
Abstract
Introduction
For decades dementia scholars have focussed on how people living with dementia, due to their declining cognitive skills, risk being perceived by formal caregivers as someone without personhood.1,2 The nature of dementia, characterised by cognitive impairment, disturbs the existing conceptualisation rooted in modern societies, where rational thought, coherent memory, and purposeful communication are regarded as valued assets of exhibiting one’s personhood. Accordingly, our conception of dementia may suggest to us that there is a loss of personhood in those who are unable to express themselves. 3 Something that raises a vital ethical issue due to the fact that when people are recognised as lacking personhood, they count as less and there appear to be no good moral, psychological, or social reasons for nurturing or guarding their lives compellingly.3,4 Unfortunately, such detrimental effect in dementia care practices is well-documented.2,5,6 This ethical issue is highly relevant to contemporary societies across the world, as not only growing numbers of people will be living with dementia 7 but also the increased focus on improving dignity in dementia care practices 8 as well as developing new ways to maintain their personhood. 4
Background
To date, arguably the most well-known and accepted effort to address this ethical issue is Kitwood’s 2 seminal work on person-centred care. Such an approach requires formal caregivers to understand and maintain the concept of personhood in those they care for, which entails supporting care recipients’ sense of self. Something that is essential for high-quality dementia care. 9 Nonetheless, formal caregivers can struggle to accept and interpret personhood when dementia progresses into later stages of cognitive impairment (often referred to as ‘advanced dementia’ and how the term is used in this paper), leading to the fundamental ethos of person-centred care becomes lost. 10 Despite the fact that person-centred care has become the primary focus for dementia care practices in Western settings 9 loss of sense of self from the perspective of the person living with dementia still asserts itself in care practices, 11 where nursing home residents living with dementia experience poor individualised care6,12 characterised by social exclusion, 13 containment, 14 and wide use of antipsychotics. 15 Scholars argue that the way the notion of personhood is understood in person-centred care, as something that is bestowed by the caregiver, is too narrow and static. Such a view of people living with advanced dementia fails to acknowledge them as active agents capable of supporting their own personhood through their subjective experiences of living in the world and with others.16–19 In short, the concept of personhood used in person-centred care undervalues essential philosophical elements of what it means to be a fully human being living a life with a dementia condition through all its stages.
The concept of personhood remains contentious in metaphysics and moral philosophy. 20 However, some innovative studies have broadened the view of personhood by taking a more existential approach to the dimensions that can make a person feel as human, thus, ‘can counteract notions of unravelling personhood’ ( 21 p.19) and ‘offer helpful nuances of meaning that the term ‘personhood’ and ‘person-centred’ care may obscure’ ( 22 p.882). These studies are based on Galvin and Todres’ 23 Lifeworld-led care theory, that highlights the notion of humanisation and seeks to guide a more ethical human sensitive care. They state the existential can act as a means to deepen our knowledge of the human experience of living through life ruptures. Such existential knowledge can help direct caregivers to provide care that acknowledges care recipients’ personhood in all its human complexity. 23 Thus, the complexities of personhood (or loss thereof) in caring relations would more adequately be understood as a spectrum of existential forms of humanisation and where these are not guarded, kinds of dehumanisation. Insights into dehumanisation of people living with dementia can support formal caregivers to maintain personhood in dementia care. 24
Dehumanisation is defined by Smith 25 as someone’s attitude towards another person, where this other is perceived as having a less-than-human essence. Research related to people living with dementia demonstrates how dehumanisation may be embedded in the common understanding and description of them in political, cultural, and professional rhetoric and metaphors. People living with dementia are depicted as ‘zombies’, 26 ‘dementors’, 27 ‘vulnerable monsters’, 28 and ‘vacant and draining bearer of their condition’. 29 Life with dementia is described as a ‘never-ending funeral’, 30 a ‘prescribed disengagement’, 31 a ‘cosmic confusion laced with terror’, 32 and a fate ‘worse than death’. 33 And dementia and its progressing uncurable nature are portrayed as a ‘silent tsunami’, ‘millennium demon’, 27 ‘merciless assault’, 33 and ‘our greatest killer’. 34 All of which clearly illustrate how people living with advanced dementia are painted on a canvas of negative stereotypes and societal fear on which a dehumanising ideology of dementia in Western world can grow.
Although it is important to recognise and challenge ideologies that may reinforce dehumanisation, this is not the sole solution; otherwise refuting the ideology would be enough to resist dehumanising attitudes. Smith 25 emphasises that it is essential that we also pay attention to the psychological dimensions of dehumanisation and understand how ‘dehumanising impulses’ unfold inside people if we are to oppose them. Most formal caregivers want to do a good job and will claim to be acting in the best interests of their care recipients. However, it is critical to acknowledge that dehumanising attitudes are not necessarily seen in people who are evil or cruel but can occur imperceptibly in anyone. Just as dehumanising attitudes not only relate to excessive violence but also more subtle everyday forms of bias.25,35 As dehumanisation is both societal and psychological it is important that we both understand the cultural and political ideology outside ourselves as well as the impulses inside us. 25 Given the extensive literature describing dehumanisation in dementia existing outside the caregiver, there exists a need to understand the psychological roots that might elicit dehumanising attitudes inside the caregiver. While research on the psychological aspects of caregivers’ dehumanisation of people living with dementia has started to sprout, 24 such knowledge is still scarce and has not systematically been examined in detail.
We acknowledge the growing body of research aiming to maintain personhood and uphold human dignity of people living with advanced dementia, work that often focuses on ways to recognise and make visible the person behind the dementia condition and its obfuscations. However, scholars investigating dehumanisation outline how a better understanding of dehumanisation processes towards certain groups of people can teach us a lot about these groups’ humanity. 36 Thus, an alternative perspective may be pertinent, wherein the concept of personhood in advanced dementia is examined inversely, emphasising instances where recognition of personhood is absent. Inspired by Galvin and Todres’ existential approach to personhood, we suggest that supporting and maintaining personhood in people living with advanced dementia requires us to identify what might elicit dehumanising attitudes in dementia care practices. And acknowledging how attitudes are shaped by our perceptions, 37 we wish to explore how formal caregivers’ perceptions of people living with advanced dementia can inhibit their sense of feeling as human beings in caring relations. This review addresses the research question: which perceptions of people living with advanced dementia can elicit dehumanising attitudes among formal caregivers?
Method
Theoretical underpinnings
The concept of dehumanisation is understood and used with great diversity in the literature. Based on Smith’s definition and Galvin and Todres’ human care theory, our study views dehumanisation as a psychosocial existential phenomenon that exists in caring relations. Therefore, we apply Galvin and Todres’ 23 eight forms of dehumanisation, that individually and together describe how care recipients are hindered to feel as human beings. We also examine how formal caregivers’ attitudes may obstruct such feelings of being human among care recipients living with advanced dementia. As such, the selection and analysis process of the review were focussed on how formal caregiver perceptions could make people living with advanced dementia feel like: (1) objects without subjectivity (objectification), (2) submissive recipients of stimuli without responsiveness (passivity), (3) categories without uniqueness (homogenisation), (4) alienated without sense of belonging (isolation), (5) standards without individual feelings and experiences (loss of meaning), (6) cases without past and future lives (loss of personal journey), (7) separated without sense of familiarity (dislocation), or (8) physical bodies without meaningful connections to the world (reductionist view on the body). In other words, if the perception of the caregiver was recognised as possibly leading to any of the abovementioned forms of not feeling as an (existential) human being, it was characterised as a dehumanising attitude. In this way, the eight forms were used in our study to identify formal caregivers’ unintentional dehumanisation of people living with advanced dementia in the literature. We also used them to direct the initial stages of our analysis. However, we did not attempt to fit our findings to these eight forms.
Literature review
To answer our research question, we conducted an integrative review incorporating multiple perspectives and types of literature (qualitative- and quantitative studies as well as theoretical- and grey literature) about caregivers’ dehumanising attitudes of people living with dementia. Integrative reviews hold the potential to contribute to comprehensive descriptions of the phenomenon in concern, as it allows us to examine and summarise the phenomenon through the broadest kind of knowledge. 38 To ensure rigour in the systematic literature search, the search strategy was based on a population (person living with advanced dementia), phenomenon of interest (dehumanisation), and context (formal caregiver’s attitude) (PICo) structure, and a preliminary search was carried out in collaboration with an experienced research librarian. Through this initial work, relevant keywords and databases were identified. In this regard, keywords for dehumanisation were derived both from general theoretical conceptualisations of the phenomenon and how it directly has been related to dementia. Thus, dehumanisation, infrahumanisation, objectification, alienation, depersonalisation, pathologisation, medicalization, stereotyping, and stigmatisation were used in searches with both American and British spelling and truncation. Furthermore, it became apparent that, although the research question is focused upon ‘advanced dementia’ and ‘formal caregivers’, these aspects needed to be omitted in the search itself to broaden up the scope of the search; otherwise, the number of hits simply became too small or non-existent.
As recommended for integrative reviews, the scope of the systematic literature search was broadened into several phases.
38
To begin with keywords were used in scientific subject specific (CINAHL, PubMed, Embase, and PsycInfo) and scientific interdisciplinary (Web of Science, Scopus, and Google Scholar) databases to search for quantitative and qualitative research as well as theoretical literature. Furthermore, a search for grey literature was made in Google Scholar and Open-Access Theses and Dissertations (https://oatd.org). Thereafter, additional searches were made consisting of queries to subject experts, hand searching in relevant journals, and citation searching based on reference lists from relevant resources. All hits from all searches were imported into Covidence (a screening and data extraction tool for conducting systematic reviews) which was used throughout the identification and screening process and a flowchart was drawn from here (see Figure 1). Flowchart illustrating the screening and selecting process.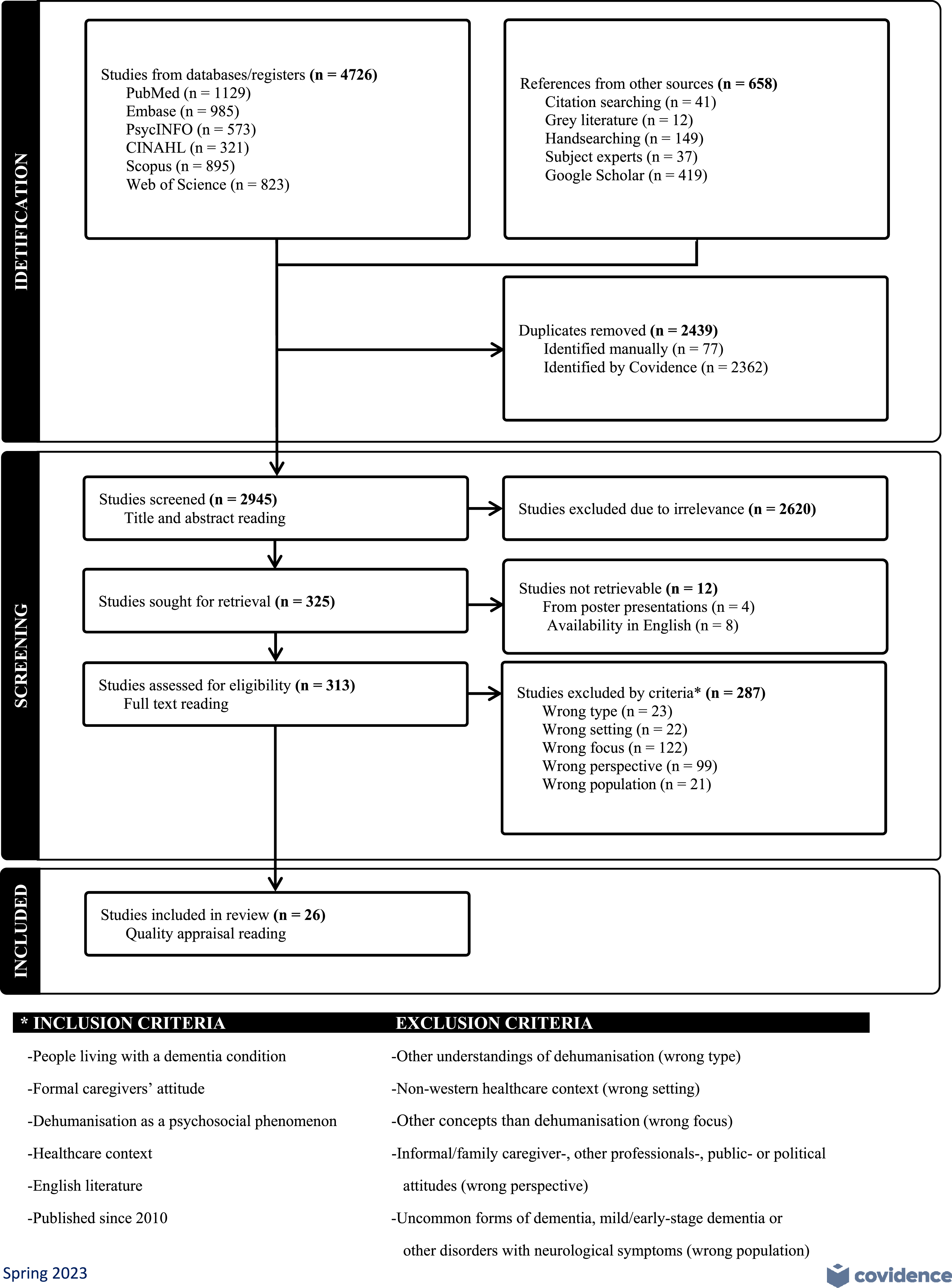
Data evaluation
First, all hits were screened based on title and abstract for eligibility and relevance. Then, relevant literature was obtained as full text, read, and reviewed according to pre-determined inclusion and exclusion criteria (see Figure 1) as well as how it regarded ‘advanced dementia’ and ‘formal caregivers’. Various recommended and validated assessment checklists were used in the quality appraisal of the selected literature, due to the inclusion of both empirical and nonempirical literature in the review. 38 Thus, grey literature was assessed based on the AACODS checklist, 39 theoretical literature based on the Walker and Avant procedure, 38 and both qualitative and quantitative research articles based on the standardised Mixed Methods Appraisal Tool (MMAT). 40 None of the texts were excluded by this quality appraisal, and 26 texts were eligible for analysis consisting of eleven qualitative and four quantitative research articles, two dissertations, one ethnography, and eight discussion papers. The whole screening, assessing, and selecting processes were done by the first author. However, to secure reliability in the process due to the large number of articles involved, the last author was consulted on verification of eligible literature while both authors looked at a random sample (15%) of the relevant literature and selected literature. Quality assessment of the random selected literature sample was done interpedently by both authors, 41 and no disagreements arose from this. The entire review process was conducted throughout April–May 2023 and has the Prospero registration number CRD42023373901.
Data analysis
Data matrix of sources reviewed.

During the first phase of analysis, data reduction, all 26 articles of different types of sources (theoretical-, quantitative-, and qualitative papers) were read thoroughly. Throughout this full-text reading, descriptions of caregivers’ dehumanising attitudes towards people living with advanced dementia were identified and divided into subgroups based on the dehumanisation forms. In the second phase, data display, physical printouts and NVivo (version 14) codes were used to visualise and collate the findings from all the subgroups. In the third phase, data comparison, data displays of the findings were looked over for connections and patterns in caregivers’ dehumanisation. To secure rigour in this phase, a triangulation process between the first, second, and last author was made, while the data were examined iteratively and patiently allowing the results to slowly become clear. This led to the fourth and final phase, conclusion drawing and verification, in which the identified relations of particular findings were raised to a higher level of abstraction and synthesised into five general themes capturing formal caregivers’ dehumanising attitudes towards people living with advanced dementia.
Findings
Five themes are formulated that express the perceptions that can elicit dehumanisation among formal caregivers. This happens when people living with advanced dementia are perceived as (1) absurd, (2) shadow, (3) perilous, (4) void, and (5) repugnant. Individually and together the themes summarise how perceptions of people living with advanced dementia elicit dehumanising attitudes among formal caregivers in dementia caring practices. As such, each theme synthesises the individual perceptions found in the individual articles of the primary sources, where the eight forms of existential dehumanisation became visible in our analysis. Galvin and Todres 23 posit that the eight forms are best understood as overlapping each other rather than as discretely independent. Thus, summarised themes of dehumanisation can illustrate more than one of the forms, as intertwined, which is the case in our five themes. Still, it should once more be emphasised that dehumanisation is not necessarily deliberate.25,35 This was also evident in the individual articles’ descriptions, where caregivers appeared mostly unaware of their dehumanising attitudes and seemed to have the care recipient’s best interest in mind and also showed examples of more humanising attitudes towards people living with dementia.
People living with dementia as absurd
Formal caregivers risk being dehumanising when they perceive people living with advanced dementia as someone unaware of what they are doing and devoid of reason. This happens when the behaviours and action of people living with dementia are viewed as unsound so as not to be taken seriously or lacking any meaning, thereby reflecting forms of absurdity – meaning a state of being ridiculous or wildly unreasonable. 43 A close look at the reported perceptions of absurdity allows us to categorise it in two sub-themes, where people living with dementia are understood as incompetent and unable to act meaningfully.
Acting incompetently
Caregivers interpret the behaviour of people living with dementia as signs of their confusion, loss of autonomy, or lack of control.44–46 As such, the behaviour is regarded as irrational manifestations of their incompetence to perform independent actions,44,47 to act for their own benefit,48,49 to pursue a specific purpose,46,50 or to express a unique need.51,52 Thus, the behaviour of people living with dementia was understood by caregivers as something acted out by persons unaware and unable of understanding what they were doing and why they were doing it. For example, if a person living with dementia went outside the care facility, left their hospital bed, walked around in the ward, opposed to the care, or tried to strip off their bed linen or clothes, the caregivers didn’t think about or were not curious as to why such behaviour had surfaced. Instead, it was understood as incompetent and lacking agency and reason and, therefore, something that needed to be corrected and controlled.46,50,52–56
Acting meaninglessly
The behaviour of people living with dementia was often considered by caregivers to be based on the impaired functions of the person rather than on how the dementia affected this person living in the world with such a condition.57,58 This meant that their behaviour was not seen as containing any meaning from the perspective of a person living with dementia but instead attributed to illogicality,56,59 madness,57,60 or impaired cognitive symptoms.48,58 In other words, people living with dementia were perceived by caregivers as someone unable to interact in meaningfully psychosocial-,13,61,62 communicative-,48,54 or lucid ways.49,50,57 This meant that attempts to communicate about or reflect on underlying reasons for the actions of the person living with dementia were limited or completely omitted.26,47,48,50,63 For example, if people living with dementia acted by withdrawing themselves from social activities, 63 becoming repetitive in their actions and language,44,48 or opposing to the measures done to them, 57 such action may be seen in the eyes of caregivers as meaningless resistance to care,46,59 meaningless combativeness,57,64 meaningless social-, physical-, or personal needs,47,53,61 or meaningless irritating utterances.44,48
People living with dementia as shadow
Formal caregivers risk being dehumanising when they perceive people living with advanced dementia as unable to communicate intelligibly and express their personal story. This happens when the narrative of people living with dementia is heard or told as representing somebody who is not really there or who is just a diagnosis, not a person, thereby reflecting forms of shadows – meaning a darkness in which a person cannot be seen. 65 A close look at the reported perceptions of shadow narratives allows us to categorise it in two sub-themes, where the perception of people living with dementia leads to caricature of them as being empty shells and ‘demented’ care recipients.
Being empty shells
Caregivers may interact and communicate (verbally and nonverbally) with people living with dementia as if they are merely physical bodies, where the person inside basically has disappeared due to the effects of the condition.58,66 Their person becomes indistinctly lost in the darkness of dementia. This may happen when a person living with dementia is perceived as someone detached from the person they once were,46,53 clueless as to who they are,52,63 emotionally empty,45,51 and incapable of understanding anything.44,61 These losses of former and present self-understandings are manifest when care recipients’ communication of their own desires for appearing as they once did, 67 holding on to familiar rituals, 49 wanting to go home, 56 and possessing personal items 46 are ignored or devalued by the caregivers. In such circumstances, caregivers may carry on interactions and communication with the care recipients as if nothing of importance has been uttered.47,56,61 As for the emotional emptiness in people living with dementia, caregivers may not consider how their actions affect the care recipient. This means that the potential emotional impact of the care interactions on the person living with dementia and their responses are not recognised and only explained in the mind of the caregiver as part of an empty interior.13,50,67
Being ‘the demented’
Caregivers may nurture a narrative about people living with dementia as nothing more than the loss of their cognitive abilities. This stems from a biomedical notion of what it means to have dementia.26,48,57 As such, living with dementia is reduced to biomedical symptoms and impairments, where behaviour that might otherwise be regarded as normal is interpreted as evidence of neurological pathology.57,62,66 So individual and personal responses, actions, and expressions may be positioned by the caregivers to be the result of cognitive decline and feed into an account that these are typical dementia behaviours.57,66 As such, taking a walk becomes positioned as disruptive wandering, 50 sexual activity as disinhibition, 49 anger as overt aggression, 60 or incomprehension as being deviant. 63 This approach may generate a discourse where people living with dementia are referred to as ‘demented’, indicating that they are no more than their diagnosis.26,57,60,66 The dehumanising narrative of the ‘demented’ is not only established in caregivers’ verbal accounts but also in their nonverbal concept of how a ‘demented’ care recipient looks. This may reflect the caregivers’ and the institution’s priorities.45,49,52 An example is how personal familiar clothes of a person living with dementia may be rejected for loose-fitting and institutional garments.45,46 Other examples are when they are dressed and groomed to be decent, covered, and clean care recipients49,53 or, conversely, may be left visibly unkempt, scruffy, and with bibs and spillages on their face and clothes from a previous meal. 46
People living with dementia as perilous
Formal caregivers risk being dehumanising when they perceive people living with advanced dementia as people that always endanger themselves and those around them. This happens when the person living with dementia is felt unnaturally fragile and wearisome, something that provokes not tenderness but is disturbing and somehow threatening, thereby reflecting forms of perilousness – meaning causing a dangerous or unsafe risk. 68 A close look at the reported perceptions of perilousness allows us to categorise it in two sub-themes that may foster a constant unsettling sense of people living with dementia as being a danger not only to themselves but also to their caregivers.
Posing danger for themselves
Caregivers experience a person living with dementia as someone constantly at a risk of damaging oneself, even in cases where it does not necessarily apply. This may be a perceived risk of physical danger manifested, for example, in preventing people living with dementia from going out for unreasonable or exaggerated fear of them getting hurt or lost.50,56,59 Or it could be that the caregivers did not regard them as able to do anything good for themselves.55,60,63 Thus, the care practices may be adapted, according to how caregivers think they may be protected from themselves by controlling, restricting, and restraining them.59,69 Use of antipsychotics, 55 hidden doors and exits, 56 false information, 44 tiring the person out, 48 paternalistic care, 47 or containment at the bedside 50 are all measures used for securing their safety. Some caregivers even expressed a need for keeping a person living with dementia under constant surveillance by always having them in sight 64 or using trigger alarms when they moved about. 56 It is not only physical danger that caregivers needed to protect people living with dementia from but also emotional danger. As such, caregivers may suppress imparting honest information about medication, invasive procedures, or life events such as the loss of a loved one.44,54,56 It was perceived to be emotionally better for care recipients living with dementia to remain ignorant 54 and left happier in their own world. 44
Posing danger for the caregiver
If a person living with dementia acts or responds aggressively to the surroundings57,64 or expresses oneself assertively,49,69 it may be regarded as posing a danger to the caregivers. This behaviour is then immediately considered as challenging and problematic, and something that should be opposed, even though in fact such behaviour could be understandable given the situation persons living with dementia see themselves in. Such as, getting aggressive when being forced to do something you don’t understand nor want. 60 Sometimes this experience of danger among caregivers is based on their own experience of past behaviours and situations rather than on what is happening in the actual moment.54,56,64,66 People living with dementia may become defined by caregivers according to such present or previous behaviours, thus becoming labelled as wanderers, violent, or disinhibited. This can lead not only to their behaviours being misunderstood but also who they are as persons.48,57,64
People living with dementia as void
Formal caregivers risk being dehumanising when they perceive people living with advanced dementia as living lives where nothing in it generates any value for themselves or others. This happens when the life of a person living with dementia is seen as emptied of enjoyments, hope, and simply not worth living, thereby reflecting forms of voids – meaning a completely empty space. 70 A close look at the reported perceptions of voided lives allows us to categorise it in two sub-themes where people living with dementia are seen either as passive care recipients or as living dead.
Resembles passive recipients of care
In caring for people living with dementia, the caregivers may perceive those cared for as an object for which it is only necessary to meet bodily needs. Investing in everyday enjoyments or positive activities is not worthwhile.44,69 Task-orientated care approaches are dominant among caregivers who overlook how care practices could be experienced and enjoyed by the care recipient. Responding to essential and normally pleasurable needs such as food, sleep, social and meaningful activities, or bathing becomes a chore to be completed and is not seen as a possible source of pleasure for the person cared for. Examples include people living with dementia being bathed at the same time as they were on the toilet, 61 being clothed as if they were mannequins, 53 disturbance of their individual eating and sleeping patterns for institutional convenience, 49 obliging them to attend social activities that were meaningless to them,63,69 or caregivers avoiding any personal interactions.51,61 Verbal and nonverbal, or embodied, communication of individual desires by people living with dementia often goes unrecognised,63,66,67 and care interactions may become limited to merely meeting basic bodily needs with minimal interpersonal interplay.26,46,53,58
Resembles ‘the living dead’
A similar null image was visible in caregivers’ perception of the general life of people living with dementia, which in their mind often contained only loss and no hope.55,57,58 People living with dementia were perceived through a lens solely focused on their cognitive and functional losses and, therefore, how they would be expected to behave and what they would not be able to do.58,60 This perception not only includes the actual cognitive losses but also about the prospect of future deterioration, even if the person is managing at present. Thus, regardless of the degree of impairment a person living with dementia may be seen as someone who should retire from life,57,69 inevitably has to be moved into a care home13,58 and is unable to regain50,64 or learn new skills.66,69 In effect, that they practically were already dead.26,62 Intrinsically, this view sees the life of people living with dementia as being the existence of people, where any taste of freedom, ease, pleasures, or well-being are impossible. As such, caregivers may regard the person living with dementia locked in a life without hope, no room to breathe, or nowhere to escape. 60
People living with dementia as repugnant
Formal caregivers risk being dehumanising when they perceive people living with advanced dementia as unpleasant and unappealing, and consequently as being without dignity. This happens when people with dementia are sensed with disgust, as old, foul, and decaying bodies and, thus, working with them is of low status, thereby reflecting forms of repugnance – meaning a feeling of strong dislike or disgust. 71 A close look at the reported perceptions of repugnance allows us to categorise it in two sub-themes evoking ideas of people living with dementia as being either undignified repulsive bodies and/or unworthy abject others.
Considered repulsive bodies
As dementia care includes caring for an old, ill, and declining body,52,62 a central task and element for the caregivers is doing direct hands-on activities in handling, assessing, and manipulating the other person’s body. 67 This work disturbs the norms for the treatment of the body, where, especially in people living with advanced dementia, it involves what is considered the negatives of the body.49,67 An older person living with dementia may lose control of their bodily functions and suffer from urinary and faecal incontinence,45,67 as well as difficulties maintaining personal hygiene, problems with eating, or inattention to their bodily needs.46,52 This may be amplified when a person living with dementia resists the caregiver’s attempt to help or clean them and, as a result, has to use force, mislead, or simply let them be.44,56,66 All of these came to signify what was considered by the caregivers as dirty, disgusting, and demeaning work around the undesirable functions of a grotesque body.49,52,67 Thus, the caregiver’s focus may be on the objective deficit of a physically repulsive body without considering the person behind the condition55,57,69 and their dignity.46,66,67 In the worst cases, people living with dementia may be perceived as someone for whom dignity is not important 44 or even possible 66 and therefore someone unworthy of respectful and empathetic care.13,26,64,67
Considered abject others
Being perceived as someone unworthy of respect, empathy, and without dignity is also distinct in how caregivers give individual status to a person living with dementia. Simply providing care through bodywork49,67 and working with chronic diseases of older people, and in geriatrics as a whole,45,64 is ranked very low in terms of prestige and importance among caregivers. Furthermore, caregivers work in a climate characterised by an ageism that represents negative stereotypes, prejudices, and discrimination against older people. This is based on their age or the perception of them being weak, dependent, and vulnerable,47,62,69 as well as a hypercognitive culture that holds rationality, cognition, and memory as core aspects of a person’s human value.51,60,66 All these bodily, mental, and societal dimensions may contribute to the low significance attributed people living with dementia if they are seen by the caregivers as an abject other who does not demand respect and dignity.26,49,52 The insignificance, lack of respect accorded, and indignity of these abject others in the mind of the caregivers are shown when their behaviours and emotional expression are ignored,48,56 they become invisible in the wards,13,50 and are left facing the wall separated from others at mealtimes or waiting for hours on a non-existing bus at a fake bus stop.44,66
Discussion
Based on our analysis, formal caregivers may perceive people living with advanced dementia in such a way that fosters attitudes of these care recipients as being less than humans. This happens when formal caregivers perceive this group of people in caring relations as acting absurd, being a shadow, posing perilousness, resembling a void, or considered to be repugnant.
Our findings show how dehumanising attitudes can be elicited when a person living with dementia is perceived as someone who needs to be contained, restricted, or adapted to direct their everyday life so as not to disturb or endanger it. This pattern is in accordance with what has been identified as a special care-choreography, where the main purpose for caregivers in a nursing home is to sustain calm. 72 Caregivers choreograph everything from how moods, people, timeslots, and the surrounding space should be arranged in relation to each other, to ensure that calmness can occur. This orderliness requires that residents living with dementia must be shielded, accommodated, and made to fit into a certain frame. 72 For example, residents living with advanced dementia are frequently perceived as being in danger of falling and hurting themselves, so therefore they are constantly told or nudged to sit down and avoid moving around at all. 73 Also, our findings display caregivers’ tendency to interpret behaviour and expressions as problematic and disturbing signs of the medical cognitive condition, which consequently means that other explanations related to social interactions or the environment may be ignored. 74 This phenomenon, known as ‘malignant positioning’, 1 has been displayed in several studies where what might otherwise be normal behaviour is considered and labelled as worrying, dangerous, or violent if the person performing it has dementia.75,76
Although our findings denote dehumanising attitudes among formal caregivers, it also became apparent that such perception never acquires the form of a clear and explicit denial of the care recipients’ humanity. The caregivers’ attitudes did not manifest as deliberate expressions of negative perceptions towards individuals living with dementia. Nevertheless, our findings revealed an inadvertent tendency among caregivers to perceive them as diminished in existential humanity. This ambiguity, where on one hand humanity is not strictly denied, but on the other existential human properties are not strictly acknowledged, resonates with dehumanising theory, that points out that in dehumanising processes the dehumaniser sees the dehumanised as both human and less than human at the same time. 25 Furthermore, when encountering other members of our species, our senses react directly, and we automatically experience them as humans. However, dehumanising attitudes are not merely passive sensory interpretations of the other but an active process formed by dehumanisation ideologies that make us accept beliefs in defiance of what our senses tell us. 25 This resonates with well-established research literature going back over 60 years which demonstrates how such ambivalent experience of others is affected by seeing what we expect to see. An example is Rosenhan’s 77 classic study ‘On Being Sane in Insane Places’ that shows how utterly normal actions exhibited by mentally healthy people could be interpreted as being abnormal by professionals in a psychiatric hospital – because the professionals expected to see abnormality in people in that context and did not differentiate mentally healthy individuals from those who were mentally ill. This exemplifies how our perception of the other is based upon expectation, training, context, motivation, culture, memory, and the like. Thus, if we see a person otherwise familiar to us in a context in which we don’t expect to see them we often fail to recognise that person immediately. So, when caregivers inadvertently accept all or part of a dehumanising dementia ideology, their perception is misled into paying attention to, thinking about, and imputing meaning to people living with advanced dementia in this ambivalent manner.
Thus, our analysis indicates that dehumanisation, though influenced by ideology, seldom arises as the product of purely rational thinking. Instead, it appears to be fostered by perceptions closely linked to bodily sensations and feelings. These findings align with more recent theory of moral psychology that discusses ‘embodied moral judgments’, which illustrates how our moral judgments often stem from ‘gut feelings’ demonstrating, for example, how disgust influences the severity of judgment.
78
Applied to our findings, repugnance and other ‘gut feelings’ (as illustrated by the themes described above) may lead to a negative moral judgment, depriving care recipients living with advanced dementia a sense of feeling as human beings. It is important that we acknowledge and pay attention to formal caregivers’ own embodiment as essential when providing care.
79
In recognising bodily sensations and feelings that can lead to dehumanisation, we propose a model that illustrates (see Figure 2) how dehumanising attitudes in caring relations can be categorised as the caregiver’s misled embodied perception. Thus, the caregiver senses and feels the absurd behaviour, the shadow narrative, the perilous presence, the void life, or the physical repugnance of people living with advanced dementia. Dehumanisation-embodied model, which illustrates how misled embodied perceptions can elicit dehumanisation in caring relations.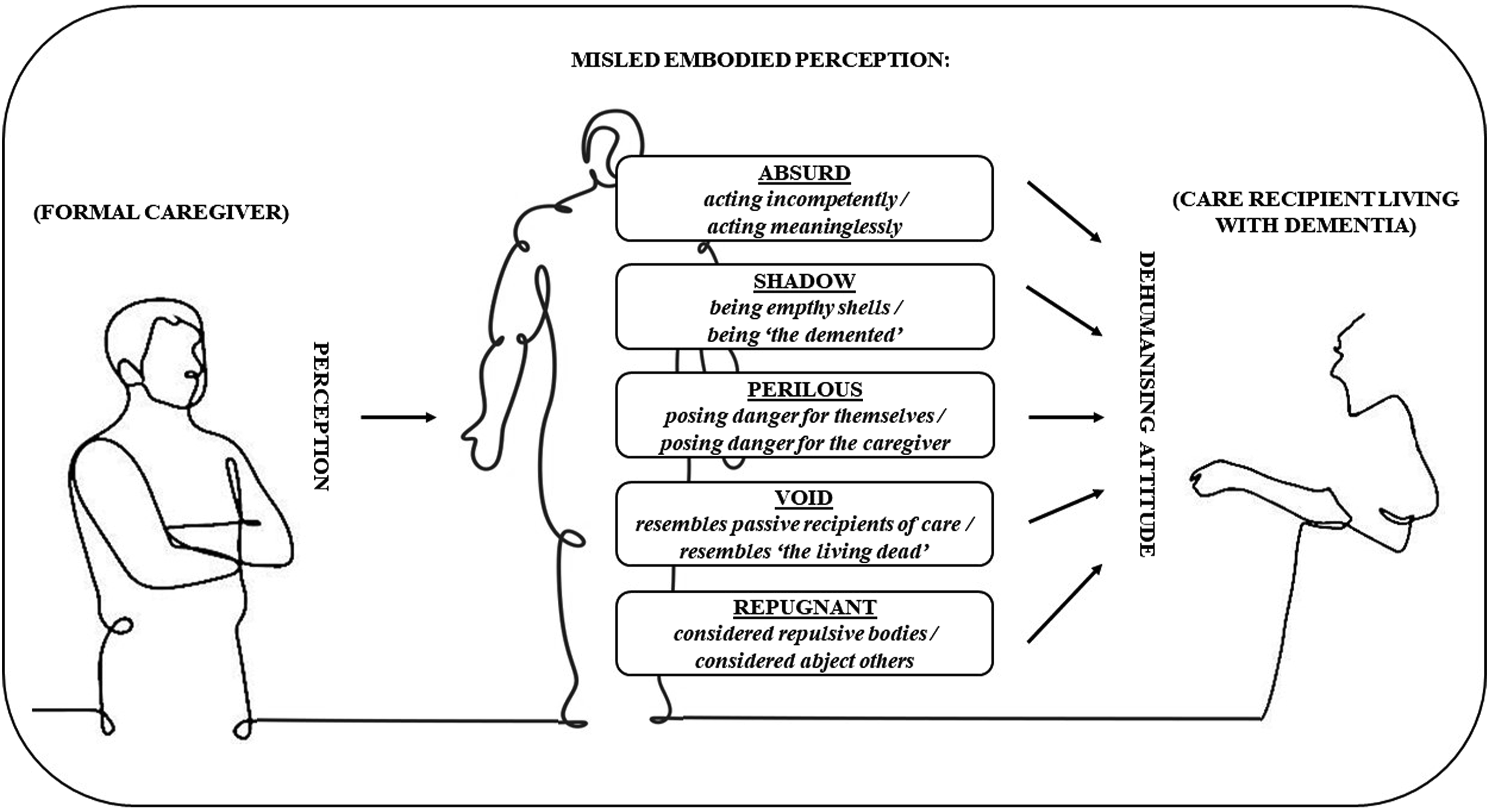
The ethical response to recognising dehumanisation should not be limited merely to an abstract discussion of where to draw moral lines, as those who do not recognise the full humanity of people living with dementia may easily believe that those lines are always met. Dehumanisation may not alter abstract ethical reflection, but it certainly influences the judgment in concrete individual caring situations, known in Aristotelian terms as ‘Phronesis’. 80 The concept of ‘Phronesis’ belongs to a virtue ethics approach, which can provide an alternative to counter dehumanisation, as virtues are the dispositions that allow us not only to do the right thing but also to feel the right thing. 4 Yet, to become more fully virtuous require that we think critically for ourselves about our inner dispositions, instilled in us by our character, training, and background. And virtue ethics can guide such reflexivity and try to improve our understanding in a way that leads us to think and act in more virtuous ways, especially in caring for people living with dementia. 4 So, learning virtues that might help to control the bodily sensation and feeling (like those described in our themes) leading to dehumanisation of people living with advanced dementia, influence also ethical thinking and evaluation of concrete cases. To support such ethical reflections in caring relations, Galvin 80 writes about ‘knowledge for the heart’. This is a kind of knowledge that cannot be reduced to rational content, nor can be reduced to an irrational feeling, but is a form of knowledge that is aesthetically textured and sensitive to unique situations lived by humans, where rationality and sensibility integrate. Thus, leading the caregiver to apprehend and respond to the ruptures in the lived experience of the care recipient. 80 Such knowledge can facilitate the addition of empathy to caring practices and is vital for guiding person-centred care23,79 and, we argue, is crucial in supporting formal caregivers’ virtue ethics to guide them to challenge their misled embodied perceptions with which they come to dehumanise people living with advanced dementia. However, though dehumanisation could be challenged by the development of virtues, this should not be read as if we claim that dehumanisation demonstrates lack of virtues in formal caregivers. The causes of dehumanising perspectives can be multiple and complex, including organisational, societal, and cultural factors, so by all means it is important to restrain from assuming moral failure in caregivers where dehumanisation is recognised.
To embed formal caregivers’ knowledge into their hearts and into their everyday practice requires them to display an empathic understanding of the world of the care recipient.79,80 As such, when recognising their own unintentional dehumanising attitudes, the caregiver should try to envision, feel, and share the world of the person living with advanced dementia and be open to what could make this person act or express themselves as any person would do. For example, if care recipients attempt to leave the care institution and ‘wander’ around apparently without an aim, this can easily be seen as an irrational and emotionless act of somebody lost in the shadow of dementia. Such a perception can easily lead to dehumanisation, possibly eliciting impatience, anger, and rushing to use different levels of constraint. Knowledge of the heart aims for a more empathic understanding, raising questions to find out in which existential experience this apparently aimless wandering is actually a meaningful human action. So rather than viewing the care recipient as an ‘empty shell’ trying to escape, it is possible to see in such behaviour a most human reaction, indeed, what might be expected from any person who finds themself in an unfamiliar place. The combination of humane empathic understanding in accordance with a virtue ethics approach allows the caregiver not only to review their misled embodied perceptions but also enables them to resist it.
Although our five themes do not directly develop virtue ethics in formal caregivers, they allow a first step in recognising dehumanising attitudes in dementia care practices that can lead to more empathic understandings. Galvin and Todres 23 created their care theory as a means to guide and improve existing person-centred care practices, by putting more emphasis on the philosophical dimensions of care recipients’ personhood. Further, they aimed at approaching personhood by considering how care recipients themselves feel as existential human beings. Thus, our results support a more existential understanding of people living with advanced dementia, that foregrounds their personhood and, thereby, can generate a more human-sensitive person-centred care. 23
Limitations of the review
As with any broad-based review, we cannot exclude having overlooked relevant literature. We have largely excluded books and book chapters as they are not explicitly commended in integrative review methodology,38,42 but we have included material from grey literature. Also, by only concentrating on more recent English language literature, we may have overlooked relevant older or non-English sources.
A further limitation concerns the term ‘advanced dementia’. As mentioned in our methods section, this term had to be omitted from the search. What we found was that even though the included articles focused on advanced dementia, many did not distinctly mention this, usually just specifying ‘dementia’. This may have affected our results and their relevance for the advanced dementia stage specifically, as the five themes could be applicable to other stages of dementia. However, it was clear to us throughout the analysis process that dehumanising attitudes became more pronounced in line with the severity of care recipients’ cognitive impairments.
In concentrating on dehumanisation, we may appear to be critical of certain professional groups and delineate an overly one-sided picture of their perception of people living with dementia. This is certainly not our intention. Dehumanisation may arise in anyone, may intermittently be turned on and off at different times, and may be seen as moving on a spectrum that puts less or more emphasis on the intensity of the dehumanising perception.22,23 This level of alternation and intensity of the dehumanisation has not been made clear in our themes. In addition, although our study found perceptions among formal caregivers that may prevent their care recipients from feeling like existential human beings, they may also in some situations effectively support their very human existence. Furthermore, our analysis is mainly at the level of the individual caregiver, whereas what may also be significant are the overall organisation, culture, and environment of residential and hospital dementia care. Thus, our paper has not explored the effects of management practices, funding decisions, or health strategies even though they likely contribute to dehumanisation of people living with dementia. These factors may limit the applicability of our results to improving dementia caring practices.
Conclusion
Our study indicates that resisting dehumanisation is not just a matter of rejecting a particular oppressive ideology but is more a practical matter of identifying and reacting in a timely way to perceptions of people living with advanced dementia that may elicit dehumanising attitudes. More than raising moral accusations we consider this paper can help the formal caregiver to recognise these misled embodied perceptions, described in our themes (absurd, shadow, perilous, void, and repugnant), and work with them through virtue ethics. In short, the dehumanising perceptions should not be taken as proof of a dehumanising ideology but rather taken as warnings of impending dehumanising attitudes that tell caregivers to review both how they are thinking and how they are perceiving the person living with advanced dementia. We suggest that our embodied model of dehumanisation offers a potential means of helping caregivers to recognise unintentional dehumanising attitudes in themselves to become able to resist them and, thereby, guide a more ethical human-sensitive care.
Dehumanising attitudes are based on an assumption that people living with dementia react as they do because they are less than humans, but this is in our opinion wrong, as people living with dementia react as they do precisely because they are humans. We should give the benefit of the doubt to people living with the condition, no matter the stage, and assume that their behaviours are the results of perfectly human and rational nature. People living with advanced dementia react just as people without dementia would do if they experienced the world from their point of view.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Independent Research Fund Denmark (2061-00010B).