
Abstract
Introduction
Nurses working in nursing homes took care of and protected the most vulnerable group of people during the COVID-19 pandemic; frail and multimorbid old adults in need of care. Challenges occurred in the intersection between needs of the individual NH residents, protection of the other residents, the requirements of the next of kin and the needs of the society. In this study we investigated ethical difficult situations occurring in nursing homes during the COVID-19 pandemic as expressed by nurses.
Background
Older adults are particularly vulnerable to negative health effects from COVID-19 infection, 1 and older and frail adults with multimorbidity are at high risk of disease severity and death.2,3 The COVID-19 pandemic has therefore been especially challenging for older adults and those caring for them, and restrictive measures have been particularly extensive in nursing homes (NHs).4,5 Nurses have had to contend with shifting national and local guidelines concerning the handling of outbreaks of COVID-19 in their NH departments. 4 This has been complicated by the fact that residents often have complex care needs, have dementia or other forms of cognitive impairment, 6 display challenging behavior, 7 and depend on assistance in daily activities and care. Indeed, NHs are now providing care for residents who require more intensive care and resources than residents a decade ago. 8
During the first year of the pandemic, approximately 50% of all COVID-19–related deaths in Norway took place in NHs. One out of three residents with COVID-19 died because of the disease. 4 An international report on COVID-19–related deaths in NHs in 29 countries showed great variation in this respect, from 0 cases (Hong Kong, Jordan, and Malta) to 85% of cases (Canada). The percentage of NH residents who died because of COVID-19 is related to the percentage of older adults in a country living in NHs 5 ; on average, however, 47% of the COVID-19 deaths across the 29 countries took place in NHs. 9
Cooperation between the nursing staff and the residents’ relatives is a central criterion for good care 10 and quality of life for residents. 11 Visits from relatives are also very important for the residents’ overall health. 12 In the early phase of COVID-19, the Norwegian NHs were closed to visitors. While most NHs began allowing visits, these were limited and regulated. 13 These social restrictions have been challenging and caused suffering for the residents, their relatives, and the care staff; in many cases, the social distancing has been devastating, with a profound sense of loneliness for residents and guilt for their relatives and care staff.14,15,16 The lack of nurses’ everyday cooperation with the relatives has therefore been challenging in giving proper nursing care of the residents.
Registered nurses are obligated to perform nursing in a professionally safe and sound manner. The clinical nursing practice standards include (a) regulatory requirements, such as current legislation, guidelines, regulations, and human rights; (b) evidence-based knowledge and nursing skills; and (c) ethics described in the Code of Ethics for Nurses.17,18 The four fundamental responsibilities in nursing are to promote health, to prevent illness, to restore health, and to alleviate suffering. 19 The responsibility to meet the standards of clinical nursing is a shared responsibility between the individual nurse and the system within which nursing is being performed. 20 For Norwegian NHs, this latter (i.e., the system perspective) comprises different management levels in the municipality. The ways in which these managements levels cooperate within the NH and with NH staff have an important impact on quality of care for residents, particularly around creating a culture of safety, care of respect, dignity, and quality.21,22 Ethical challenges and dilemmas are common in the everyday work of nurses in NHs, as they balance between ideals, autonomy, and dignity in daily care for residents.22, 23
The COVID-19 restrictions have had an impact on daily life at NHs. 23 Sarabia-Cobo et al. 24 interviewed nurses via video conference in four countries (Spain, Italy, Peru, and Mexico), and found that they experienced fear related to the pandemic, a sense of duty and professional commitment, and emotional exhaustion. The authors urged reflection on a global level to consider the most appropriate model of care during a pandemic in NHs . 24 A Norwegian report 5 based on qualitative case studies, focus groups, and individual interviews from five different NHs stated that the COVID-19 pandemic was experienced as dramatic and demanding by healthcare personnel, residents, and relatives; the authors described ethical challenges related to the pandemic, such as balancing different residents’ and relatives’ needs, prioritizing saving lives versus living meaningful lives, isolation without decision to use coercive measures and lack of advanced care planning.
In general, however, few studies have investigated the specific ethical challenges and dilemmas in NHs during the pandemic.
Aim
The aim of this study was to illuminate ethical difficult situations experienced by nurses working in Norwegian NHs during the COVID-19 pandemic.
Research methods
Research design and participants
The study was grounded in a qualitative, descriptive, and cross-sectional design. Semi-structured individual interviews with open-ended questions were conducted with a purposeful sample of 1 male and 14 female nurses, aged between 27 and 60 years, who had experience with residents that had COVID-19. Inclusion criterion was experience with COVID-19. The nurses worked in eight different NHs, comprising 11 wards of different sizes. The experience of residents with COVID-19 was from 1 to 10 residents. Four of the NHs had no deaths due to COVID-19, while the other four had one to 3 deaths. The participants were recruited by NH leaders through the snowball method. 25 To ensure representation from a variety of communities, recruitment took place in three out of 4 health regions in Norway within both urban and rural areas.
Data collection
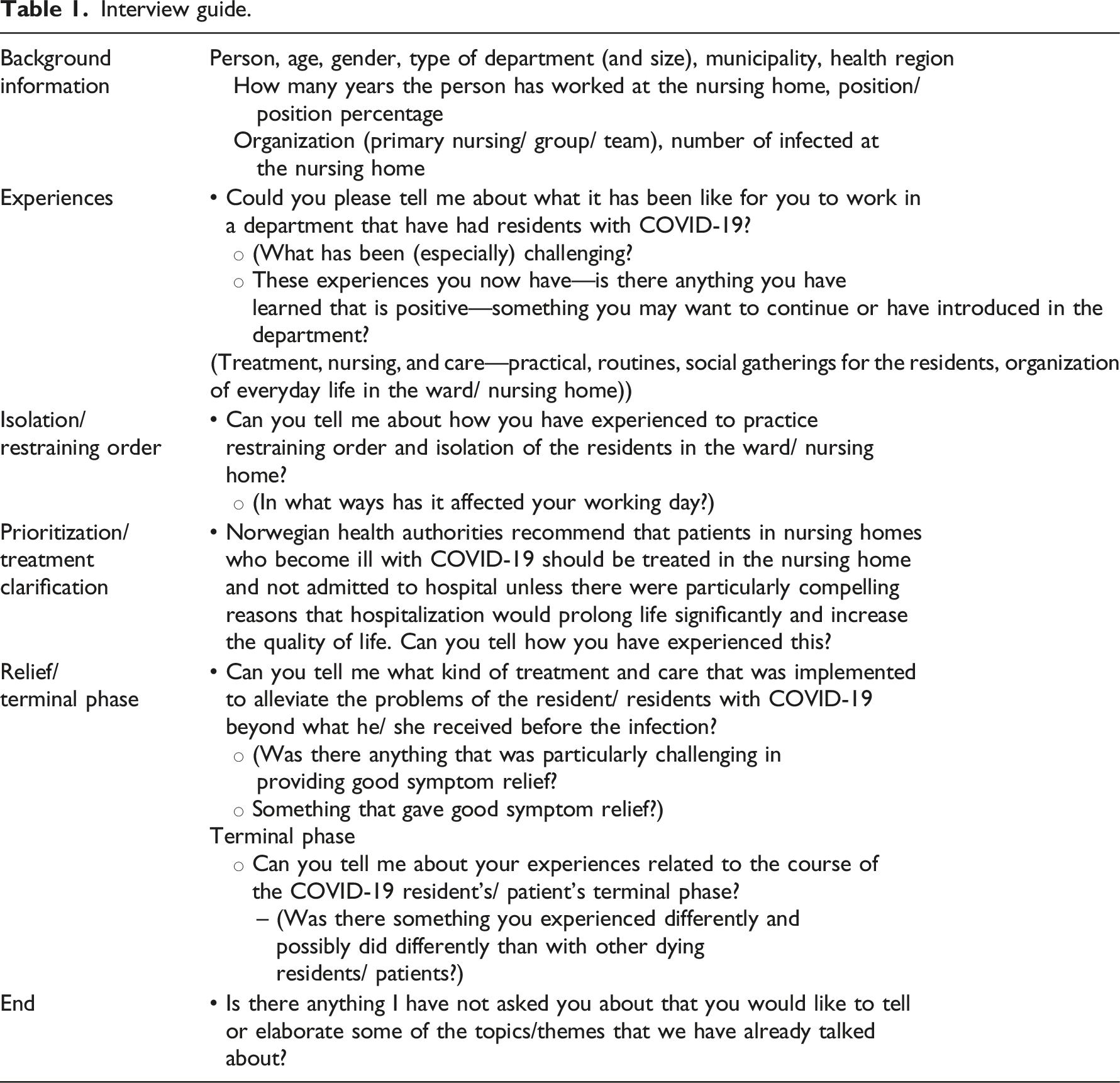
Interview guide.
Analysis
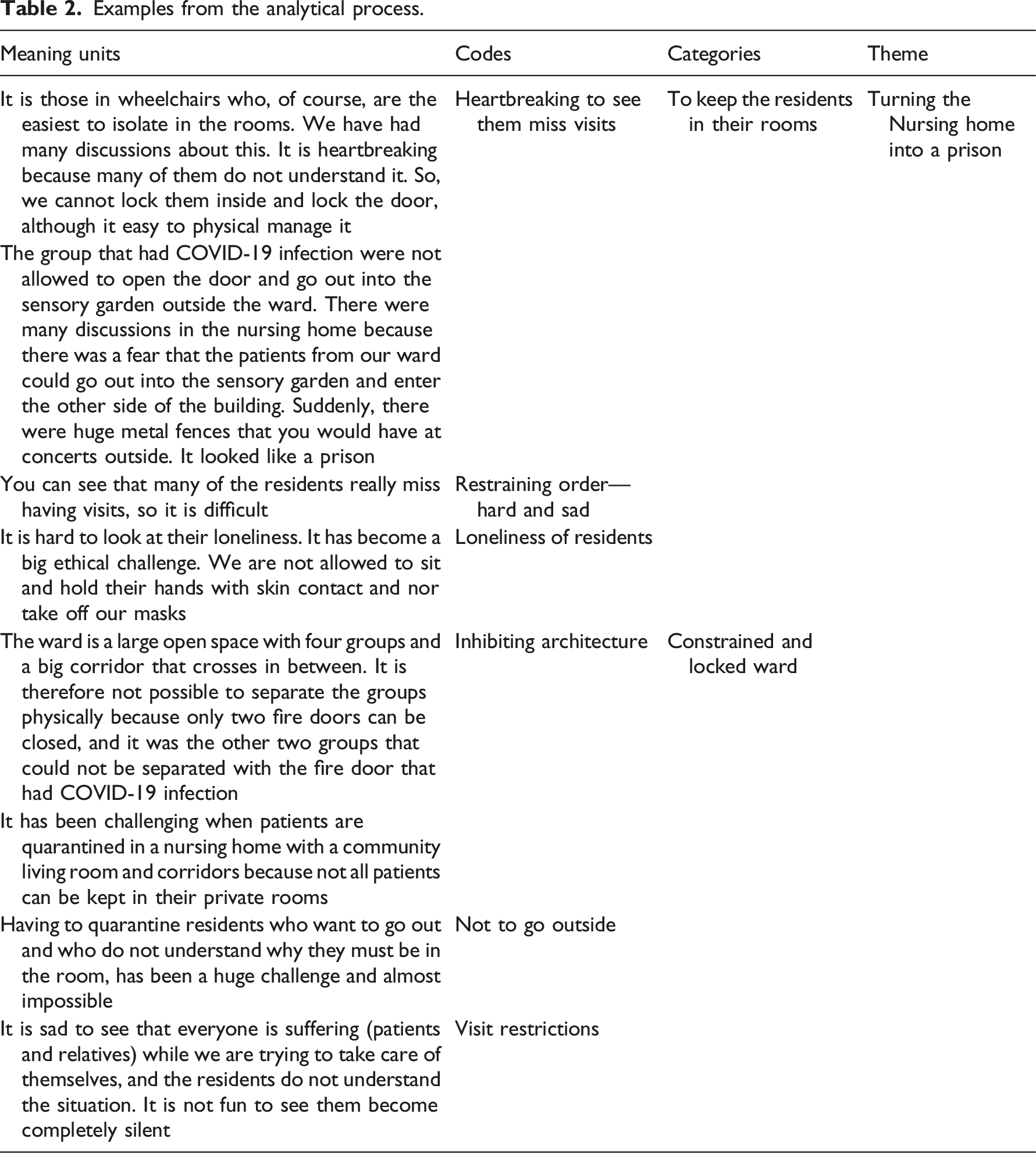
Examples from the analytical process.
Ethical considerations and approval
The study was approved by the Norwegian Centre for Research Data (NSD) (project number 503268). Oral and written information about the study was provided to acquire informed, written consent from the participants. The transcribed interviews were de-identified. The participants were encouraged not to give information/names in the interviews that could identify residents, colleagues, and NHs.
Findings
The COVID-19 context
The analysis revealed a diversity of nurses’ experiences describing COVID-19 infection outcomes among NH residents, courses of actions around preventing further contagion, and challenges in providing proper care and treatment to all residents. Their experience is also connected to the pandemic’s timeframe. Early in the pandemic, in March/April 2020, there was considerable uncertainty regarding restrictions, quarantine regulations, proper infection-control equipment, and the organization of isolation, which made the nurses’ work quite challenging. Moreover, as the rules and regulations changed rapidly, many of the nurses reported that they coordinated with their colleagues to check the government and health authorities' websites for updates. The nurses had to determine how to isolate infected residents, implement quarantine restrictions, and organize cohorts—all while contending with concerns regarding a lack of infection-control equipment. All of the nurses described a fear of being infected themselves during this time, either bringing COVID-19 into the NH or from the NH to their families. Correspondingly, most of the nurses implemented very strict hygiene measures and some isolated themselves from their family.
Overview of findings: Codes, categories and themes.
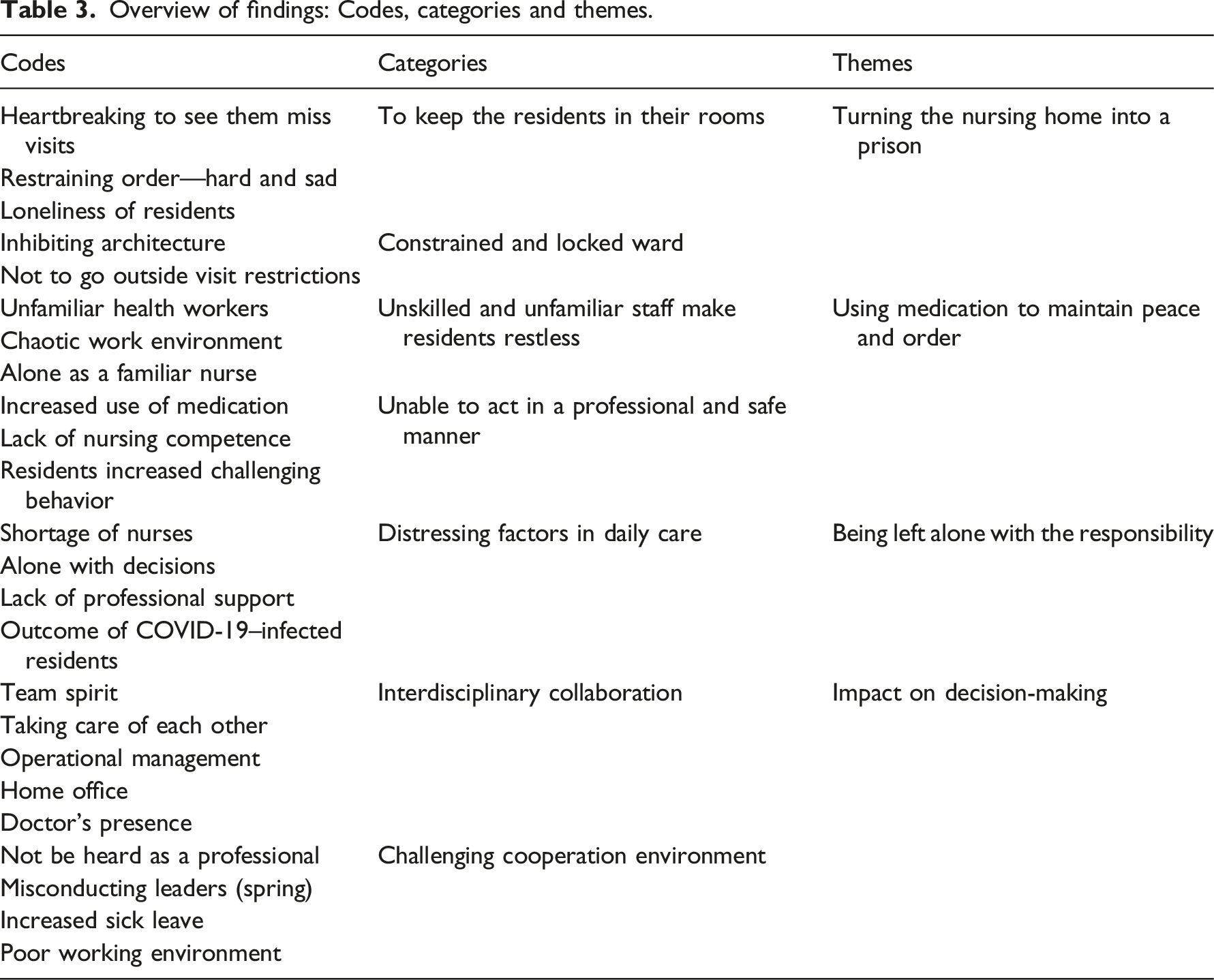
Four key ethical dilemmas were identified from the nurses’ experiences and will be presented below: (a) turning the nursing home into a prison; (b) using medication to maintain peace and order; (c) being left alone with the responsibility; and (d) impact on decision-making.
Turning the nursing home into a prison
The nurses expressed tremendous distress about having to tell the residents that they had to stay in their rooms, and that they were not allowed to come out before they were given permission. All the nurses explained that they felt they had turned the ward into a prison with locked doors and barriers to prevent residents from walking around and sitting in the communal living spaces. Some also referenced the fences that were erected to prevent residents from going into the garden.
There are two adjoining buildings. And so, there is also a door in there. So, they were very afraid that patients from our ward would walk over and into the building on the other side. So, once this spring, suddenly an enormous metal fence was put up (…). It really looked terrible, looked like a prison. (N12)
All the nurses reported that many of the residents with cognitive impairment had difficulty handling these restrictions. Many nurses explained that they had to create restricted areas so that mobile but cognitively impaired residents would be constrained to one small part of the ward: the nurses said that they could not prevent them from coming out of their rooms because these residents did not understand what was happening. To make them stay in their room, the nurses had to lock the door with a key, and that felt too harsh. One nurse reflected that this practice may have caused more contamination in the ward, but they chose this solution to mitigate distress for both residents and the nursing staff.
It is not possible to keep all patients in their room—not everyone lets you explain that they must remain in the room. There are many reasons for them being there, so there have been some challenges. Because in the beginning we saw that the first who were infected were quite mobile in the ward. (…) So, if we had managed it a little better, then maybe we could have confined it more—we don’t know this, but it all happened so fast. (N15)
Using medication to maintain peace and order
Many nurses related that they thought that it would be very stressful and frightening for residents to be locked in their rooms without understanding why. Few wards therefore used medications to ensure that the mobile residents suffering from dementia would stay in bed, calm and drowsy, with one nurse sitting at their bedside to look after them and help them with food and beverages.
We had a professional and ethical discussion about it (…). If it had been me being confused and old, maybe … I would rather be drugged unknowingly, just lying there drowsy, taking in food and then sleeping again, rather than not understanding it. Just being relaxed and comfortable, rather than confused and thinking that I had to go out, looking for my kids, my father, my mother (…) and then not being allowed to get out. I imagine I would have fought tooth and nail to get out of that door, and that is much more undignified, in my mind. (N2)
Many nurses reported an overall increase in the use of medication to maintain peace and order in the NHs during the pandemic. Many residents became more physically and verbally agitated and upset in these new situations, which often involved the recently hired unskilled staff. In some instances, the residents hit staff, leading to significantly increased use of medications. Reflecting on this, the nurses felt that they had not acted in a professionally sound and safe manner in these situations.
They [the residents] noticed that they were unfamiliar people [staff] who did not know them—because we know exactly what we should say to the patients. They need things to be quite similar every day. We know what to say to calm them down, meet them where they are. And when unfamiliar people come, they do not know the routines. So, what we saw… a lot of extra medicine was needed to keep them [the residents] calm. Quite simply in order to avoid fights—they can harm themselves and others. We do have aggressive patients. (N8)
Being left alone with the responsibility
Any nurses who had been at work when a resident tested positive for COVID-19 had to go into quarantine. This led to limited staff availability. Some thus experienced being the only nurse on staff who knew the residents, had the skills to undertake the hygiene measures, and knew the organization of and routines in the ward. These nurses expressed how they were overwhelmed by the responsibility and felt that they were unable to practice soundly and safely. One nurse described a situation that still haunted her, when she explained the challenge regarding the distribution of skilled and unskilled personnel early in the pandemic. All the skilled personnel were working with the two residents who had COVID-19, and she was left alone with 24 residents and newly hired and untrained staff members.
I was left alone, knowing the names of 24 patients, who they were. It was a dementia ward where no one can account for themselves. (…) When [staff] from other wards came—and among them a group from the social and welfare services who had never been to a nursing home before—in the heat of the battle, I found masking tape and wrote the patients’ names and stuck it onto their backs so that those who came in would know which room they should return them to or [help them] stick to their food lists (diet lists) and such, for example (…) Oh, it was an extremely painful situation to be in (…) I found an abandoned patient with a mouth filled with meatballs, with an obstructed airway. Recovered a patient in the cooling room who was drinking a bottle of chlorine. No, it was terrible! (N12)
All nurses experienced a feeling of being left alone with the responsibility for the daily treatment of and care for the residents. They described how being the only nurse in a shift who could care for a sick resident with COVID-19 was sometimes so stressful that they felt powerless.
I was in that room (…) with the responsibility for her in all of my shifts because I was the only nurse … and she was quite ill. I was going to try to insert a peripheral venous catheter—it was so difficult, because she was so dehydrated, with arteries that cracked. I remember that I started to cry in that patient’s room, because (…) she was so ill and I was not able to help her and there was no one else to ask to help me. Actually I don’t remember how things went, if I was able to insert the catheter or not. I only remember a … feeling of powerlessness, and that I actually started to cry.
In some NHs, it was decided that leaders and physicians could not enter the ward, and this made the nurses’ work more challenging. One nurse talked about a situation in which a resident had died and the physician could not come into the ward to confirm the death. Instead, the nurse was instructed to use FaceTime to facilitate the physician’s confirmation. She described this as feeling too absurd, so she refused.
[It was] an ordinary, expected death, and the leaders in the municipality had refused the physician to enter the room to confirm that the person was dead. So, we received the message that this should be done on FaceTime. All the ethics just ripped apart inwardly. You cannot go down to the morgue and take your telephone along and do it on FaceTime! It was completely absurd, and I just didn’t understand. So, I put my foot down and said “That, I will actually not do.” No. (N7)
Not having control and being alone in assessing medical treatments and making judgments about infection-control measures were highlighted by most of the nurses as challenges early in the pandemic.
Impact on decision-making
When the second wave of COVID-19 reached the NHs, nursing students and capable volunteer personnel from the first wave were more readily available. Several nurses stated that they could not have survived without these individuals. When they spoke about their experiences with the NH leaders and community leadership, however, the nurses’ accounts were a bit more nuanced; these experiences were largely influenced by how the municipality and NH leadership acted in regard to the pandemic situation and cooperated with the nurses. Some leaders were supportive and helped to make the best of an exhausting situation, through obtaining necessary equipment; organizing and implementing new routines for kitchen and cleaning personnel; hiring more nursing staff; making phone calls to the residents’ relatives; and having daily dialogues with the nursing staff. The nurses reported that some of the NH leaders refused to work from home, arguing that they wanted to remain in the ward to provide moral support for their staff. Two NHs also had a physician working in the ward, helping with sick residents, educating unskilled staff, and organizing routines for infection control. All of the nurses in these NHs felt that there was good cooperation between the leaders and the rest of the NH staff. Indeed, the nurses expressed that despite this extreme period and the ethically challenging situations, they felt they had developed better partnership between and among the other nurses, other personnel in the interdisciplinary care team, and the NH leaders.
In other NHs, the nurses expressed their frustration over leaders’ lack of involvement, support, recognition of their nursing skills, and understanding regarding the challenging situations the residents and the nursing staff were facing. The nurses described some decisions as especially challenging and nearly unbearable. One such situation occurred when two nurses were instructed not to inform the other residents’ relatives when one of the patients was confirmed as having COVID-19. Only the infected residents’ relatives were to be informed, but the nurses explained that they experienced this as dishonest; moreover, they felt that this lack of honesty would ruin the cooperation they had with the relatives, as these latter would lose trust in the nurses.
In March, it was so painful, because we got the message from the management that we were not allowed to inform the relatives about infection in the ward. Almost a week went by from the established infection until we could convey the information. The family called, asked if we had contagion, and of course we were ordered to lie. That was extremely painful. (N4)
Two other nurses described a discussion with their leaders in which they expressed the opinion that the ward should not receive new, short-term residents for observation without first testing them for COVID-19, but their opinion was disregarded. These nurses also noted that placing a new resident into a sparsely furnished room in which they were forced to sit alone for days was difficult to handle, emotionally and professionally. Six nurses stated that there had been some problems with regard to cooperation with the management even before the pandemic. However, the pandemic brought with it issues related to high turnover, sick leave, and burnout, which simply added to the challenges with which the nurses were already contending. These nurses expressed the opinion that this would ultimately affect the satisfaction of both residents and their relatives with the NH.
Discussion
The COVID-19 pandemic has challenged societies and health care professionals around the world. In this study, we aimed to explore and describe the ethical difficult situations experienced by nurses working in Norwegian NH.
To establish control over the situation and fulfill the infection-control regulations, the nurses described using physical constraints such as locked doors and medications. They felt being alone with the responsibility, and many experienced that their leaders gave them orders with which they disagreed. They often felt forced to do things against their own professional judgment of proper care for individual patients. The findings are in line with other studies emphasizing that the COVID-19 pandemic threatened the integrity of clinicians and created moral stress and suffering.29,30
As in other countries, the main goal for the health management of the pandemic in Norway was to protect inhabitants from COVID-19 infection: in particular, to protect frail, vulnerable, older adults living in NHs.4,13 The regulatory requirements were developed in accordance with this goal. One could argue that the regulations and guidelines were developed to maximize utility for society as a whole—prioritizing minimizing infection over all other health-related goals on a national level. These external factors, such as national and local guidelines for infection control and clinical procedures, controlled and limited the arena in which the nurses in our study conducted their professional practice.4,13 Our findings revealed the complexity of the COVID-19 situation and describe the challenges that arose when the nurses balanced between following the guidelines regarding isolation and visiting and providing what they considered proper patient care. These findings highlight the tensions that emerged when the ideal of the NH as both a home—where residents have autonomy—and a medical institution 31 was challenged by the pandemic.
One particularly challenging factor centered on the rapidly changing regulatory requirements in the first wave of the pandemic. Moreover, from the nurses’ perspective, practicing in accordance with these regulations rendered it nearly impossible to practice individual care in accordance with the ethical guidelines.
Here, one notable example is the nurses’ extensive use of medications, such as sedatives. According to evidence-based knowledge and ethical principles, medication should only be used to relieve patients’ symptoms, not to sedate them to have control. However, to follow the infection-control regulations and protect residents against the virus, nurses felt forced to do things they otherwise would not, such as giving the residents sedatives to calm them. Jia et al. 32 found that health care during the pandemic tended to neglect patient rights. Possible reasons for this are described by Morley et al. 33 highlighting that the pandemic led to allocation of scarce resources. In a review study of ethical dilemmas in nursing practice, Haahr et al. 34 emphasized the perspective of balancing harm and care. The decision to use sedatives may in this way also be connected to balancing scares resources and/or protecting other residents and untrained staff from physical abuse.
The use of constraints in NHs is strictly regulated by law to protect the autonomy and dignity of patients. 35 The nurses in our study described the use of physical constraints such as fences and locked doors, as ethical difficult, but did not explicitly define this as “breaking the law.” However, as noted above, the COVID-19 regulations seemed to trump other regulations and legislation, and the nurses felt obliged to follow the new regulations. The nurses linked the complex situation to the expectations that relatives and community leaders had for their work, and the pressure they felt from society to avoid COVID-19 infections in the NHs. Interestingly, even when they experienced the regulations as barriers to proper care for individual patients and their relatives, the nurses did not describe much opposition to the regulations. This dovetails with Greason’s 22 findings that while NH staff do not experience difficulties making ethical decisions or determining an ethical course of action, they often experience moral distress. To manage this distress in making ethical decisions, staff often comply with what they are instructed to do, out of fear of consequences. They also often delegate decision making to family, “have a meeting,” or are socialized into accepting the workplace culture of doing what you are instructed to do. 22 It is also supported by another of Haahr et al.’s 34 findings that nurses’ ethical challenges in clinical practice often centered around navigating disagreements. Such strategies may contribute to ethical difficult situations when it comes to the nurses’ daily work during the COVID- 19 restrictions. However, one notable exception in our study was the nurse who refused to go to the morgue and use FaceTime with a physician so the physician could confirm the death of a resident. This is an example of one moment of individual opposition, as the situation was experienced as “too absurd.”
Nursing has its starting point meeting the individual patient’s basic needs and providing person-centered care. Nurses have acquired a specialized competence that gives them an independent responsibility to assess and safeguard the tasks they must complete. 36 This is connected to the International Council of Nursing’s (ICN) code of ethics for nurses which provides guidelines for their responsibility toward the patient, co-workers, him/herself—and to society. 18 Our findings show that, for nurses in NHs, balancing these four levels of responsibilities may go beyond the bounds of possibility and become impossible. In a cross-sectional study of nursing home staff during the third wave of the COVID‐19 pandemic, Brady et al. 30 found high levels of post‐traumatic stress, mood disturbance and moral injury. Significantly, more nurses than other staff groups reported poor wellbeing, but nurses were more likely to use adaptive coping styles than non‐clinical staff.
Our findings describe four key ethical dilemmas experienced by nurses during the pandemic; we argue that these ethical challenges emerged because there were different values at stake at the same time. Here, the most prominent issue was the value of utility, looking at the NH, the city, or the society as a whole, and then making choices with outcomes that would be as good as possible for as many as possible—versus the value of meeting the needs and rights of the individual. The nurses in our study also described a conflict between the value of duty (acting according to regulations, legislations, and orders) versus their responsibility for individual patients’ health-related needs. Overall, then, the challenges arose at the intersection between the needs of individuals and the needs of society as a whole.
There is no “quick fix” for the ethical challenges that arise in a situation like the COVID-19 pandemic. However, our findings indicate that leadership and collegial support may play an important role in helping to mitigate the negative impacts of those dilemmas. In this study, some nurses described a lack of support from and trust in their leaders, experiencing them to be ignorant of nurses’ competence and making decisions without them. Other nurses described a supportive cooperation with the NH leaders; notably, these nurses seemed to have better handled the challenging situations that emerged during the pandemic. Their competence as nurses was recognized and they participated with the rest of the interdisciplinary team in the NH. These experiences suggest that good leadership creates a better culture of safety of respect, dignity, and quality. 20
Strength and limitations
To ensure credibility, dependability, confirmability, and authenticity, we have attempted to describe the process in reflexive manner, presenting each stage of the research in detail. The COREQ Checklist has been followed. 37 The informants were recruited due to their clinical experience with COVID-19 and represent an authentic sample, presenting rich descriptions. Interviewing is an unfolding process during which the interviewer acquires new insight into the studied phenomenon. New insight influences the subsequent follow-up questions throughout the interview process.26,27,28
The interviews were conducted by AHH, a female nurse experienced within the field of care for old adults. The pre-understanding of the researcher was made explicit throughout the research process. AHH conducted the initial analysis, from reading the transcripts to making codes. SE participated in the further analysis, in which categories and themes were identified. All authors took part in discussions about the design, methods, and data analysis, and contributed to the writing of the paper.
The study included a small number of participants from Norway, but are diverse in relation to gender, experience with COVID-19, geography and length of experience. Transferability of the findings to other cultures and contexts must be handled carefully. We propose that the issues identified in our study generate new knowledge about experiences of ethical challenges due to COVID-19 in the NH context that may guide further research.
Conclusion
This study reveals ethical challenges occurring at the intersection between the needs of individual NH residents, the protection of other residents, and the needs of society as a whole. The nurses’ ethical challenges were intertwined with external factors, such as national and local guidelines, and the nurses’ subjective professionality. The nursing ideology of person-centered care and the societies’ ideology of an NH as a home for the residents were therefore nearly impossible to manage when the needs of society as a whole had to be prioritized over the individual resident. This duality created ethical difficult situations and inflicted emotional distress, offering nurses limited opportunities to perform nursing in a professional sound and safe manner.
Footnotes
Acknowledgements
The authors are grateful to the nurses who participated.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.