
Abstract
The aim was to synthesize the findings of empirical research about the unmet nursing care needs of older people, mainly from their point of view, from all settings, focusing on (1) methodological approaches, (2) relevant concepts and terminology and (3) type, nature and ethical issues raised in the investigations. A scoping review after Arksey and O’Malley. Two electronic databases, MEDLINE/PubMed and CINAHL (from earliest to December 2019) were used. Systematic search protocol was developed using several terms for unmet care needs and missed care. Using a three-step retrieval process, peer-reviewed, empirical studies concerning the unmet care needs of older people in care settings, published in English were included. An inductive content analysis was used to analyse the results of the included studies (n = 53). The most frequently used investigation method was the questionnaire survey seeking the opinions of older people, informal caregivers or healthcare professionals. The unmet care needs identified using the World Health Organization classification were categorized as physical, psychosocial and spiritual, and mostly described individuals’ experiences, though some discussed unmet care needs at an organizational level. The ethical issues raised related to the clinical prioritization of tasks associated with failing to carry out nursing care activities needed. The unmet care needs highlighted in this review are related to poor patient outcomes. The needs of institutionalized older patients remain under-diagnosed and thus, untreated. Negative care outcomes generate a range of serious practical issues for older people in care institutions, which, in turn, raises ethical issues that need to be addressed. Unmet care needs may lead to marginalization, discrimination and inequality in care and service delivery. Further studies are required about patients’ expectations when they are admitted to hospital settings, or training of nurses in terms of understanding the complex needs of older persons.
Introduction
The increase in the older people population in many countries has led to a growing demand for healthcare services. 1 These demands from older people are varied depending on their comorbid conditions and functional ability. Policy makers and other stakeholders are beginning to recognize and anticipate these trends which require healthcare systems to function as effectively and efficiently as possible, serving all older citizens equally with appropriate and affordable care. 2,3
If a nursing care need has been adequately addressed that care need has been met. A care need met in the context of mental healthcare is A physical, psychological, social or environment-related demand for help, care or a service, with the goal of solving or reducing a problem that is experienced or expressed by an older person in relation to an underlying psychiatric condition.
4
Unmet care needs can herald threats to safety, the successful management of acute or chronic health problems and consequential negative health-related events. 9,10 As nurses represent the largest group of healthcare professionals, 7 unmet needs related to nursing care warrants closer examination and recognition. However, unmet nursing care needs from the point of view of older people, or care receivers in general, are different from those defined from the viewpoint of professionals or systems. This review focused on the older individual’s perspective. However, the informant or identifier of unmet care needs could be the informal caregiver, family member or a professional.
All people are entitled to quality nursing care while being cared for in institutions as patients. 11,12 Older people are a heterogeneous group whose needs are increasingly diverse. Although some outdated stereotypes still may exist, new expectations, such as reducing inequity, dealing with diversity, enabling of choice and ageing in place, have to be managed. 13 These new expectations are dashed by studies demonstrating unmet care needs for many groups of patients, such as those with advanced cancer 14,15 and patients with dementia 16 –18 or mental illnesses. 19,20
Unmet care needs seem to occur largely in informational (30%–55%), psychological (18%–42%), physical (17%–48%) and functional (17%–37%) domains. 15 This finding is supported by Puts et al. 21 who, in a review focusing on older people suffering from cancer, found that unmet care needs existed mainly in psychological, information and physical domains. More specifically, a recent systematic review reporting on patient outcomes in acute hospital care settings showed associations between missed care and a range of poor patient outcomes. These outcomes were decreased patient satisfaction, increased medication errors, urinary tract infections, patient falls, pressure ulcers, critical incidents, lower quality of care and patient readmissions. 10 In addition, Johnson et al. 22 reviewed the unmet care needs of people in home care settings and pointed out significant gaps in home care services for older people in Canada.
Unmet care needs have also been found, relating to patient outcomes, including death. 9 Other adverse events include falls, 23 inadequate nutrition, 24 depression, 25 incontinence, 6 discomfort or inconvenience, 26 and institutionalization, 27 which may lead to a decrease in quality of life. 28 These studies focused on unmet needs from the nurses’ point of view. 29 However, it is necessary to analyse the health and well-being domains of the unmet needs of older people using patient views. 8,13,30 This analysis will be an important precursor to the development of care and services which are more individualized, tailored and supportive to older people, 8,11 responding to the need for person-centred care. There is an increasing number of older individuals with chronic conditions in the world. 8 There is also a desire to provide quality care assessments and provision for all, tailored to the individual’s needs and based on correctly assessed care needs and provision as a right. 31
Several studies have analysed patients’ care or assistance needs, based on descriptions of, for example, Activities of Daily Living (ADLs) and Instrumental Activities of Daily Living (IADLs). 32 Other ways include lists of tasks based on nursing care using different terms and identified nursing duties or tasks. 29 This analysis requires a common and pragmatic understanding of ‘unmet needs’. In a systematic review, Jones et al. 29 described three main approaches to understand unmet care needs using terms such as ‘unfinished care’, ‘missed care’ and ‘the implicit rationing of nursing care’. However, studies conducted using these concepts focus mainly on nurses’ reports of nursing activities and care left undone, and there is a dearth of evidence about defining the concept of ‘unmet needs’ from the perspective of older people. More research into unmet care needs using patients’ views is needed, to provide a more detailed and balanced analysis of nursing care and the nursing care missed, unmet and unplanned. The information from this review will help in discussions of inequalities in access to care and care assessment, planning and provision; patients’ rights; the provision of quality care; and missed care.
Aims and objectives
The aim of this scoping review was to synthesize the findings of empirical research about the unmet nursing care needs of older people identifying the breadth, depth and scope of the current literature. The study is a part of the RANCARE project (CA15208 – Rationing – Missed Nursing care: An international and multidimensional problem).
The specific research questions were as follows: What are the methodological approaches used? Which concepts and terminology have been used? What unmet care needs have been identified? What ethical issues have been raised?
Methods
This scoping review, after Arksey and O’Malley, 33 was used to identify gaps in the current research literature and so provide a guide for a future research agenda. The scoping review used the following process: (1) Identifying the research question(s), (2) Identifying relevant studies, (3) Study selection, (4) Charting the data and (5) Collating, summarizing and reporting the results.
Literature search for identifying relevant studies
The systematic literature search used two international scientific databases, CINAHL (from earliest to December 2019) and Medline (PubMed, from earliest to December 2019) on 18 December 2019. These two databases have been found to be the most appropriate and comprehensive in the field of health sciences. 34 The search terms were (‘unmet care needs’ OR ‘unmet need’ OR ‘unmet needs’ OR ‘unfinished care’ OR ‘missed care’ OR ‘care left undone’ OR ‘unmet nursing care’) AND nursing AND (older OR aged OR elder* OR senior) used in various phrases with the Boolean operators. Unmet care needs considered from older people’s point of view did not exclude the participants, for example, professionals. Therefore, these terms were selected to cover all possibilities. Unfinished care, missed care and care left undone were included as these concepts refer to care that is based on needs assessment, but for many reasons was interrupted or not actualised. These selected terms were applied to the title and abstract level of the retrieved studies written in English. The search produced 120 studies (32 from CINAHL and 88 from Medline). In addition, a manual search of reference lists from the retrieved studies produced four additional studies increasing the total to 124. After this initial retrieval, 12 duplicates were removed, then the titles and abstracts were screened by two independent researchers (D.K., R.S.) against the inclusion and exclusion criteria (Figure 1).
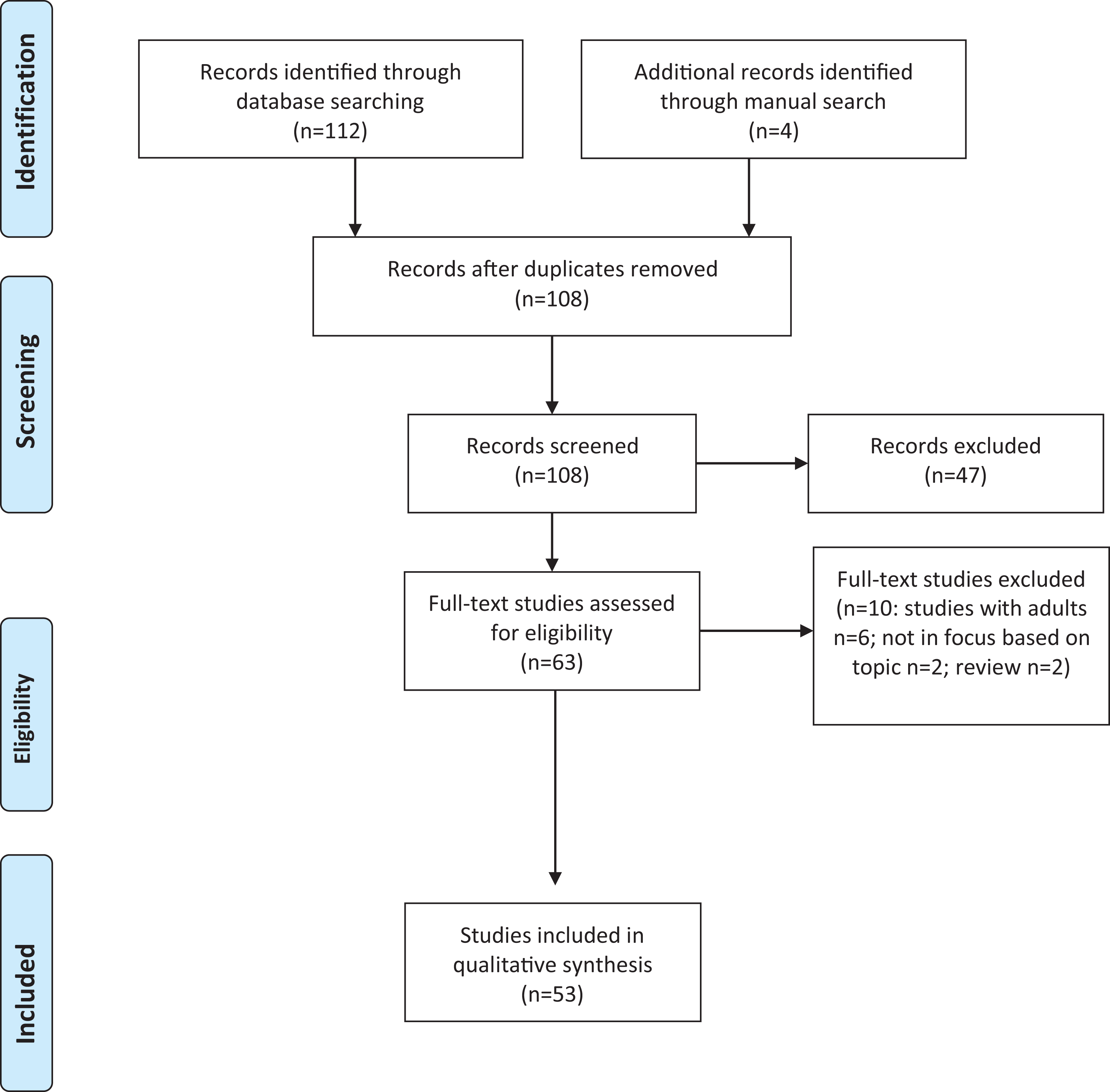
Flow chart of the literature search.
Inclusion and exclusion criteria for selecting the studies
The predefined inclusion criteria were that the study (1) uses empirical research published in a peer-review journal; (2) is written in the English language; (3) focuses on the topic of interest – unmet nursing care needs of older people, and nursing care responsibility, performed by all levels of nurse professionals (unmet care needs, unmet needs, unfinished care, missed care, care left undone, unmet nursing care and care rationing); and (4) concerns older people, 65 or over, 13 their care settings or their context. Studies were excluded if they were (1) reviews, editorials, case studies or narratives; (2) studies not involving older people in their care settings; and (3) not about nursing care. Using the inclusion and exclusion criteria, 63 full-text studies were selected for further inspection.
The full-texts of the 63 studies were then examined. During this examination, the two independent researchers (D.K., R.S.) could not reach an agreement about the inclusion of 10 of the retrieved studies. A third researcher (M.S.) evaluated the studies, and consensus was reached between the three analysts. Fifty-three studies were included in the final analysis.
Data extraction and analysis
The following information was collected and charted into working sheets in a table format by two researchers: author, year, country, study aim, study design, sampling method, sample size, informants, data collection, data analysis, healthcare context, research concept and main findings. The data were analysed using a content analysis approach by searching for responses applied to the stated research questions. Data condensed and charted in tables were then discussed in the research team and double checked by its accuracy (10% of the material). Unmet care needs were identified from the articles from the results sections, tabulated and then categorized according to the World Health Organization (WHO) classification. 28 Regarding the ethical issues, text in articles was read through identifying any ethical concern stated by the authors, such as words, sentences or phrases, and were tabularized and coded. Then the material was extracted and analysed by the constant comparison method. The expressions and wording used by both the participants in the studies, and study authors were used in the analysis wherever possible to reduce interpretation.
Results
Description of the studies included
Most of the reviewed studies were conducted in the United States (n = 22), Australia (n = 3), Canada (n = 2) and Europe (n = 22). In Europe, the studies were conducted in the United Kingdom (n = 10), Switzerland (n = 3), Netherlands (n = 2), Finland (n = 2), and Norway, Portugal, Poland, Germany and Spain, one in each. In addition, studies were conducted in Asia, Japan (n = 2), and Korea and Taiwan, one in each.
Most of the studies were conducted in residential or nursing home contexts (n = 23). The rest were conducted in community settings (n = 6), home care (n = 7), hospital settings (n = 5), primary care (n = 5), rural group practice (n = 1) or in other settings (n = 6). The sample sizes varied from 13 to 71,669 and depended on the study design. In most of the studies, the informants were older people (n = 33); their informal caregiver, relatives (n = 5); or both (n = 2). In some studies, healthcare professionals (n = 12), including registered nurses (n = 3), were the informants.
Methodological approaches of the studies
The most frequently used methods were questionnaire surveys (n = 38), followed by interviews (n = 7), the use of administrative data and patient documentation (n = 4), focus groups (n = 2) and demographic data (n = 2). Several instruments measuring unmet care needs were identified: the MISSCARE Survey 35 ; the Basel Extent of Rationing of Nursing Care (BERNCA) 36 and adapted for nursing homes (BERNCA-NH) 37 in Switzerland; and the Camberwell Assessment of Need of the Elderly (CANE) developed by Reynolds and colleagues 38 from the original instrument Camberwell Assessment of Need (CAN) 39 using data from the United Kingdom, Sweden and the United States. The names of the instruments reveal that their target concepts vary, being missed care, rationing and unmet care needs, respectively.
Concepts and terminology used
An unmet care need has been described as a problem for which an individual is not receiving an appropriate assessment or intervention that could potentially meet the need.
40
(Using the Iliffe et al.
41
definition)
Description of studies included in the analysis.

GP: general practitioner; ADL: Activities of Daily Living; IADL: Instrumental Activities of Daily Living; RN: registered nurse; BERNCA: Basel Extent of Rationing of Nursing Care; AMI: Acute Myocardial Infarction; CHAID: Chi-square automatic interaction detection; MMSE: Mini-Mental State Examination; P4P: pay-for-performance; EOL: end-of-life.
In the literature reviewed, few studies described the theoretical basis for unmet needs in older people. Berridge and Mor 88 used the cumulative disadvantage theory of Dannefer and colleagues to explain the unmet needs in the context of health-related inequalities in older people. Similarly, Cohen-Mansfield et al. 18 examined unmet needs through the Unmet Needs Model developed earlier, focusing on the needs of older people with dementia. Exploring unmet spiritual needs of older people, Erichsen and Büssing 71 applied Alderfer’s Existence, Relatedness and Growth model, which is an extension from Maslow’s theory. Khandelwal et al. 87 compared unmet needs to inconsistent care. Martin et al. 55 and Wieczorowska-Tobis et al. 81 described the apparent imbalance between the assessed clinical needs of older people and the context in which optimal interventions were missed.
The unmet care needs of older people
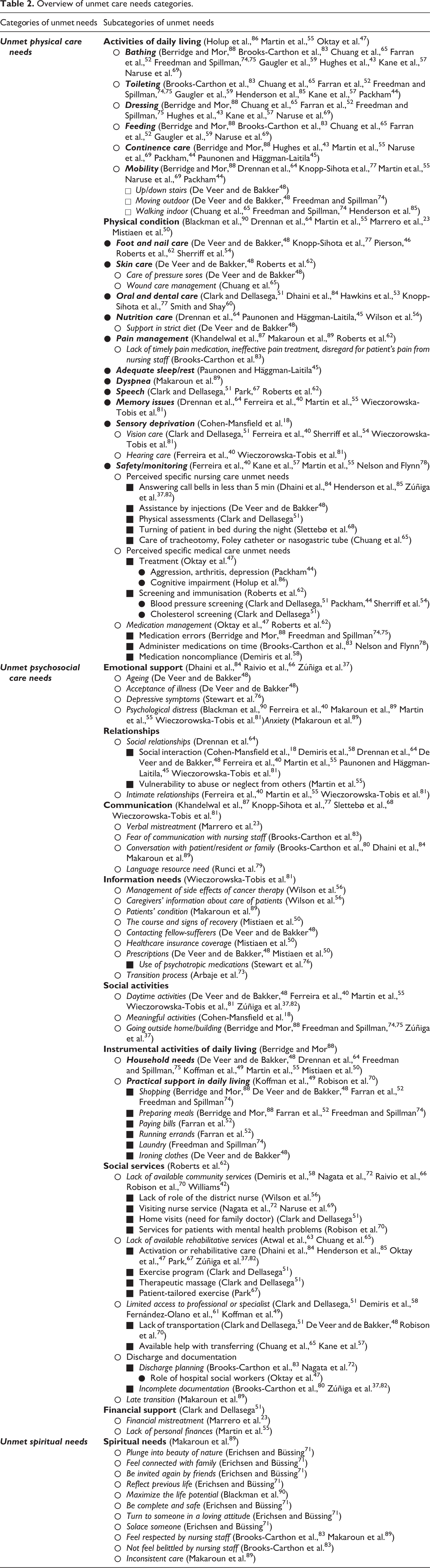
The majority of the studies concerned unmet care needs in three categories: physical, psychosocial and spiritual. The categorisation of different types of needs was adopted from the WHO International Classification of Functioning, Disability and Health Framework. 28
Unmet physical care needs included three main categories: ADL, physical condition, and safety and monitoring (Table 2). ADL included six sub-categories including bathing, toileting, dressing, feeding, continence care and mobility. The category of physical conditions included, for example, oral health, skin care or needs related to pain management. Safety and monitoring included unmet care needs, for example, related to medication. Unmet psychosocial care needs were organized into six main categories concerned with emotional support, relationships, IADL, social services, social activities, and communication and information needs. Macro-level reasoning was offered for some of these unmet care needs, such as the lack of available community nursing services or rehabilitative services or limited access to professional and/or specialist services. Finally, unmet spiritual needs were reported least and concerned, mostly religious-spiritual needs (Table 2).
Overview of unmet care needs categories.
The review found some context-specific assessments of unmet care needs reporting them to be common in traditional community housing and most prevalent in retirement, senior housing and assisted living settings. However, some authors found that unmet care needs are prevalent in all older people care settings. 74,75 The reasons for the unmet care needs included poor language-resourced and culturally bound care, not meeting the individual cultural differences, and were found less often in urban areas compared to rural areas. 79 Alongside this, minimal social interaction, due to the language barriers, was found to be associated with a sense of isolation. Negative outcomes due to unmet care, associated with harm, were reported by Gaugler et al. 59 who found that care recipients with dementia and associated increased unmet care needs were 1.77 times more likely to move from home to a nursing home and were 1.37 more likely to die than those with care needs that were met.
Raised ethical issues
Ethical issues related to the unmet care needs of older people were reported in some studies. Most of the ethical issues raised were related to the clinical prioritization of nursing care by tasks 37,68,82,84 associated with failing to carry out nursing care activities, 77,83,85 or shortcomings in providing good care for older people. 68,77 Several studies explored the consequences of failing to carry out nursing care in the context of falls, 23 urinary tract infections, 78 patient satisfaction, 50 or instrumental and daily living activities such as wet or soiled clothes, staying at home/inside the residential care facility, went without a hot meal/getting dressed/groceries/paying bills/clean laundry or eating, 74,75 raising questions about the respect of the ethical principle of non-maleficence. In other studies, patients complained (or indicated) that they were treated with disrespect 73,83,87 especially during the transition of older people 73 or at the end-of-life stage, 87 felt powerless or belittled, 83 felt ignored 63 or neglected 55,73 by nurses, had restricted autonomy in residential care settings, 44 or needed to use assertive self-advocacy to express their needs. 83 These results identify some poor experiences and demonstrate how strongly some people feel about this in their care. Some patients unable to speak for themselves and those having more comprehensive needs are even at risk of being neglected altogether. 68 In addition, the need to further support patients’ confidentiality, 56 self-esteem 71 and equal access to care 68 were highlighted in several studies. Another issue raised is the right to information from healthcare professionals in preparation for discharge; most of older people’s informational needs were concerned with the course and signs of recovery. However, some of the healthcare professionals did not even consider the possibilities (financial, self-care, mainly in housekeeping) of older people, so the information were often useless for them. 50 One study explored the role of nursing tasks delegation in the provision of care to residents. More qualified nurses often failed to instruct their less-qualified colleagues about proper care of the residents, but delegated some tasks on them (e.g. turning during the night shift) and omitted their responsibility for caring which often led to serious consequences for residents. 68
Two studies reported ageism as the main cause of unmet care needs. 53,68 In addition, Ferreira et al. 40 revealed that unmet care needs were associated with the worst patient outcomes and that the needs of institutionalized older patients often went under-diagnosed and thus untreated. Stewart et al. 76 found that the prevalence of depressive and challenging behaviour in older people was often treated with psychotropic medication rather than more social methods, which can be considered a sign of unmet care needs at the institutional level.
Another type of discrimination, regarding the unmet care needs of older people, was reported, based on race. 88 Black people were more likely to experience discrimination, unmet care needs and their consequences. 80,83 There is also evidence of nurses’ and other health professionals’ lack of recognition of the need for rehabilitation 63 neglecting the needs of those recovering from severe conditions and leading to, for example, prolonged immobilization. This suggests that the promotion of health, well-being and the support of independence was lacking, and this neglect may lead to harm through the loss of independence.
Discussion
Studies exploring unmet nursing care needs here include the point of view of patients, clients and individuals, while the missed nursing care literature is more often used in analysing omissions of care from the point of view of professionals. Although this scoping review includes limited empirical evidence, there is enough to demonstrate that the unmet nursing care needs of older people, including fundamental human needs, has been investigated from a number of perspectives and is significant. The review has revealed that it is not only missed care but also the quality of care 83 and the varied reasons for missed care that are also important. Although the quality of care is regulated in Europe and globally, for example, 8,12 the level of unmet care needs of older people is significant, occurring in many countries, in all care settings for older people. Thus, these significant and varied care issues are not local or even national phenomena, but a concern for nursing globally. The ethical issues that surround some of the unmet needs only add to the seriousness of these global nursing issues and may mean shortcomings in seeing the individual and in the person-centeredness of nursing care.
An examination of the concepts and terminology used in the reviewed studies with different approaches pointed to some systematic and some inconsistent use of the concepts. However, these different uses led to similar results. Of the three types of care needs categorized, physical, psychosocial and spiritual, the majority reported were omissions of physical care focused on ADL. This means that across a variety of different care settings, care provision is not always meeting the fundamental physical care needs of older people. Many older individuals have chronic conditions, affecting various parts of their body either locally, such as oral health and foot health, for example, 46,48,54,62,77 or systemically such as chronic lung and heart disease. Such unmet care needs may cause harm either directly or indirectly and are associated with a reduction of stable and healthy ageing at home or in a community. 13 Moreover, this finding warrants serious recognition. There is very strong ethical element and clinical care as physical unmet care needs have been found to be signs of undignified care. 91 Provision of adequate physical care is an ethical issue as is the non-provision.
The most obvious reason for unmet care needs is neglect, which is reported in several studies and is complex. This complexity may be concerned with the inadequate assessment of individuals’ needs prior to planning and care provision. 92 Many of the studies reviewed were carried out in non-hospital environments where the number of nursing staff is lower and the ratio of Registered Nurses to nursing assistants (e.g. licenced practical nurses) is less than that in a hospital context, 7 even though in many such settings, patient dependency levels can be quite high. Therefore, older people in non-hospital care settings are more likely to be cared for by people who do not have the education and competences required to assess old people’s needs sufficiently well. 93,94 However, this review focused on nurse professionals, not other workers such as social care or technical staff.
Given the variety of unmet nursing care needs (Table 2), closer investigation is needed. Based on the definitions of missed care, it is not just the work that is missed that needs to be considered, 10 but how the care assessment and plan are managed to completion also requires attention. The Institute of Medicine 11 and the WHO 8,13 have recognized the importance of including older people’s and patients’ perspectives in safeguarding older individuals’ health and well-being. Demonstrations of unmet care needs may be associated with the failure of nurses and other care assessors to follow this current advice and not facilitating older peoples’ participation in their care. 95 Some studies reviewed suggested this was because of the use of specific instruments to assess the older person’s condition and plan care that do not require interaction. 37,82 This lack of interaction is demonstrated in most of the studies reviewed, as older people’s needs are described from the researchers’ or health professionals’ frame of reference. A reduction of unmet care needs and inadequate care provision may be achieved by considering the older person’s perspective more thoroughly. This might have to take into account the generation difference between the older person and the care provider.
Age discrimination, ageism, has been reported in acute healthcare settings about older people, usually those with complex needs. These older people, requiring longer periods of recuperation and rehabilitation following an episode of ill health, are troublesome to staff working in a system with rapid turnover of patients. 96 In many societies, the lives of the older people are not considered of equal worth to the lives of younger people 97 and the allocation of resources is not needs-based but according to views on how beneficial people are to society. 98 Although this ageism is mainly observed at the macro level, the process influences nurses’ decision-making, for example, when rationing their time. 99,100 In addition, there are serious concerns suggesting that ageism was the main cause of unmet care needs 53,68,100,101 demonstrating outdated stereotypes for considering older individuals. 13 This type of ageism has been reported as counter-effective in cardiac care. Recently, it has been found that older individuals recover better from serious cardiac conditions if admitted to an Intensive Cardiac Unit (ICU) 102 with their condition(s) considered holistically. 103 Supporting the use of the ICU in this context, Levy et al. 97 found that reduction of ageism is cost-effective and improves the health of the ageing population.
Related to the concept of unmet nursing care needs is the extent needs are met under different circumstances. For example, some older persons are not assertive, and they do not or are not able to demand that their needs be met. 18 For those able to be assertive but are not, the relationship with the health professional is important. It has been reported that some older people think they are a burden and do not ask for what they want, being satisfied with what is done for them. 104
It can be argued that older people can improve their own health and have a responsibility to do what they can to age well. 94 However, not all older individuals have the options, capacity, abilities or knowledge to age well appropriately on their own and need assistance. 28,105 Where the capacity of older people falls below a level where they can look after themselves, the burden of some care requirements are frequently shared with unpaid family caregivers who provide significant care, including medical care and social support, to their loved ones. 66,103 Careful consideration is required about where the line is between informal caregiving and professional nursing practice with regard to knowledge, skill, attitudes and competence and the ethical management of care.
This review has raised implications for nursing care that calls for further research, particularly around the need for more transparent ethical stances in decision-making about the assessment planning and provision of care. This care should comply with the principles of care quality and meet the fundamental rights of older people demonstrating respect and equality. Serious concern exists if nursing care does not meet these fundamental values, especially if they lead to the neglect of older people.
Research into meeting the needs of older people is needed: at the macro level, for example, strategic resource allocation and population issues of access to healthcare 7,94 ; at the service level, the system level, within populations in care institutions and including political decisions. Research is also needed at the level of the individual where unmet needs might arise from, for example, professionals’ ability, competence, and implicit and explicit rationing, causing distress and poor health outcomes.
Strengths and limitations
The scoping review guidelines and search protocol were followed, which made the process transparent and strengthened the review. The review was further strengthened by the independent work of three researchers and discussion leading to consensus about the inclusion of citations for full-text screening. 106 As the nature of the scoping review is to describe the status of the research in a specific topic, a quality appraisal of the included research was not included in the review protocol. 98 Two databases were used, the most comprehensive regarding health and healthcare. 107 However, this could have left out some relevant research. Similarly, only studies completed in the English language were included, excluding any relevant studies in other languages. Although a variety of search terms were used increasing the possibility of finding the relevant empirical studies, studies including patients’ perspectives on missed care, which may have been reported in patient satisfaction and quality of care studies, were omitted from the review. The search of the literature was conducted using the variations of the search terms with Boolean operators, and the limited number of records was a surprise. However, we limited the search in general terms, not initiating any search from the different illnesses or health conditions, such as dementia, cancer and similar. As there is a variety of terms used for unmet care needs and missed care, more conceptual work is needed to redefine the concepts. Finally, there were no time limits in the search. The first study was from 1980. 42 The increased complexity of older people’s health and health problems may not be present in the earlier studies. However, early studies also revealed unmet care needs and were included in the review.
Conclusion
The results of this review suggest that unmet nursing care needs are varied and geographically widespread in terms of the three types of unmet needs: physical, psychosocial and spiritual. The nature and apparent frequency of unmet care needs raises consequential concerns for individuals, groups of individuals and the ethics of care, and sometimes seem to undermine modern active ageing and ageing in place policies. 13
Front-line healthcare professionals and their aides are not solely responsible for the unmet needs of older people found in this review, particularly when strategic decisions fail to support strategic policies. In the review, this discrepancy was demonstrated by regional health disparities and unequal access to nursing or other services after assessed needs. Further redefining the responsibilities of professionals and informal caregivers or family members is needed whether all unmet care needs are due to professional nursing or to others. However, it would be very difficult to identify which of the identified unmet nursing care needs, representing holistic human needs, are not properly the focus of nurse professionals.
Unmet care needs warrant further consideration as there are numerous unmet care needs ranging from the many basic needs to more complex needs. Moreover, the focus of the reviewed research has mainly been from the professionals’ perspective, with only a limited number of studies from the patients’ point of view. There is also evidence of unmet care needs associated with care rationing. The results also indicate that it is not only the unmet or met care needs but also the level of meeting those needs that should be considered. While being cared for in a healthcare setting, patients should be able to expect that care will be provided according to the best evidence-base available and will thus be of good quality. A further consideration is needed for those vulnerable patients, such as people with memory disorders, who are not able to express their needs and who may need an advocate to help them. Ageing in place and the next decade of healthy ageing 94 set demands for meeting the needs of older people. This requires comprehensive care assessment, planning and provision managed by carers with competence.
As care and access to healthcare services are fundamental rights of human beings, unmet care needs raise serious ethical concerns which should be studied and highlighted in decision-making regarding resource allocation. These matters should also be acknowledged in policy development regarding the healthcare and health service provision for older people.
Footnotes
Acknowledgements
On behalf of the *RANCARE Consortium COST Action – CA 15208:
Acaroglu Rengin (Istanbul University, Turkey); Andreou Panayiota (Cyprus, Cyprus University of Technology); Antonic Darijana (Bosnia & Herzegoviva, Public Health Institute, Banja Luka, Republic of Srpska); Ausserhofer Dietmar (Italy, Landesfachhochschule fur GesundheitsberufeClaudiana); Baret Christophe (France, CNRS, LEST); Bosch-Leertouwer Helen (Netherlands, Windesheim University of Applied Sciences); Bragadottir Helga (Iceland, University of Iceland); Bruyneel Luk (Belgium, KatholiekeUniversiteit Leuven); Christiansen Karin (Denmark, VIA University College); Čiutienė Rūta (Lithuania, Kaunas University of Technology); Cordeiro Raul (Portugal, Instituto Politecnico de Portalegre); Deklava Liana (Latvia, Riga Stradins University); Dhaini Suzanne (Lebanon, American University of Beirut); Drach-Zahavy Anat (Israel, University of Haifa); Eftathiou Georgios (Cyprus, Cyprus University of Technology); Ezra Sigal (Israel, Sheba Hospital, Sheba Medical Centre); Pilan Fuster (Spain, UniversitatInternacional de Catalunya); Gotlib Joanna (Poland, Medical University of Warsaw); Gurkova Elena (Slovakia, University of Presov); Habermann Monika (Germany, Hochschule Bremen Neustadtswall); Halovsen Kristin (Norway, Oslo and Akershus University College Applied Sciences); Hamilton Patti (United States, Texas Woman’s University); Harvey Clare (Australia, CQUniversity Australia); Hinno Saima (Estonia, Tartu Health Care College); Hjaltadottir Ingibjorg (Iceland, University of Iceland); Jarosova Darja (Czech Republic, University of Ostrava); Jones Terry (United States, The University of Texas at Austin); Kane Raphaela (United Kingdom, Liverpool John Moore University); Kirwan Marcia (Ireland, Dublin City University, School of Nursing and Human Sciences); Leino-Kilpi Helena (Finland, University of Turku); Leppée Marcel (Croatia, Institute for Healthy Ageing, Slovenska); Amorim Lopes Mario (Portugal, INESC-TEC); Millere Inga (Latvia, Riga Stradins University); Ozsaban Aysel (Turkey, Istanbul University); Palese Alvisa, (Italy, Udine University); Patiraki Elisabeth (Greece, University of Athens); Pavloska Katina (FYR Macedonia, Institute for mental health for children and youth); Phelan Amanda (Ireland, University College Dublin, School of Nursing, Midwifery & Health Systems); Postolache Paraschiva (Romania, ‘Grigore T. Popa’ University of Medicine and Pharmacy of Iasi); Prga Ivana (Croatia, Andrija Stampar Teaching Institute of Public Health); Rasch Agripina (Romania, University of Medicine and Pharmacy Carol Davila); Rengel Diaz Cristobal (Spain, Hospital Universitario Virgen de la Victoria de Malaga, Campus Universitario de Teatinos); Rochefort Christian (Canada, University of Sheebrook); Scott Anne (Ireland, National University of Ireland, Galway); Simon Michael (Switzerland, University of Basel); Stemmer Renate (Germany, Catholic University of Applied Sciences Mainz); Tichelaar Erna (Netherlands, Windesheim University of Applied Sciences); Toffoli Luisa (Australia, University of South Australia); Tonnessen Siri (Norway, University College of Southeast Norway); Uchmanowicz Izabella (Poland, Wroclaw Medical University); Vuckovic Jasminka (Bosnia & Herzegovina, Ministry of Health and Social Welfare Republic of Srpska); Willis Eileen (Australia, Flinders University); Xiao Lily (Australia, Flinders University); Zeleníková Renáta (Czech Republic, University of Ostrava); Zorcec Tatjana (FYR Macedonia, University Children’s Hospital Faculty of Medicine University of Skopje).
Author contributions
The conception and design of the study were performed by D.K., R.S., M.S., P.A.S. and EP; acquisition of data was done by D.K., R.S. and M.S.; analysis and interpretation of data were performed by D.K., R.S., M.S., P.A.S. and EP; the article was drafted by D.K., R.S. and MS; and revising it critically for important intellectual content was performed by D.K., R.S., M.S., P.A.S. and EP.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.