
Abstract
Background
The global pandemic raised ethical issues for nurses about caring for all patients, not just those with COVID-19. Italy was the first European country to be seriously affected by the first wave, while Estonia’s infection and death rates were among the lowest in Europe. Did this raise different ethical issues for nurses in these two countries as well?
Aim
The aim was to describe and compare ethical issues between nurses working during the first wave of the COVID-19 pandemic in Estonia and Italy.
Research design
A cross-sectional survey study with a self-administered questionnaire. The impact of COVID-19 emergency on nursing care questionnaire was used.
Participants and research context
Convenience sampling was used to recruit 1098 nurses working during the first wave of the pandemic in 2020: 162 from Estonia and 936 from Italy.
Ethical considerations
Research ethics approvals were obtained, and the nurses provided informed consent.
Results
The most frequent ethical issues for Estonian nurses were professional communication and ensuring access to care for patients without COVID-19, and for Italian nurses, the end-of-life care and the risk of them getting the virus and transmitting it to their loved ones. There were no statistically significant differences in the frequency of ethical issues between Estonian nurses working with patients with and without COVID-19. Italian nurses caring for COVID-19 patients faced statistically significantly more (both p < .001) issues around prioritising patients and end-of-life. Nurses working with patients without COVID-19 in Italy faced more issues about access to care (p < .001).
Conclusions
Estonian and Italian nurses, working in different clinical contexts during the first wave of the pandemic, faced different ethical issues. Local contextual aspects need to be considered to support nurses’ ethical decision-making in providing care during future crises and to ensure ethical care for patients.
Introduction
The pandemic raised ethical issues for nurses and questions about how to ensure good care for all patients during the crisis, not just those with COVID-19. During the pandemic, nurses had a professional duty to care for an increased number of patients in critical condition1,2 with insufficient resources and a lack of skills, clear rules and protocols. 3 This endangered their health and those close to them. 4 At the same time, they had to expand their focus from patient-centred care to a public health-centred approach.5–7 This challenged nurses to re-evaluate the basic principles of professional ethics.8,9
Although the COVID-19 pandemic affected healthcare systems globally, the impact varied in different countries. During the first wave, Italy was one of the countries that was hit hardest, and Estonia managed to avoid more serious consequences. The pandemic influenced the ethical issues 10 that the nurses had to address and the decisions they made in different clinical and sociocultural contexts. However, there have been limited comparisons of the ethical issues in varying contexts in different countries and related to COVID-19 and non-COVID-19 patients. This knowledge is needed to deepen understanding about ethical issues as a reflection of care contexts and to enhance ethical care for patients during future crises.
Background
Standards of care and ethical values vary from the norm during times of crisis as conflicts increase the number of patients to be cared for with the same or fewer resources.11,12 From an ethical perspective, the COVID-19 pandemic challenged how nurses provided patient care, as they had to balance between conflicting duties,8,13 particularly if they were taking care of COVID-19 patients. 14 There was a lack of care equipment and evidence-based knowledge, but also skills and protocols, preventing nurses from following the standards and principles of care.6,13 During the pandemic, nurses witnessed that patients’ rights were not fulfilled and they did not receive fair and equal care. There were postponed or cancelled scheduled appointments and hospital admissions for non-COVID-19 patients, endangering their health, and continuity and equality of care. 15 The strict infection control procedures protected public health but also reduced holistic, patient-centred care and the direct contact between nurses, patients and families. In addition, visits by family members were restricted to prevent the spread of the virus, limiting their right to participate in decision-making about their health and care.3,13 Thus, patients were left without the support of loved ones and dignified care, especially during end-of-life care.6,14
During the COVID-19 pandemic, nurses also encountered ethical issues regarding working in care organisations and providing frontline care during crises. Nurses were not informed about the organisational expectations of how to work during the crisis. 16 They risked their own and their loved one’s safety when taking care of others.5,8,13 This caused ethical issues regarding altruism and duty to care,6,17 how simultaneously to help patients and protect themselves and their loved ones.8,16,17 Professional teamwork and mutual support by colleagues were valued by nurses as they managed the consequences of the pandemic.4,14 However, the pandemic also challenged collegiality, professional relationships and communication between team members. Nurses perceived tension during their communications with colleagues, 17 they disagreed with team members about treatment decisions, and they felt they were excluded from decision-making, which affected the adequacy of the care they provided.5,6 In addition, nurse managers were obliged to recruit students and new staff with limited experience and skills, endangering the quality of work and safe care. 17 Thereby, ordinary nursing work during the pandemic caused ethical issues for nurses, challenging basic nursing values and professional collaboration. Working in such a context caused moral distress to serious moral injury for nurses consequently.18,19
The COVID-19 pandemic has been the most serious health crisis in recent decades 20 and it affected the healthcare systems, economies and social functioning of both Estonia 21 and Italy. 22 Italy was the first European country to be seriously affected by the COVID-19 pandemic. 23 After the infection started in February 2020 it rapidly increased and affected the functioning of the healthcare system, a lack of hospital and intensive care beds, 24 and a lack of personal protective equipment and tests. 25 The first wave started in Estonia in March 2020, and progressed much less aggressively, 26 causing the lowest rates in Europe. 27 Adequate access to hospital beds was maintained during this period, especially to intensive care.28,29
The governments of both countries established different step-by-step restrictions, including social distancing, extensive testing and isolating positive cases and contacts.26,30 In Italy the focus was on responding to the complicated clinical situation, and in Estonia, responding to the possible worse-case scenario. In addition, healthcare systems needed to be extensively reorganised to prevent the spread of infection and maintain functioning and continuity of care. This included restricting visits to hospitals and care homes, postponing or cancelling, scheduled work and setting up special COVID-19 departments in hospitals and primary care settings.28,31 Both countries also established ethical recommendations for providing care when resources were so scarce. The main criteria that drove treatment decisions in both countries were prognoses of treatment success and further quality of life.31,32 Caring and respecting human dignity and the patient’s wishes were important values in Estonia and highlighted in guidelines. 31 The focus in Italy was on age, good palliative care and involving patients, their loved ones and healthcare staff in decision-making processes. 32 Mutual support between healthcare personnel and care institutions was highlighted in guidelines and recommendations in both countries.31,32
Aim
The aim of this study was to describe and compare ethical issues between nurses working in Estonia and Italy during the first wave of COVID-19 pandemic. The ultimate aim was to deepen understanding about the influence that context had on the ethical issues faced by nurses, to enhance ethical care for patients during crises.
The research questions were: - What were the most frequent ethical issues faced by nurses during the first wave of the COVID-19 pandemic in Estonia and Italy? - How did the ethical issues faced by nurses differ when they were taking care of patients with and without COVID-19?
Methods
Study design and research environment
A cross-sectional study design, 33 with a structured anonymous self-reported questionnaire 34 was conducted among nurses working during the first wave of the COVID-19 pandemic in Estonia and Italy. The number of nurses in both countries (6.2 nurses per 1000 inhabitants) was below the Organisation for Economic Co-operation and Development average. 35 There are approximately 8400 Estonian- or Russian-speaking registered nurses working in Estonia and approximately 264,500 nurses working in Italy. 36 In both countries, most nurses work in public hospitals and nursing education is based on the Bologna declaration. 37
Procedures
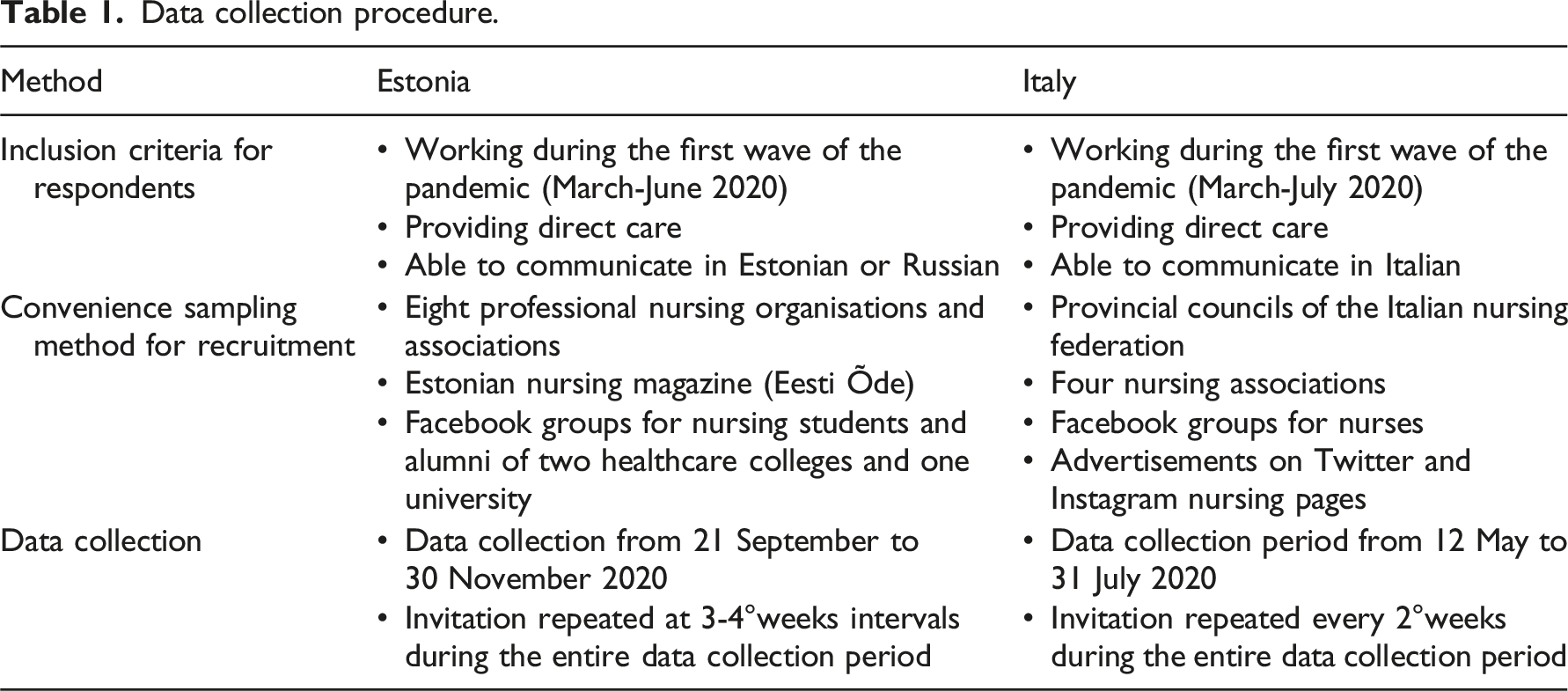
Data collection procedure.
Instrument
The data were collected using The impact of COVID-19 emergency on nursing care questionnaire. 39 The aim of the questionnaire is to measure how the pandemic impacts nursing care and comprises 26 questions divided into five sections: (i) work organisation and (ii) working context for nurses, (iii) nursing care activities, (iv) ethical issues in care and (v) educational needs for COVID-19 nursing. These were divided into 10 multiple choice questions, 11 questions based on a five-point Likert-scale, ranging from one for not at all/never to five for most of the time/always/completely, three numerical questions and two open-ended questions. Due to the descriptive purpose of the questionnaire, no cut-offs were defined, but exclusively the frequency with which participants rate the impact of the pandemic on different aspects of care. In addition, the questionnaire contained 19 sociodemographic background questions regarding age, gender, religious identity, nursing education, work details and whether they had been tested for the virus that causes COVID-19. Completing the questionnaire required to provide answers to all questions to proceed.
The questionnaire was developed in 2020 by a research group consisting of lecturers and postdoctoral fellows in nursing science. The questionnaire was piloted among 20 nurses, who assessed its content validity and face validity. 39 The original questionnaire was in Italian and was translated into English by a bilingual translator. In this study, the Estonian questionnaire was translated from English to Estonian, using the back-translation technique. 40 First, the researcher (GU) translated the questionnaire to Estonian and then it was edited by a professional language editor. After that, the questionnaire was culturally adapted to the Estonian context, ensuring that nursing and healthcare organisations and services and employment statuses were correctly categorised. After that, the instrument was pilot-tested by an expert group with five members, including three nursing science lecturers, two doctoral students at a medical faculty and five nurses in clinical practice. The questionnaire was also translated into Russian by a language editor and pilot-tested among five Russian-speaking nurses in clinical practice. The internal reliability of the questionnaire was assessed using Cronbach’s alpha coefficient. The alpha value for the whole questionnaire was 0.92 in Estonia and 0.83 in Italy. The fourth section of the questionnaire (ethical issues in care) showed an alpha value of 0.72 in Estonian and 0.79 in the Italian version.
Study variables
In this study, we will report the items regarding ethical issues. 39 There are altogether nine items regarding different types of ethical issues faced during the pandemic. Respondents were asked to estimate how often they have faced ethical issues, using a five-point Likert-scale from one for not at all to five most of the time. These included how often the nurses needed to guarantee patients without COVID-19 had adequate access to care, decide which patients to prioritise and provide patients and their loved ones with transparent information. They also needed to evaluate, how often they had to guarantee that patients received adequate end-of-life care, died with the feeling that their loved ones had attended and that their body was respected when they had died. In addition, they had to evaluate, how often they had to put their own and their loved ones’ health at risk because of work and about giving complete information to colleagues and to follow their employers’ directives, even if they conflicted with their ethical and deontological principles. We also considered six sociodemographic background variables: age, gender, level of education, working years, healthcare setting and religious identity.
Statistical analysis
STATA 14 (StataCorp LLC, Texas, USA) was used to analyse the data by country and whether the nurses worked with COVID-19 patients or not. Likert scores for the frequency of ethical issues were dichotomised into two groups: seldom related to responses 1-3 and often incorporated responses 4 and 5. Descriptive statistics were used to report background information and the frequency of ethical issues in both countries. Ethical issues were considered frequent if 55.5% or more of the nurses in the groups scored this factor 4 or 5. Student’s t-test was used to test for differences of means. Fisher’s exact test (p < .05) and 95% confidence intervals (CI) were calculated for the statistical significance of the differences between the groups. Questionnaires with missing information were not included in the analysis.
Ethical considerations
We followed the principles of good research practice 41 and ethical principles for medical research 42 throughout the whole study. The study was approved by the Research Ethics Committee of University of Tartu (Protocols numbers 281/T-3 from 16.04.2018, 322/T-7 from 17.08.2020 and 341/M-3 from 15.05.2021) and University of Torino (Approval no. 279061 – 01/07/2020). Respondents were informed about the aim of the study, the fact that participation was anonymous, and voluntary and what were the principles of data protection and confidentiality. Responding to the questionnaire provided informed consent. Participation could be withdrawn at any time during the completion of the questionnaire, without consequences. The data gathered from the nurses in the two countries were stored in secured servers at the University of Tartu and University of Torino.
Results
Sociodemographic and work-related background
The sociodemographic background characteristics (%) of the 1098 nurses.
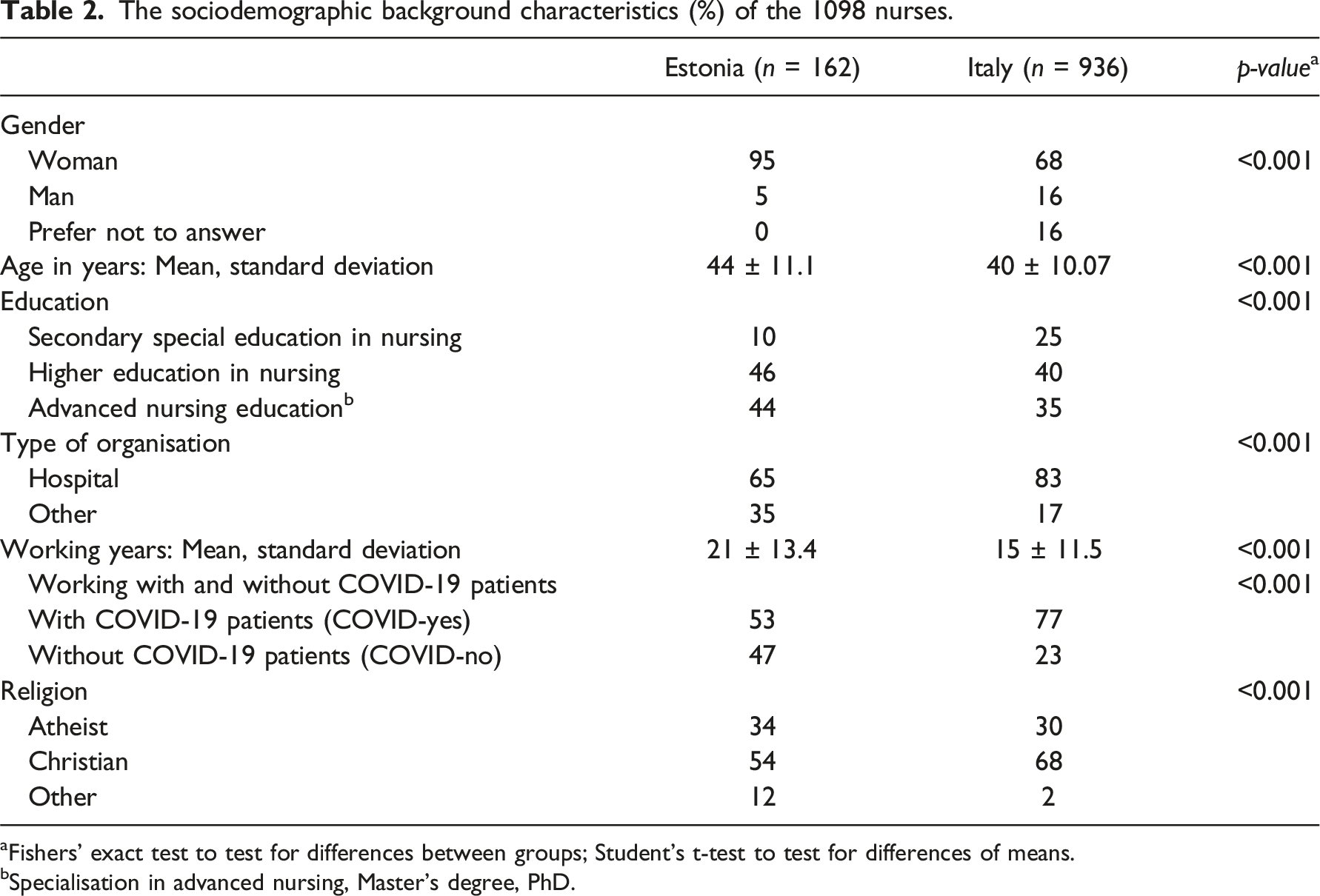
aFishers’ exact test to test for differences between groups; Student’s t-test to test for differences of means.
bSpecialisation in advanced nursing, Master’s degree, PhD.
Main ethical issues for nurses in Estonia and Italy
Frequency (n (%)) of ethical issues for nurses in Estonia and Italy.
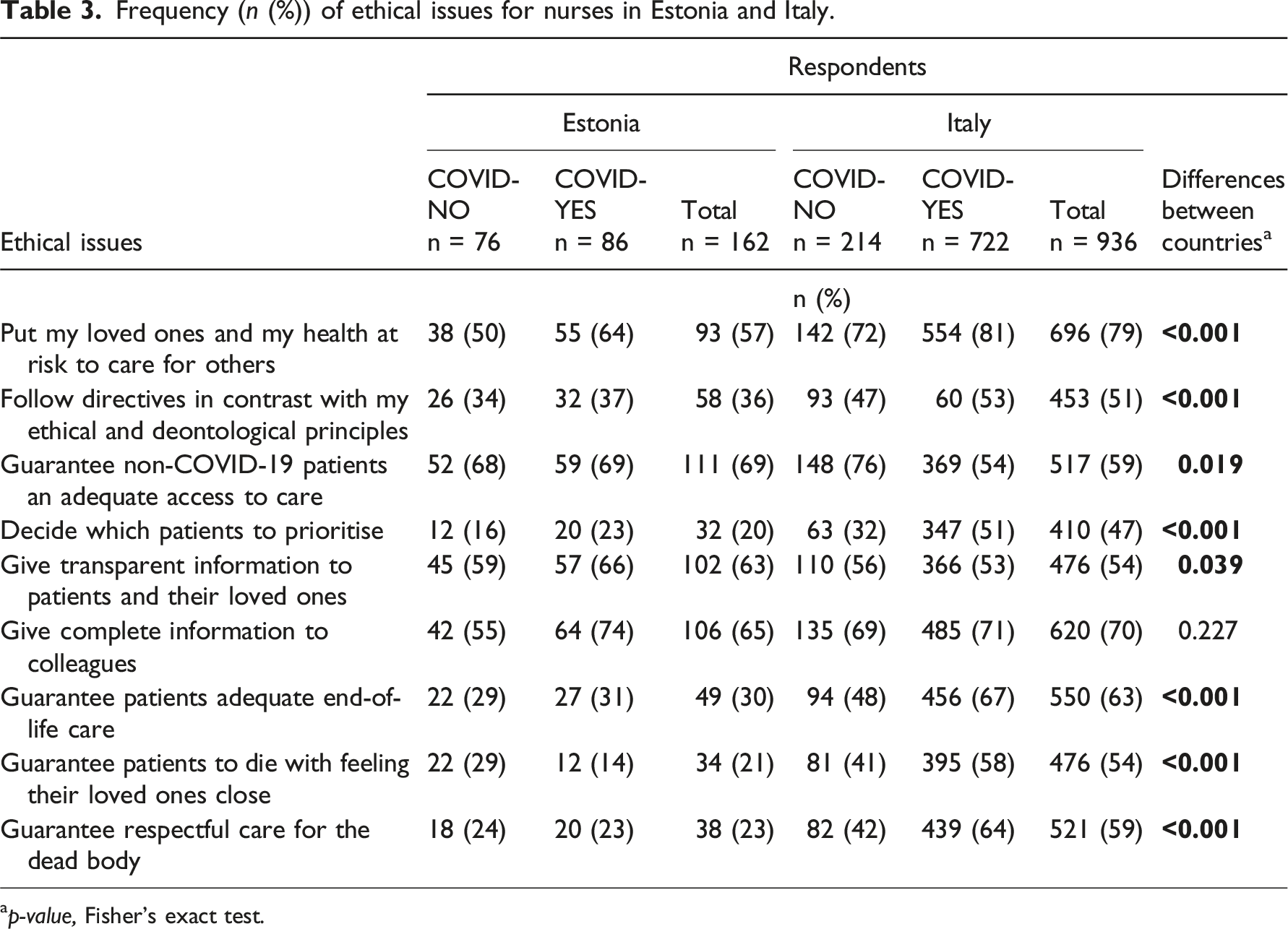
ap-value, Fisher’s exact test.
Main ethical issues and differences between nurses working with patients with and without COVID-19
Estonian nurses working with COVID-19 patients in Estonia said that the most frequent ethical issues were giving complete information to their colleagues (74%) and guaranteeing access to care for patients without COVID-19 (69%). Other frequent issues were providing transparent information to patients and their loved ones (66%) and putting their loved ones and themselves at risk of infection (64%). Nurses working with patients without COVID-19 in Estonia said that the most frequent ethical issues were guaranteeing patients access to care (68%) and providing information to patients and their loved ones (59%) and colleagues (55%). (Table 3) The frequency of ethical issues did not show a statistically significant difference between nurses working with and without patients with COVID-19 (Figure 1). The frequency of ethical issues for nurses. Based on proportions (percentages and 95% CIs) of nurses, who estimated that the frequency was high (scores 4 and 5). * Statistically significant differences, p-values, Fisher’s exact test.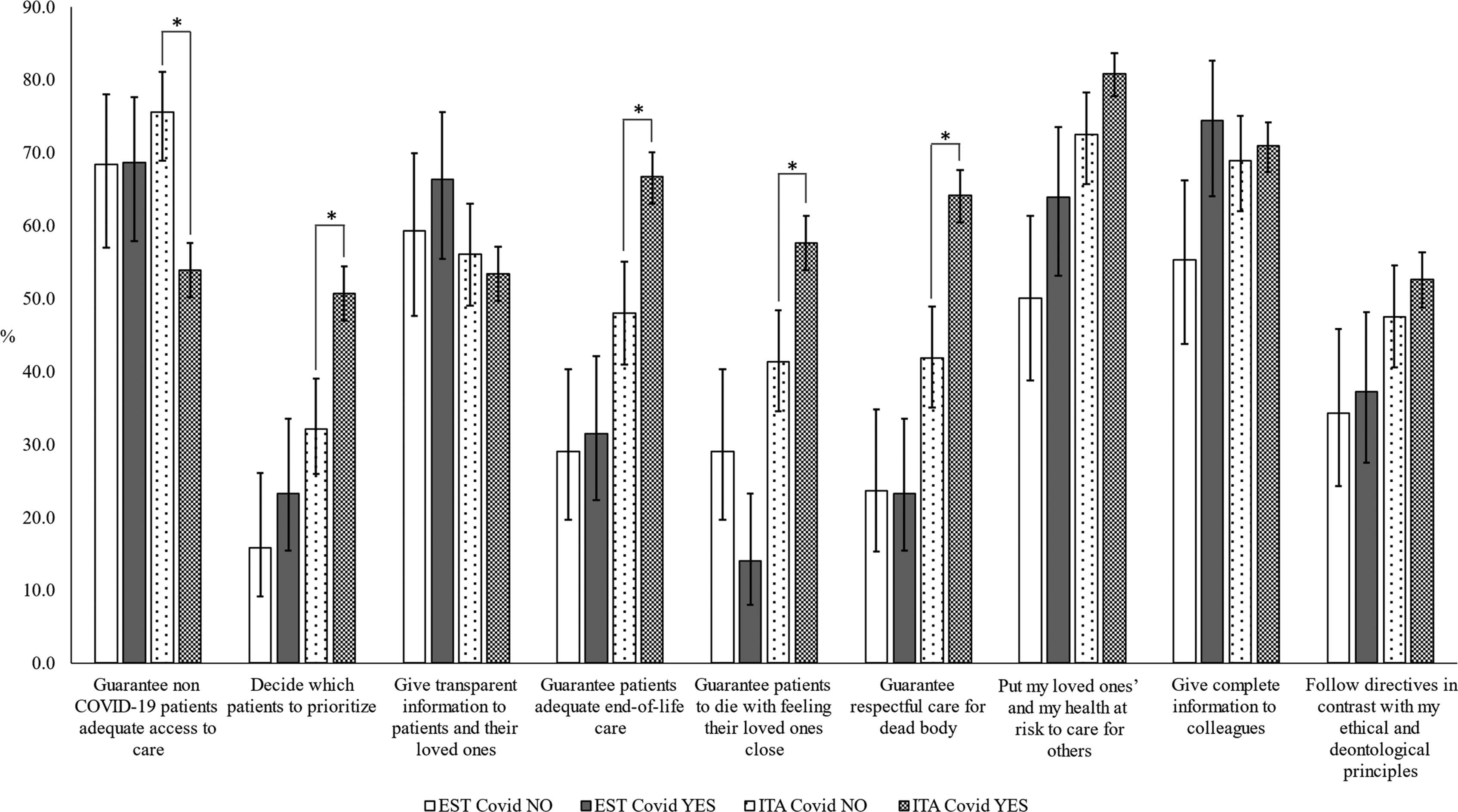
Italian nurses working with COVID-19 patients said that the most frequent ethical issue was putting their health, and that of their loved ones, at risk to care for others (81%). That was followed by giving complete information to colleagues (71%), guaranteeing adequate end-of-life care to patients (67%) and guaranteeing respectful care for dead bodies (64%). The most frequent ethical issues for Italian nurses working with patients without COVID-19 were guaranteeing them access to care (75%), putting their loved ones and themselves at risk of infection (72%) and providing complete information to colleagues (69%) and patients and their loved ones (56%). (Table 3) Nurses working with COVID-19 patients faced more frequent issues about prioritising patients and end-of-life situations (p < .001 for all) than nurses working with patients without COVID-19. Meanwhile, nurses working with patients without COVID-19 faced more frequent ethical issues around guaranteeing access to care for patients without COVID-19 (p < .001) (Figure 1).
Discussion
This study provides new knowledge about the ethical issues that Italian and Estonian nurses faced during the first wave of the COVID-19 pandemic. It compared the two countries and also looked at nurses working with patients who did and did not have COVID-19. The first wave of the pandemic progressed differently in the two countries, as Italy had 10 times as many deaths and patients requiring hospital treatment than Estonia. The ethical issues faced by the nurses were also different in the two countries and our results also reflect highlights in the clinical contexts.
The nurses who took part in our study frequently encountered ethical issues regarding providing care to patients during the pandemic, especially those working with COVID-19 patients. These results confirm previous research, which highlighted ethical issues during the pandemic, as a result of disruptions in access to healthcare. 15 These disruptions had an impact on fair, equal,6,43 holistic and patient-centred care.5,13 Our results were consistent with another study, which reported that nurses working with COVID-19 patients faced more ethical issues than those who did not. 14 Therefore, our results reinforce existing research that nurses face significant ethical challenges in delivering patient-centred care during crises particularly when they lack the skills and previous experience of handling disasters on such a scale.5,6 The COVID-19 pandemic has taught us that it is not possible to continue conventional, patient-centred care during crises by following the same hierarchy of ethical principles as we do during normal times. 12 During COVID-19, nurses had to focus more on community-centred care to handle the pandemic and continue to provide care when resources were scarce. 11 Both Italy and Estonia supported the work of healthcare workers by establishing ethical recommendations to help them to do that,31,32 but these were only available after the first wave. In future, it is important make sure that such protocols have already been prepared and that nurses are familiar with them before any crisis. Nurses are also the main frontline staff and should be involved more in discussions and decisions about preparing guidelines, instead of just following them, as this could provide another source of ethical issues for them.13,44
The Estonian nurses in our study did not report many ethical issues regarding prioritising patients and end-of-life situations. However, these issues were frequently reported by Italian nurses, especially those working with COVID-19 patients. Country-based differences in the ethical issues faced by the nurses in the two countries reflected the different progress of the pandemic in the two countries. They underline the fact that the COVID-19 pandemic was not a completely uniform phenomenon with the same characteristics in different countries. Although nurses working during the pandemic have reported similar experiences in different countries, 13 we need to consider some unique contexts to understand that phenomenon comprehensively. Our results were in line with studies that investigated ethical issues faced by nurses in similar clinical contexts to Italy during the pandemic, with high numbers of infected patients in critical conditions. Studies have reported that unprecedented working conditions and high workloads raised ethical issues that forced nurses to prioritise who they were able to help.6,43 Those were also reported by the nurses in our study. High mortality rates among COVID-19 patients heightened ethical issues related to end-of-life care, as indicated by earlier research that explored the perspectives of nurses. Providing dignified end-of-life care was challenging for nurses, especially for those caring for COVID-19 patients during pandemic. This challenge stemmed from social distancing requirements, which affected in-depth communication between nurses and patients and isolated patients from their loved ones when they were dying.6,13,14 Therefore, it is imperative to explore alternative modes of communication and assess their weaknesses and advantages. This would help to improve patient-centred communication, and the involvement of the families in the care process, during similar crises to the pandemic.
The nurses in our study faced ethical issues related their safety and the safety of their loved ones while working in environments where they had a heightened risk of getting infected with a possibly life-threatening infection. This was particularly true in Italy, where the pandemic had a huge impact on healthcare systems. The overwhelming fear that nurses had for their safety, and the safety of their loved ones, has been extensively highlighted as a prominent feature of the COVID-19 pandemic.5,6,13,17 This pandemic forced nurses to balance their personal rights, professional duties and work-life balance. It also meant they had to give more priority to their safety and self-care alongside their duty to provide care for others. 13 This created a dilemma. Nurses were needed more than ever, to help manage the pandemic and its consequences. However, there were already serious problems, due to nursing shortages, and these worsened even more due to their need to protect themselves and their loved ones. Nurses showed high commitment to professional duties during the pandemic. 16 However, in managing crises like the COVID-19 pandemic, it is important to respect nurses’ right to stay safe and take care of themselves and their loved ones as well, in addition to considering them primarily as socially owned crisis resources with the obligation to care.8,12 Working with constant fears and worries about their safety was exhausting for nurses and could have fostered mental health problems. 6 It is important to recognise that pandemics have a significant physical and psychological impact on the nursing workforce and thereby weaken their capacity to respond to these health crises effectively. Innovative solutions are needed to empower nurses, both at individual and population levels.
Our results highlight that focussing on consequentialist, community-centred care during the pandemic instead of patient-centred care was challenging for nurses. This underlines the need to adequately address the serious moral injury and long-term consequences, that working during the pandemic can cause for nurses, 18 support them in coping with it and prepare nurses for similar crises. Firstly, it is important to prepare nurses for the ethical aspects of crises before they happen. 12 Being prepared for crises should be a standard feature of working in healthcare and regular training should be provided. 16 Making ethical decisions in crises should be a critical competency for nurses, with preparedness being part of their basic education and training. This should be regularly and consistently provided during their professional career. It is particularly important, considering the role that ethical issues play in developing moral distress, moral injury, burnout and nursing shortages.18,19 Secondly, there needs to be open discussions with local communities about the standards of care that are acceptable during crises. The COVID-19 pandemic has distressingly highlighted that it is not sufficient to just ask questions about how to provide care when resources are scarce and conventional principles are not sufficient. 22 Nurses and community members both have very practical and immediate experiences of how crises influence healthcare provision and what choices need to be made. This was convincingly demonstrated by the shock that the public demonstrated in both Italy and Estonia in traditional and social media coverage about the impact of the pandemic. Involving people in discussions about their health and care, at both individual and community levels, is an inevitable part of ethical care. 45
Implications for nursing
Understanding the ethical issues that nurses faced during the pandemic is necessary to identify gaps in patient care, by addressing which care institutions can enhance ethical care to patients in future crises. Moral burden causes short-term consequences for individual nurses and patient care. 19 In addition, they cause also long-term consequences affecting nurses’ health and well-being and their willingness to stay committed to the nursing profession. 18 Using strategies to manage the consequences of the current pandemic and preparing for future ones, care organisations should consider crises also from an ethical perspective. For both care organisations and educational institutions, it is important to develop targeted strategies that support nurses in ethical decision-making, such as creating ethical guidelines tailored to crises and integrating ethical decision-making tools 11 into clinical settings. Investigating ethical issues in different countries enables to expand the understanding of the diversity of professional ethics, fosters global collaboration and contributes to the long-term preparedness of nurses.
Limitations
This study had some limitations regarding the research design, data collection, recruitment and representativeness of the respondents. A cross-sectional study design does not allow researchers to evaluate causal inference. 33 Despite nurses in both countries getting degree nursing education based on the same principles according to the Bologna declaration, 37 the differences in cultural, religious, historical and legal background in different countries need to be considered regarding nurses’ ethical issues. Retrospective self-reporting data collection could have led to some recall bias, which could have been limited by a shorter period between the start of the pandemic and the data collection period.
Convenience sampling may have meant that the research invitation did not reach all nurses who met the inclusion criteria, and this made it difficult to calculate the exact response rate. However, we used the widest possible recruitment strategy, based on our best knowledge, to inform nurses about the study. The response rate was relatively low in both countries but corresponded to the number of nurses working in those countries. However, the pandemic and the nurses’ extensive workload during that period might have reduced the responses to those who were willing to share their experiences. This meant that Italian nurses from the most affected regions participated, skewing the geographical spread of the sample. On the other hand, the sample in Estonia was geographically balanced and representative of nurses in terms of the main background characteristics. 46 An overwhelming number of respondents in both countries were hospital nurses, which may indicate their higher sensitivity towards the research topic and a greater interest in sharing their experiences. 47 However, most Italian and Estonian nurses work in hospitals. 46
Conclusions
The ethical issues faced by nurses during the pandemic reflected the progress of this international health emergency, the context of the nurses’ work and whether they worked with patients with or without COVID-19. The most pressing ethical issues for nurses were the need to provide dignified and holistic end-of-life care and provide care when healthcare system was overwhelmed by patients in critical condition and a lack of resources. Although the nurses were dedicated to caring for their patients, they were also acutely aware of the risks that the infection posed to themselves and their loved ones. Guaranteeing access to care for patients without COVID-19 patients was an important ethical issue for Estonian nurses during the pandemic, as the spread of the infection was less aggressive there than in Italy. A lot of effort was put into preparing for the worse-case scenarios in Estonia. Communication with colleagues, patients and their loved ones was equally important for nurses in both countries in terms of the pandemic, despite its consequences on their clinical work. Looking forward, nurses need continuing training and advanced support from healthcare institutions regarding the ethical issues related to future pandemics. This would improve their preparedness to make the prompt switch from a patient-centred to community-centred approach. In addition, healthcare professionals and local communities need to develop a shared understanding about the acceptable ethical standards of care provided by nurses during healthcare crises. This would support nurses during future health emergencies.
Further research needs to explore the perspective of nurses and patients, so that we can develop a deeper understanding of how crises influence ethical issues related to care. This should explore questions, impacts and expectations. In addition, more studies are needed on nurses’ perspectives, their experience of working with established ethical guidelines during pandemics and how those guidelines reflected nursing values. Another topic to consider is how cultural, religious, historical and legal factors influence nurses’ ethical issues and decision-making. The knowledge is needed to support nurses’ professional ethics in rapidly changing healthcare contexts.
Footnotes
Acknowledgements
We would like to thank all the nurses who participated in this study for their time and contribution and all the nursing organisations who helped us to recruit participants.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.