
Abstract
Background
Nurses’ demonstration of compassion is an ethical and often regulatory expectation. While research has been conducted to examine the barriers and facilitators of compassion in nurses, little is known about how nurses develop and express compassion for patients who may be blamed for their health condition. Unvaccinated COVID-19 patients are an example of such patients.
Research questions
How do nurses provide compassionate care for unvaccinated adults infected with COVID-19? How did the context of COVID-19 vaccination in Canada shape nurses’ relationships with unvaccinated patients?
Research design
A generic qualitative approach using interviews to gather data was used. Martha Nussbaum’s conceptualization of compassion and its cognitive requirements was employed to add depth to the analysis.
Participants and research context
Seventeen Registered Nurses, from a range of practice settings, who had cared for unvaccinated patients with COVID-19 participated.
Ethical considerations
Ethics approval was received, and signed informed consent was obtained. Participants who were the current students of the researchers were excluded.
Findings
Three themes were identified:
1) Encountering Extreme Workplace Impediments to Compassion.
2) Managing Emotions to Provide “Nonjudgmental Care.”
3) Practicing Narrative Imagination.
Discussion
The difficult working conditions during the pandemic impeded nurses’ capacity to be compassionate. Yet, none judged their patients’ suffering as trivial, and all provided necessary nursing care. Some initially blamed these patients for the severity of their illness and suppressed their emotions to provide what they called “nonjudgmental care.” Upon reflection, participants recognized that these patients’ life circumstances may have been barriers to vaccination which, in the end, facilitated the development of compassion.
Conclusion
This research has implications that go beyond that of caring for patients with COVID-19. The ideal of “nonjudgmental care” requires critical re-examination because judgments and emotions are required for compassion.
Introduction
Understanding the development and expression of compassion is central to ethical nursing practice internationally. 1 While there have been many studies exploring compassion, including two recent scoping reviews,2,3 which have outlined the barriers and enablers of compassion, there are few studies that examine how compassion can ebb and flow in the context of challenging clinical situations, 4 including those in which a patient may be considered responsible for their health condition. When patients are perceived to be responsible for their conditions, healthcare professionals often disengage, impeding compassion. 5 For example, people, such those living with AIDS, obesity, mental health, and substance use disorders,6–10 along with those who have been labelled “noncompliant” and “frequent flyers,” have been blamed for their health conditions and have been identified as presenting difficulties for healthcare professionals in terms of the provision of compassionate care. 10 In addition, patients and families who are not receptive to demonstrations of compassion also challenge healthcare professionals’ continued engagement. 10
Unvaccinated people with COVID-19 have been blamed for their own illness by the public11–13 which raises concerns regarding the capacity of nurses to develop and express compassion for them. Various commentaries have reported that health care professionals, including nurses, have expressed anger and frustration with these patients and recommend compassion and reflection to maintain ethical practice.14–16 Others have reported moral distress, 17 moral outrage, 18 and compassion fatigue 19 in health care professionals in relation to this patient population. A Belgian study examined the effect that divergent COVID-19 beliefs among healthcare workers had on their relationships with their peers and patients. 20 Healthcare workers, both vaccinated and unvaccinated, reported an erosion of trust with patients, the avoidance of conversations about vaccines, and the occasional provision of suboptimal care for unvaccinated patients. While compassion and empathy were not explicitly explored in this study, the need to address stigma and inequities for conditions that are perceived to be self-inflected was. 20
It is well known that the COVID-19 pandemic had a tremendous impact on nursing including having significant implications for nurses’ well-being, including exhaustion, 1 moral distress, and moral injury.21,22 It has also affected nurses’ capacity to fully meet their standards of care, 21,23 such as the provision of adequate end-of-life care21–23 and family centered care.21,24 Less is known, however, on the impact of the pandemic on the compassion of nurses, specifically when it concerns the provision of care for unvaccinated COVID-19 patients. There is growing evidence that structurally vulnerable groups and communities, such as racialized groups and Indigenous peoples, may be more hesitant to receive vaccines because of the mistrust of professionals and the ongoing process of colonialization.25,26 Furthermore, these groups often experience lower income and educational levels which are also associated with vaccine hesitancy 27 making understanding and promoting compassion with those who are not vaccinated an important element in reducing discrimination and inequity.
Research questions
While the expression of compassion is an ethical and often regulatory requirement in nursing, little research exists to describe how compassion is developed and maintained when nurses are caring for patients who are sometimes viewed as responsible for their health conditions, such as unvaccinated patients who become ill with COVID-19.
Our research questions were: 1) How do nurses provide compassionate care for unvaccinated adults infected with COVID-19? 2) How did the context of COVID-19 vaccination in Canada shape nurses’ relationships with unvaccinated patients?
In focusing on the process of compassionate care provision, we were especially interested in examining how challenges are encountered and potentially overcome in this patient population and others.
Theoretical framework
Through their review of healthcare research on compassion, Malenfant et al. 2 suggest that “compassion is inherently relational, consisting of acknowledging, engaging and proactively attending to another person’s suffering that stems from the innate qualities and good intentions of a fellow human being” (p. 22). Compassion is more than empathy, the capacity to resonate with the feelings of others, it also entails action to respond to another’s needs and suffering. 2 There are barriers to compassion such as educational settings that are not conducive to the development of compassion and practice environments that lack resources, time, staff, and support. 3
Because compassion can be variably defined as a virtue or a social construct, we chose to embed our work in theory, namely, the work of philosopher Martha Nussbaum,28–30 to add clarity, theoretical depth, and explanatory power to our study. We considered other perspectives as well, such as the work of Carl Rogers on compassion and unconditional positive regard in which the carer accepts the experiences of the other without judgment, 31 but chose Nussbaum’s work because it offers an understanding of the nature of multiple forms of judgment in the development of compassion.
Nussbaum has defined compassion as “a painful emotion occasioned by the awareness of another person’s undeserved misfortune”
28
(p.301). Our emotions are our value judgments that are central to compassion and without which our ethical responses are incomplete.
29
To act merely on a sense of duty is morally inadequate because moral emotion and the correct motives are required for actions to be morally virtuous.
28
Nussbaum
28
(p.321) outlines the requirements of compassion. She states: Compassion, then, has three cognitive elements: the judgment of size (a serious bad event has befallen someone); the judgment of nondesert (this person did not bring the suffering on himself or herself); and the eudaimonistic judgment (this person, or creature, is a significant element in my scheme of goals and projects, an end whose good is to be promoted).
The first cognitive requirement, the judgment of size, entails the belief that the suffering of another is serious and not trivial, that is, it must have significance in relation to their goals. 28 In this perspective, empathy is not enough because we cannot imagine another’s experience without appraising it. 28 The second requirement, the judgment of nondesert, is the determination of legitimate suffering, that is, a belief exists that the other does not deserve their suffering because it was beyond their control and not their fault, or that their suffering is out of proportion to their responsibility for creating it. 28 In doing so, we must be able to acknowledge that we are also vulnerable to misfortune. 28 The third requirement, the eudaimonistic judgment, involves viewing the suffering person as a part of one’s own “circle of concern” 28 (p.336). In other words, the other must be viewed as a significant part of one’s own goals and, therefore, their good or well-being should be promoted. 28 Generally, the development of the eudaimonistic judgment requires the “Aristotelian judgment of similar possibilities” 28 (p.321) which is characterized by the recognition that one could also be vulnerable to similar sources of suffering.
Circles of concern can be too small when people cannot identify with the suffering of others because of distinctions of class, race, gender, religion, and other social disparities. 28 In later work, Nussbaum 30 urges us to develop the capacities necessary to overcome the “bondage of habit and custom”(p.38) to be able to imagine the suffering of others. As a start, it is important to be able to be self-critical and to be critical about one’s own conventions and traditions. 30 Through education, we can come to know to understand the heterogeneity of the world with its various histories, religions, races, and genders and their influence on life opportunities. Finally, we all need to develop “narrative imagination” 30 (p.39) to imagine the lives of people who are very different from ourselves through life experience and exposure to the arts. 30
Like the studies reviewed by Malenfant et al., 2 Nussbaum 28 also recognizes that cultivating and expressing compassion requires a conducive context. She states, “The relationship between compassion and social institutions is and should be a two-way street: compassionate individuals construct institutions that embody what they imagine; and institutions, in turn, influence the development of compassion in individuals” 28 (p.405). Nussbaum 28 emphasizes that appropriate public arrangements must exist for the growth of compassion not only for those who are sick or otherwise vulnerable, but also for those who care for them.
Research design
We chose a generic qualitative approach to provide us with the flexibility needed to draw on various qualitative methodologies to best suit our research. 32 It also offered the possibility of using Nussbaum’s28–30 work as an interpretive framework to help us organize and make complex insights when analyzing our data. 33 In doing so our work is in keeping with an interpretative approach.
The authors, who are all experienced qualitative researchers, conducted semi-structured interviews of approximately 45 to 60 min in length from February to April 2022 using Microsoft Teams. Interviews were used as a method for data collection because they encouraged participants to share rich descriptions of their experiences caring for this patient group. 34 Participants were asked about their area of practice, educational background, gender identity and age; the impact of the pandemic on their work; and their experiences when caring for unvaccinated patients, including their emotions, ethical challenges, expression of compassion, and reflections on these patients’ vaccine hesitancy. They also were asked to share the reactions of their colleagues and leaders and what helped them, if anything, to provide good care. These audio-recorded interviews were transcribed by a professional transcriptionist, and after the deletion of the recordings, the deidentified transcripts were stored securely on OneDrive.
Throughout the process of our research, we engaged in an ongoing reflexive process that led us to be critical and reflective of our own subjectivity and context. 35 We discussed and documented our assumptions and methodological choices, including our choice of a conceptual framework. 35 When developing our relationships with our participants we were aware of our identities as academic nurses who were all fully vaccinated. As a way of promoting trustworthiness, we used a reflexive stance when interacting with participants, given our relative position of power, and later during data analysis when interpreting participants’ experiences and perspectives. 36
We analyzed the data using theoretical thematic analysis, which is a systematic, yet flexible, way to locate and develop an understanding of patterns, concepts, and meanings across a data set to make sense of, and richly describe, shared experiences using an identified theoretical framework, in this case the work of Nussbaum.37,38 We were particularly focused on Nussbaum’s28–30 conceptualization of narrative imagination and the three requirements for compassion, i.e., the judgment of size, the judgment of nondesert, and the eudaimonistic judgment. Six steps were followed: becoming familiarized with the data; identifying initial codes; searching, reviewing, and then naming themes; and producing a manuscript.37,38 These steps were conducted iteratively and collaboratively among all co-authors until we reached agreement regarding the names and characteristics of the themes and achieved coherence among the themes, the theory, and the research questions.
Participants and research context
Participant Demographic data (n = 17).
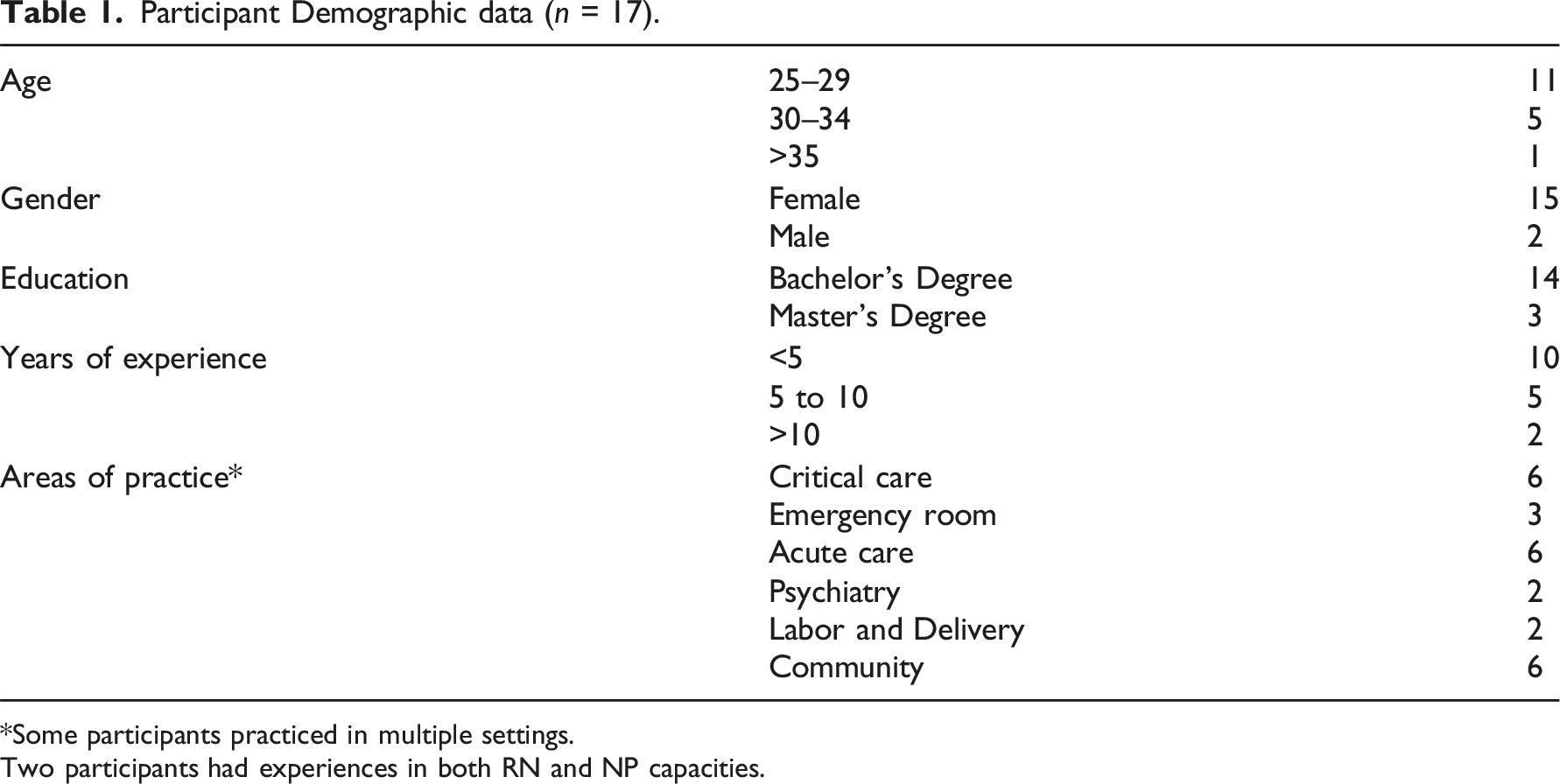
*Some participants practiced in multiple settings.
Two participants had experiences in both RN and NP capacities.
Ethical considerations
Research ethics approval was obtained by the University of Toronto’s Health Sciences Research Ethics Board. Prior to being interviewed, participants signed an informed consent document which described the nature of their participation, along with any potential risks and benefits. They were also given the opportunity to ask questions and to withdraw from the study at any time. To show our appreciation, we gave them electronic gift cards that had a monetary value less than their hourly rate as nurses to ensure that they would not feel coerced. We excluded any potential participant who was currently a student of members of the research team to avoid any student feeling pressure to participate. All data is considered confidential and is stored on a secure server.
Findings
We identified three themes that illustrate the process of nurses developing and expressing compassion for unvaccinated patients and the context in which this occurred during the pandemic: “Encountering Extreme Workplace Impediments to Compassion,” “Managing Emotions to Provide Nonjudgmental Care,” and “Practicing Narrative Imagination.”
Encountering extreme workplace impediments to compassion
The hardships that participants experienced while working during the pandemic affected their capacity to develop compassion for their patients, not only because of the frequency of death, but also because of the lack of preparedness of the healthcare system and their individual workplaces. They spoke of the shortage of nurses and beds that led to high workloads (5, 6, 7, 9, 11, 12, 13, 14, 16, 17), redeployments to unfamiliar areas of practice (1, 5, 7, 16), hostile patients and families (15, 17), tensions related to vaccination mandates for healthcare workers, (1, 7, 10, 15), and the visitor restrictions that separated patients from their family (2, 7, 9, 10, 11, 12, 13, 15, 17) as being especially difficult.
Describing their intense experience of working during the pandemic, Participant 8 said: “COVID, I think, “flipped both my workplaces upside down,” and Participant 3 said: “I just don’t necessarily feel like it’s totally natural to have, like, this much repetition of tragedy on an ongoing basis.” As a result of these working conditions, nurses and other team members were described as burned out (3, 4, 6, 7, 9, 12, 14, 15, 17), exhausted (3, 6, 7, 12), and overwhelmed (10, 16).
Most spoke of the lack of meaningful workplace supports (1, 2, 4, 11, 12, 15, 16) or had mixed reviews of the support provided (3, 5, 6, 14), revealing institutional leadership that could not, or did not, show compassion for participants’ working conditions. At the time that the interviews were conducted, many protests regarding COVID-19 restrictions were being held close to hospitals, lowering the morale of participants (2, 4, 6, 7, 8, 9, 13, 15, 17). Participant 9 said, “It’s a little bit soul crushing…Why are you protesting this when healthcare workers are trying to get to work and you know, do good things?” The protests also revealed a lack of compassion for the well-being of healthcare workers on the behalf of some members of the public. Participant 4 summarized the impact of these working conditions on compassion: “I think most people with organizations right now because, you know, you don't necessarily feel super supported when you're working in an environment that's constantly short, and you know people are talking about money and there's cuts and you know and you're just doing your best and everyone is trying to get by, but everyone is burned out… It’s dependent on a workplace and a work environment that...that has good people, and by good people I mean people that check in on each other and people who see the suffering of others. And sometimes people are so tired and burned out at this point that they don't have the energy to do that.”
It is in this context that most participants (1, 2, 3, 7, 10, 11, 12, 13, 14, 16) also spoke of the attitudes and comments of some of their coworkers, including other nurses and members of the multidisciplinary team. Participant 10 said: I feel like...maybe...like not with the patient but in, like, the attitude among the care team sometimes is rather judgmental about the patient. Not in front of the patient but...and so maybe that has impacted care, you know because when...when the whole team is kind of in, like, saturated by that culture of judgment, there are definitely difficulties that can arise.
These judgments reflect the belief that unvaccinated patients were responsible for their predicament and should not have been freely consuming valuable healthcare resources. In other words, they were judged to be responsible for their suffering and therefore, an indication that Nussbaum’s
28
second requirement for compassion, the judgment of nondesert, was not met. For example, Participant 1 said: It’s a bit disappointing because I would hear comments as if they were vaccinated, they’re not going to be here, or things like, they should pay for their own healthcare. It’s their fault that they’re here.
Similarly, referring to the perspectives of some team members, Participant 7 said: Unvaccinated people are just kind of taking up valuable resources that vaccinated people aren’t being able to receive, at the moment, because they’re considered non-acute and non-emergent.
Overall, this context of fatigue, overwork, stress, and attitudes of blame is important to acknowledge because the unusually difficult working conditions had an impact on all team members’ ability to provide compassionate care.
Managing emotions to provide “nonjudgmental care”
Participants expressed a host of emotions that they actively managed to provide nursing care in a professional manner to this group of patients. Frustration (2, 4, 7, 9, 13, 14, 17) and anger (2, 3, 6) were commonly described as emotional reactions. From the perspective of Nussbaum, 28 these emotions are value judgments that were actively suppressed by participants.
Several strategies to control frustration and anger were described, such as venting privately (2, 11,16). Participant 16 said: “The patient would still receive, you know, optimal nursing care, hourly rounds, meds, all that sort of stuff but the sentiment would definitely come out in I guess, private spaces where nurses felt free to vent.” Other strategies included suppressing both emotion and negative thinking to avoid having their emotions influence patient care. For example, Participant 14 said: “So, that's why I've kind of really focused just to take it as it is, don't ask questions, don't get upset, don't let your emotions into it. Just take care of them as a patient with COVID pneumonia.” Similarly, Participant 17 said: “It's difficult to try to...to keep going and you know, put on, I guess, a smile when you've just been kind of verbally abused about these decisions,” and Participant 12 said: “While I'm in the room, (I) just stop thinking about it.” Participant 15 was able to continue to provide care by limiting communication. They said: I personally choose not to communicate. I...I just...I say okay, I keep my communication very, very limited. I don't try to make small talk. I don't...the patients are here to get better, so I just choose to keep it very simple, very direct and that's it.
The perceived moral responsibility to provide care in a nonjudgmental fashion by disregarding these emotions for unvaccinated patients is summarized well by Participant 6 who said: You still have to take care of them, so...and provide, like, the same type of care that you to any patient and be, like, non-judgmental. So, I think that...I think it’s a bit of a battle just knowing that you still have to provide, like, good patient care regardless of their point of view that they have on vaccines and views that have on yourselves and like being unbiased and unjudgmental in terms of providing all types of care.
Treating unvaccinated COVID-19 patients dutifully and in a uniform fashion were aspects of this approach to care. This way of thinking is illustrated well by Participants 11 and 9. Participant 11 said: “You need to treat those patients the same way you treat, like, a drunk driver or like, a pedophile that we have or someone from jail. Like, you have to still do...the same thing,” and Participant 9 said: “So, I don't think that there's necessarily a different approach to care because we all kind of recognize that we have, you know, a duty to go and care for these patients.” (9)
While none of the participants expressed doubt in their patients’ suffering, i.e., they met the first requirement of compassion, the judgment of size, 28 this overall approach to care was not fully adequate to reach the ideals of compassion. Compassion entails the expression of moral emotions, 28 which is not consistent with the suppression of emotion to control frustration. Nevertheless, Nussbaum’s 28 third requirement, the eudaimonistic judgment, was met by these participants because they provided nursing care for these patients because they were deemed to be in these nurses’ circle of concern as a reflection of their nursing responsibilities and goals.
Practicing narrative imagination to foster compassion
All participants engaged in a process of narrative imagination in their responses to unvaccinated COVID-19 patients to foster their compassion, sometimes referring to the expression of compassion for patients as central to their nursing identity. Through this process they were able to respond to patients’ suffering by recognizing the barriers they may have encountered when considering or obtaining vaccinations resulting in their understanding that these patients’ COVID-19 illness was undeserved. Ultimately, the participants felt the painful emotions inherent in compassion that Nussbaum 28 describes, saying things like it was “hard and sad”(11), “sad”(5, 12), “heartbreaking”(9), and that they were “grieving for these patients.”(4)
Expressing the fundamental moral importance of compassion and the need to look beyond patient choices, Participants 1 and 9 said: So, to me, as a nurse, we should...compassion should be innate in us... I mean, we are taking care of people, and it shouldn’t matter what their choices are. That’s what we have learned...not only learned but that’s who we are as nurses. (1) At the end of the day, they're still humans regardless of, kind of, the choices that...that they've made regarding vaccine or not vaccine. They're still...you know, they're still critical care patients. They're still very sick humans in beds who are, you know, at risk of losing their lives and that's devastating and it's sad. You still need to kind of provide that compassion and care for patients who like many are at the end of their life. (9)
Participant 3 described well how they initially judged a patient but then reflected on the patient’s personal history that may have inhibited vaccination, leading to their judgment of nondesert of a patient’s suffering and the development of the participant’s compassion. For someone not to take, like, the opportunity that they have in this country to prevent themselves from a life-threatening virus, like it just...it doesn’t really add up in my mind but...but then I have to pull myself back to, like, background histories and life experiences and stuff and just have some kind of compassion for that.
Similarly, Participant 4 commented on the importance of understanding peoples’ different interpretations of information and beliefs in maintaining compassion in the following quotation: “Moral beliefs and dilemmas and science and people's own personal research on what that means and what data means and how they have interpreted it kind of preserves the compassion and the integrity of the provider.” Through these quotes Participants 3 and 4 demonstrated the compacity to not only rely on their own beliefs and knowledge to make sense of their patients’ decisions and actions, but also to rely on the importance of recognizing the heterogeneity of peoples’ perspectives that Nussbaum 30 encourages.
Participants also identified epistemic barriers to becoming vaccinated such as a lack of information or the presence of misinformation, especially that which contained elements of a conspiracy theory (5, 10, 12, 13, 14, 15, 16, 17). A lack of trust in science (3, 17), specifically in the COVID-19 vaccine which was believed to be developed too quickly and consequently, was thought to be unsafe (1, 9, 12, 13, 14, 16), was also a common explanation that participants gave regarding their patients’ reasons for not being vaccinated. Participant 13 described well how understanding these barriers helped them to become empathic. So, frustration for sure, but also empathy recognizing that there is so much misinformation out there and if you're...if you're not as literate...like, if your health literacy is not as high as, like, a healthcare provider's then you might not know where the right information to go to is. (13)
Pregnant people and those in their childbearing years were identified as groups with significant reservations given the newness of the vaccine and conflicting information (2, 5, 9, 11, 15).
Participant 5 said: So, a lot of pregnant women thought they would be...they were almost like being guinea pigs, right and then there were also things that were said in the media about, like, like how the vaccine affects fertility and so on and so forth.
Others pointed to differences in religion and culture (4, 9, 10, 15) and distrust in government given the history of discrimination that some of these patients had experienced (3, 5, 8, 10, 11) that influenced decisions about vaccination. Participant 11, in the quote below, articulated the process of developing empathy by imagining the lives of their patients that were very different than their own in a process that Nussbaum
30
believes is necessary for opening our concerns for people who may seem initially dissimilar from ourselves. I've tried to work on, like, empathy for patients who are unvaccinated…I think they (patients who immigrated from a different country) relate a lot of it to feeling like the government has too much control. I don't know if it's the actual science behind it they're questioning but they, like, I think are feeling parallels to the government in the country they used to live, and so it's very, like, triggering for them. (11)
Discussion
The significance of our research is greater than that of furthering our understanding of nurses’ compassion in relation to unvaccinated COVID-19 patients, but it is relevant to other patient populations as well. It also sheds further light on recognizing how working conditions can pose challenges for healthcare workers. As in previous research,2,3 we discovered that the context of care had a significant impact on the capacity of nurses to be compassionate, making it important to be critical of the assumption that nurses are compassionate by their nature and role. Rather than attribute individual blame to our participants for sometimes not meeting the ideals of compassion, we suggest that multiple contexts shaped their moral relationships with unvaccinated patients. Workload, the lack of support, colleagues who blamed patients, visitor restrictions, vaccination mandates, and protests all had a detrimental effect on them which compounded the challenges they experienced with a patient population that had the hallmarks of those found to challenge healthcare professionals’ compassion.6–10 Nussbaum,28,30 along with scholars in nursing, 40 have long recognized that ethical practice is deeply influenced by working conditions, including the moral environment of organizations, making it incumbent on organizational leaders, regulators, and policymakers to foster the moral conditions of nurses’ work especially in crisis circumstances that could compromise compassion and the well-being of nurses and patients alike.
Our findings, like those of other studies,2,4 suggest that compassion might not happen spontaneously but may need deliberate effort on the part of nurses and organizations, and it may ebb and flow. While Nussbaum’s 28 work does not describe the development of compassion as a phased process, her three requirements of compassion make it clear that these might not all be met at the same time. All participants met the first cognitive requirement of compassion, namely, the judgment of size. None doubted that the suffering of the patients was serious. In fact, many of them commented on their acute suffering while on ventilators and being apart from their families. The second requirement, the judgment of nondesert, 28 however, proved to be difficult to achieve. Because of the perceived availability of vaccines in Canada, being very sick with COVID-19 was often viewed by participants, at least initially, as something avoidable and in the end, the patients’ own fault. Consequently, participants reported difficulties that they, or other team members, experienced in developing compassion.
The third requirement, the eudaimonistic judgment, which entails including the suffering person in one’s circle of concern such that their suffering is acted upon, was met. 28 The situation of nurses and members or other helping professions is unique in this regard. Unlike coming upon, or having knowledge of, the suffering of people in everyday life or in the media, nurses, as a matter of their regulatory and employment requirements, must provide care to attend to the suffering of their patients. Their patients are necessarily a part of their professional circle of concern, which was a sentiment described by our participants. This is not to say that nurses’ motivations might not have other dimensions, but there is a difference from the concern they may experience for patients and the concern they, like lay people, may experience for the suffering of others that may not result in actions to help.
Nussbaum28,30 suggests developing our narrative imagination to broaden our perspective of peoples’ suffering beyond our usual family and friends to overcome the smallness of our everyday circles of concern and enlarge our eudaimonistic judgments. Our findings are novel because participants did not use their narrative imagination in this way, but instead used it to meet the second requirement of compassion, the judgment of nondesert. 28 They were able to move beyond their initial belief that unvaccinated patients were responsible for getting sick by coming to identify the multiple barriers these patients may have faced in becoming vaccinated. This reflexive process enabled the participants to recognize their own privilege and relative position, including their high health literacy.
This form of narrative imagination aligns well with the skills required for culturally safe nursing practice which may help nurses to go beyond assigning personal blame not only to patients who are not vaccinated, but also to those living with the stigma associated with substance use disorders, obesity, unhoused status, and mental illness to name a few. The adoption of a cultural safety approach requires that healthcare professionals be able to reflect critically on their deeply held attitudes, to be flexible in their interactions with others, and to examine how the social histories of people impact their health. 8 Compassion can then become possible, despite difference, when nurses are able to identify with the suffering of those they may have initially deemed as deserving their own misfortune.28,30
Participants’ provision of “nonjudgmental” care as a method to overcoming negative reactions to patients, however, has limitations that need attention. This approach suppresses the opportunity for nurses to reflect on their emotions and to acknowledge that some judgments are necessary elements of compassion, namely, nurses’ judgments of size, nondesert, and eudaimonism, that result in their active provision of care. Nevertheless, we are understanding of participants’ behavior in this regard because it could be an indication of depersonalization, a characteristic of burnout, experienced by many nurses during the pandemic. 41 It could be that participants were performing compassion without experiencing the needed emotions to manage the demands of care during this crisis because they no longer had the capacity to form emotionally involved relationships with their patients while also sometimes struggling with their belief that their patients’ suffering was their own fault.
Describing one’s relationships with patients as “nonjudgmental” may also reflect the ambiguousness of the term despite its commonness in nursing. 42 Nurses may be referring to unconditional positive regard in which the other is accepted and respected without judgment, but from Nussbaum’s and Rogers’ perspectives the carer also must experience emotions like warmth and even love. 31 If we subscribe to Nussbaum’s 28 conception of compassion, being nonjudgmental in the manner that participants described it, lacked moral emotion and was a sign that they were only acting out of a sense of duty. We, therefore, suggest that care be taken when the term ‘nonjudgmental’ is being used as an ethical expectation for nurses. It may seem to suggest to some that it is important to detach from patients emotionally to suspend judgment, but judgment, at least from Nussbaum’s28,29 perspective, is necessary for the development of compassion. Ultimately, we believe that emotional engagement and respect informed by narrative imagination are what is needed in nurse-patient relationships, not detachment.
Limitations
There are two limitations in our study. First, participants may have presented themselves in a socially desirable way downplaying their own struggles with compassion and instead, focused on the less-than-ideal behavior of other team members. Second, given the strong public health messaging in Canada of the importance of COVID vaccinations, nurses who were ambivalent about, or opposed to, vaccines may not have felt comfortable enough to become participants in this research, making our participants a unique sample and limiting the transferability of our findings.
Implications and conclusions
The implications of our research extend beyond the care of COVID-19 patients to the development and expression of compassion more generally. While there is ongoing debate whether compassion can be taught or fostered, 2 the use of narrative imagination that participants described is worthy of further investigation, especially because there is some evidence that reflective learning can be helpful. 3 We found Nussbaum’s28–30 work particularly helpful in offering an explanatory framework as to the various conditions and requirements of compassion and believe that further research using this framework under more usual circumstances could increase the understanding of the development of nurses’ compassion.
We recommend that the term ‘nonjudgmental’ be used with caution in relation in nursing education and codes of ethics. Although the intent of requiring nurses to be nonjudgmental may be to direct them to avoid discriminatory judgments, and not judgments more generally, we believe that nurses need to be aware of their judgments to the largest extent possible, recognizing that many of these judgments can remain unconscious 43 and need examination because they can be “parochial and habitual.”30(p.39) Being “nonjudgmental” could mask detachment, burnout, or the suppression of emotions related to blaming patients for their health problems. Given the current attention now being paid to equity, diversity, and inclusion, this is of particular concern because “nonjudgmental” care could also have the potential to hide discrimination. Nurses’ judgments could instead become normalized if they are reflexively examined with respect to how they foster or impede compassion.
Ultimately, we emphasize that compassion also be shown for nurses who often work in very difficult conditions. We can only legitimately require nurses to be compassionate if the context of their work makes this possible.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Toronto COVID-19 Action Initiative.
Correction (August 2024):
Article updated to correct the Caroline Variath's affiliation to “Vancouver Island University,