to the position in 2019, subsequently in 2020/2021 the Covid-19 pandemic has deepened understanding of the crucial role of migrants/refugees as key workers in the healthcare sector in Birmingham, the UK and elsewhere. It has underscored the importance of effective skills utilisation. More broadly, it has focused attention worldwide on shortages of medical staff, bringing into sharp relief issues of reliance of some countries (such as the UK – especially as it moves to a post-Brexit immigration regime) on importing skilled labour that is also needed elsewhere, so highlighting links between global geopolitics and anchor institution development strategies. In turn, this highlights the importance of multi-scalar perspectives in future research on these topics.
Footnotes
Acknowledgements
The authors wish to thank the following colleagues at the University of Birmingham for their leadership and input to the USE-IT! project (![]() ): Dr. Peter Lee (Project Lead and Principal Investigator - responsible for USE-IT! Project design) and Dr. Sara Hassan, together with all partners in the USE-IT! Project, notably Karolina Medwecka-Piasecka, USE-IT! Project Manager European and International Affairs, Birmingham City Council, and participants in the research.
): Dr. Peter Lee (Project Lead and Principal Investigator - responsible for USE-IT! Project design) and Dr. Sara Hassan, together with all partners in the USE-IT! Project, notably Karolina Medwecka-Piasecka, USE-IT! Project Manager European and International Affairs, Birmingham City Council, and participants in the research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the EU Urban Innovative Actions initiative, which provided funding for the USE-IT! Unlocking Social and Economic Innovation Together project.