
Abstract
Background:
Identifying and safeguarding ethics in eHealth services from the service users’ perspective in social care and healthcare is important. The use of eHealth services should not prejudice the quality of services or the social interaction required in care. There is a lack of studies about the ethics of eHealth services from the service users’ perspective.
Aim:
The aim of this study is to identify and analyse ethical issues related to eHealth in social care and healthcare from the service users’ perspective.
Research design:
An integrative literature review.
Ethical considerations:
The review followed good scientific conduct.
Research context and data sources:
A systematic literature search was performed using CINAHL, Scopus, PubMed/MEDLINE, Web of Science, Cochrane Library and Academic Search Premier to find relevant empirical studies published in English from their earliest up to 30 November 2018. In addition, reference lists from the identified research papers were searched. A quality appraisal of each paper included in the review was conducted before thematic analysis.
Results:
In total, 26 studies were included in the review, and from these four ethical themes were identified: (1) privacy in eHealth, (2) beneficence and nonmaleficence in eHealth, (3) justice in eHealth and (4) trust in eHealth. The ethical issues within these themes were related to information sharing; ownership; access to information and data protection; informed consent; defence of rights; and equity, equality and proportionality of response.
Conclusion:
eHealth inequality occurs in social care and healthcare. eHealth service designers and social care and healthcare professionals need to act to maintain and improve user access and data accuracy and provide different levels of security in eHealth services, relative to the information stored. There is a need for further research about ethical issues of eHealth from the user’s perspective, including the customer-oriented availability and usability of eHealth services which avoid discrimination.
Introduction
Identifying and safeguarding ethics in eHealth services from the service users’ perspective in social care and healthcare is important. The use of eHealth services should not prejudice the quality of services or the social interaction required in care. The Organisation for Economic Co-operation and Development (OECD) suggests that efforts and continuous research are needed to improve and expand our knowledge about the provision of equal and secure digital opportunities for all. 1 As part of this improvement and expansion, it is necessary to evaluate the advantages, disadvantages, risks and consequences of eHealth services for the individual and the community in a fair and equal society. 2 –4 The service users’ perspective on the ethical issues concerned with the development of eHealth services is an important part of this evaluation. 5 –8 Any evaluation should pay particular attention to data protection issues and the ability of the citizen to access digital systems. 9 This improvement and expansion of eHealth services must not undermine the quality of services, social interaction and human factors. 3,4,9
Digitalization is a global phenomenon, and the use of digital technology affects both professional and private lives. 10,11 In developing countries such as sub-Saharan Africa, 45% of the population use the Internet, compared with 83% in developed countries such as North America; overall, this amounts to 67% worldwide. 12 In the Nordic countries, such as in Finland, 75% of people aged 65–74 years and 37% of those aged 75–89 years used the Internet and eHealth. 13 To develop a wider use of the Internet, the European Commission’s long-term (2021–2027) programme, Digital Europe, aims to guide European digitalization for the benefit of citizens and businesses at a planned cost of €9.2 billion. 14
Currently, there are three levels of eHealth services: (1) general online services provide advice, information, tests and guidelines on healthcare and social services; (2) various appointment services for social care and healthcare, tracking personal information and viewing options; and (3) digitized services include various video conferencing and remote services used, for example, in education, diagnosis and the provision of treatment options. 15 –18 There are worldwide actions to improve the health of citizens by improving access to digitalized health information. For example, the European Commission and the World Health Organization aim to develop new opportunities to better meet the needs of users and to promote and harmonize the use of eHealth technology at individual and organizational levels. 9,16,19
Studies have shown that more attention to ethics and risk management should be considered. 20,21 Earlier studies have found varying and disparate use of eHealth in specific areas of health, for example, in telehealth, 21 –23 in mental health and eHealth technologies, 24 –26 and in varying diagnoses such as urinary incontinence and diabetes. 27,28 However, the user perspective concerned with, for example, which health technology and services are needed, along with their acceptability and feasibility, has rarely been investigated.
Ethical issues of eHealth
Citizens provide information which is collected and stored digitally for use within eHealth services. This information is subject to human rights legislation. 29 Human rights treaties are international treaties which, when ratified and adopted by an individual state, that state undertakes to secure the rights and obligations specified in the treaty for the people. 29 The European Union Agency for Fundamental Rights and the Finnish Constitution advocate the human rights to privacy: ‘Everyone has the right to life and to personal freedom, integrity and security’. 2,30 Similarly, the Status and Rights of Patients Act 31 stipulates that the information contained in patient records is confidential. Patients are equal before the law and have the right to good health and medical care, as well as to humane treatment and the right to information and self-determination. 5,31
Ethical issues that may affect human rights occur in the intersection between the technology used to provide eHealth services and the use of the information stored, as both the eHealth services and users adapt over time. 3,4 These ethical issues may compromise the rights of individuals and organizations, and ways to reduce this need to be found. 3,32 The areas of intersection between the technology used and the information stored where analysis may be important include trust, privacy and related data protection, ownership, dignity, and equity and proportionality of response. 3,32 In addition, respect for life, the intention to do good, doing good, avoiding harm and providing justice are important overall ethical principles of nursing 33,34 that should be considered when planning and implementing eHealth technology. 9,19 These principles lead to, for example, facilitating patient’s self-determination and the dignity of life. 33,34 The Human/Technology Adaptation Fit Theory for Healthcare Model 35 focuses on this intersection between technology adaptation and user adaptation in the context of voluntary or mandatory digital health information. Both researchers and practitioners can use this model to determine the effects of the implementation of new technologies. 9,35
Ethical principles include trust, privacy and related data protection, property rights, dignity, fairness and proportionality. Trust must be present in eHealth in such a way that citizens need to be reassured that data are being processed properly, that they are up-to-date and of quality, and that security risks are being taken into account. 3 The success of eHealth will have a positive impact on confidence. 36 Healthcare professionals are also aware that personal contact is required. 37,38 Privacy allows citizens to choose what information they want to share about themselves. 6 –8 Equity must be made possible in the implementation of eHealth. 3 Equality in eHealth does not apply to the older people, the low-educated, those out of work and those living in rural areas. 39 People with a lower level of education use digital services less than those with a higher level of education. 40,41 Research of ethical issues from the user’s perspective is fragmented, especially the use of eHealth, thus warranting further research. 20,21,40 Previous research has focused on the experiences of eHealth users, including different implementations of eHealth in healthcare, 24 –26 professional opinions 37,42 and digital applications for various diagnoses. 27,28,43 However, ethical issues from a user perspective in eHealth have rarely been explored. It has been shown that the implementation of eHealth requires earlier design stages 24 and the identification of necessary research. 25,26 The successful use of eHealth in health promotion programmes depends on the motivation and support that people can receive. 27,28,44
The current health literature is limited regarding eHealth ethical issues, especially from the service users’ and citizens’ perspective. 20,21 This is an important gap in ethics research given the wide use and planned increases in the adoption of eHealth technology discussed earlier. The aim of this current review is to find out more about this gap.
Aim
The aim of this integrative review was to identify and analyse the ethical issues related to eHealth in social care and healthcare from the service users’ perspective. The associated research question is: What are the ethical issues of eHealth in social care and healthcare from the service users’ perspective?
Methods
The review was conducted after Whittemore and Knafl’s 45 five-phase process for conducting an integrated review: (1) problem identification, (2) literature search, (3) data evaluation, (4) analysis and synthesis, and (5) presentation of results.
Literature search
A systematic literature search was conducted using six relevant international databases – CINAHL, Scopus, PubMed/MEDLINE, Web of Science, Cochrane Library and Academic Search Premier – searching entire databases from their earliest, without time limit, up to 30 November 2018. The following keywords and database-specific headings (MeSH or CINAHL headings) were employed in every database combined with Boolean operators: Telemedicine; Electronic Health Records; Medical Records Systems; ehealth; e-health; mhealth; Computerized Patient Medical Records; Electronic Medical Records; Ethics; Moral; Ethical; customer, citizen. Two co-researchers (M.S. and R.S.) checked the usefulness of the database search.
The inclusion criteria were the following: (1) peer-reviewed empirical studies in international scientific journals written in English; (2) ethical issues of using eHealth in social care and healthcare related to the user perspective; (3) ethical issues related to the use of systems, guidance and care services; (4) experiences of service users, their use of eHealth and the ethical issues that occur; and (5) all empirical research designs where results describe patient experience and observations. The exclusion criteria were the following: (1) editorials, case reports and opinions; (2) the use of non-medical and socially digitalized services and related ethical issues, such as digitalized banking services and commercial services; and (3) the experiences of nursing staff or service providers about the content of eHealth services, their need, product development and research conducted. The database searches identified records (n = 5737) which were selected by one author in three steps. First, duplicates (n = 1800) were removed and the title and abstract of the remaining papers (n = 3937) were considered against the inclusion and exclusion criteria, leading to the inclusion of 47 papers. Finally, the full text of these 47 articles was assessed, resulting in 17 studies which were included in the review. The reference lists of these included studies were then searched manually for relevant papers. Nine relevant papers were found, and so twenty-six studies were included in the review (Figure 1).
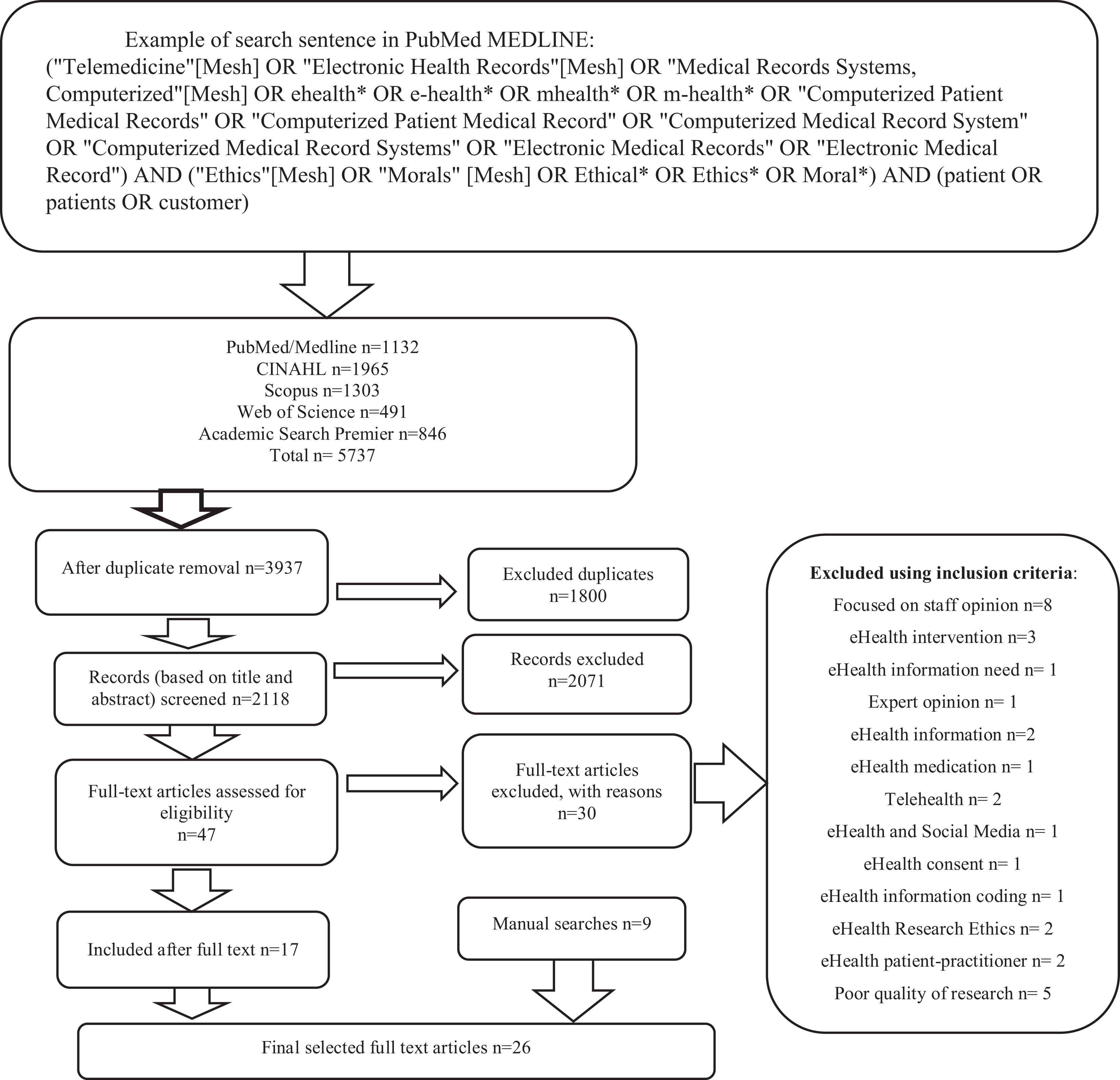
Flowchart of the literature searches.
Data evaluation
Studies (n = 26) were critically appraised using standardized study design–specific checklists. 45 The quality of individual articles was evaluated using quality assessment criteria designed for both qualitative and quantitative studies. 46 This evaluation considered mainly purpose, methods, data collection, data analysis and conclusions. 47
Data were extracted to a table including information about author, year, country, aim, design, sample, data collection method and results (Table 1). 46,48
Description of the included studies.
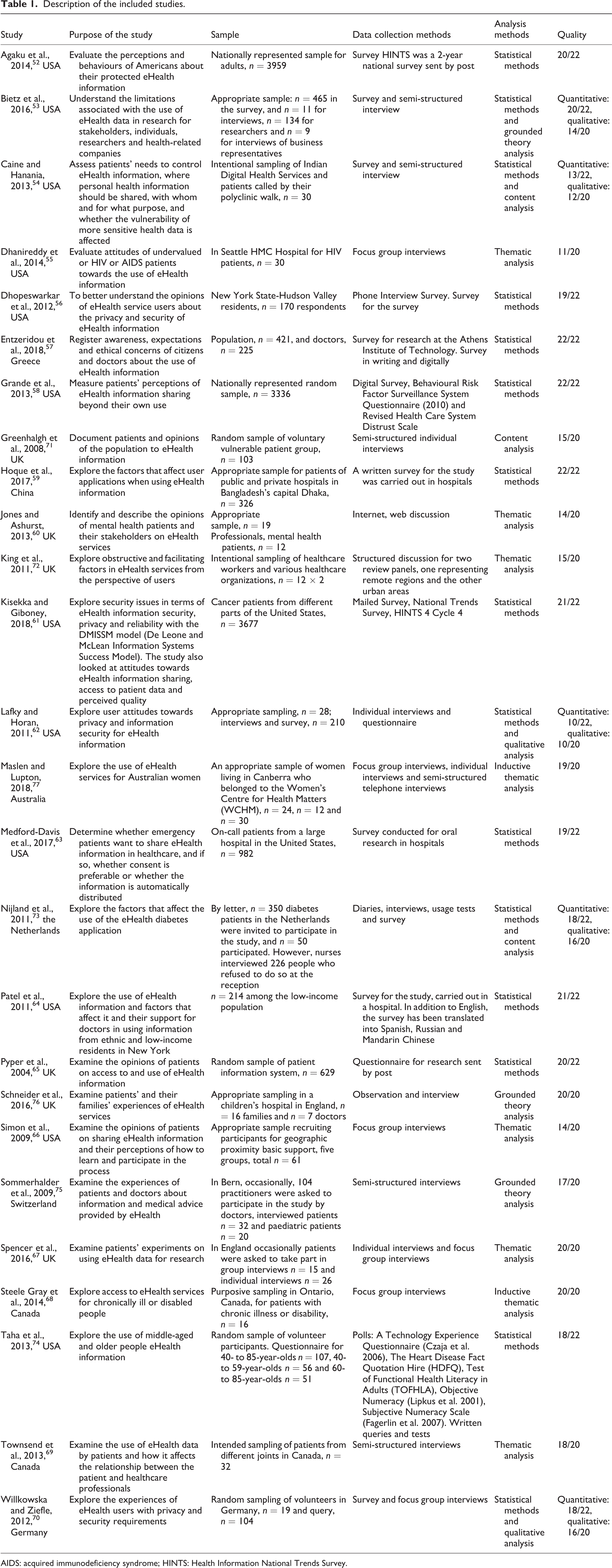
AIDS: acquired immunodeficiency syndrome; HINTS: Health Information National Trends Survey.
Data analysis and synthesis
The data were thematically analysed. 49,50 The text concerned with ethical issues related to eHealth and retrieved from the studies was coded using the author’s original words to increase authenticity, and no interpretations were done; the text was investigated inductively guided by the research question. Words were tabulated, combined and reduced, retaining the original quality of the comments. Words were grouped into notes; they were given a code, and a group of codes were highlighted with the same meaning and organized into subthemes, which were merged into main themes during synthesis. 45,51
Results
Study characteristics
The 26 articles were published between 2004 and 2018 and conducted in many countries: the United States (n = 12), the United Kingdom (n = 6), Canada (n = 2), Greece (n = 1), China (n = 1), Australia (n = 1), Switzerland (n = 1), the Netherlands (n = 1) and Germany (n = 1) (Table 1).
The methodological approaches of the studies were quantitative (n = 10), qualitative (n = 11) and mixed methods (n = 5). All the quantitative studies used descriptive survey questionnaires (n = 10). Some of these questionnaires were developed for the individual studies or validated instruments (n = 4). The qualitative study data were collected by interview. Descriptive survey studies and interviews were also used in the mixed methods papers, and one of these studies also used diaries and quizzes.
The quality of the included studies was good, the scores being 20.3/22 (range 4,0) for quantitative studies, 16.6/20 (range 9,0) for qualitative studies and 15.8/22 (range, 12,0) for mixed methods studies. The most common weaknesses were in the research analysis section.
Ethical issues related to eHealth in social care and healthcare from the users’ perspective
Thematic analysis of the studies led to the identification of four themes: Privacy in eHealth, Beneficence and Nonmaleficence in eHealth, Justice in eHealth and Trust in eHealth. These themes contained 11 sub-themes related to the ethical issues in eHealth services of social care and healthcare.
Theme 1: Privacy in eHealth
The theme Privacy in eHealth was found in 22 of the 26 papers through the following sub-themes: data sharing, ownership, access to data and safety, and informed consent (Figure 2).
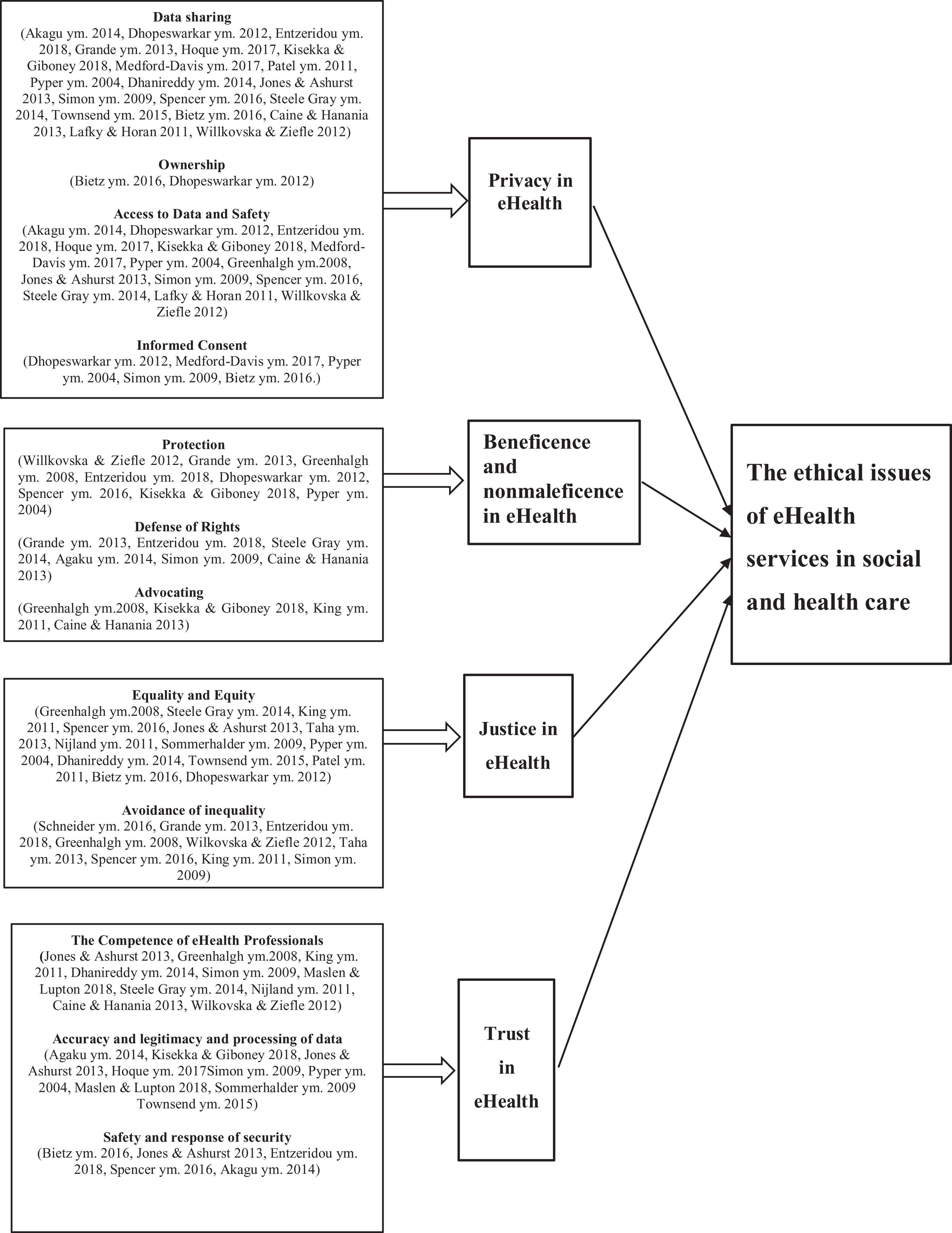
Summary of results.
Data sharing
Data sharing and privacy of eHealth data within services were a concern for citizens in 19 papers. 52 –58,59,60,61,62,63,64,65,66,67,68,69,70 It was important that privacy was protected by choosing with whom the information would be shared. 56,65,66,67,69 However, information was shared more willingly person-to-person, in the conduct of research 58,67 and with the citizen’s own physician. 54,56,61,63,64 Those people with long-term conditions, those severely ill and those with emergency health problems were more willing to share their health information because they benefitted from the discussion. 62 Many citizens were more willing to share their eHealth information if privacy, anonymity and confidentiality were guaranteed. 53 Citizens emphasized the need to respect the rights of individuals when sharing information. 56
Ownership
Perceptions about health information ownership varied. Usually, citizens thought they owned their own health information. 54,57
Access to data and safety
Data security in eHealth services was a concern in several studies. 52,56 –59,61,62,63,65,66,67,68,70 In particular, the transfer of analogue healthcare information to eHealth information caused concern about data protection. 52 Many citizens wanted to avoid access to their eHealth records by third parties. 56,57,67,68
Informed consent
Some citizens only wanted to share information after giving informed consent, which gave them control over what was being shared and with whom. 53,56,63,68
Theme 2: Beneficence and Non-maleficence in eHealth
Beneficence and nonmaleficence mean doing good and avoiding harm, 3 and within this review they include the sub-themes protection, defence of rights and advocation (Figure 2). Mostly, citizens believed that eHealth services were more beneficial than harmful, 57,65,66,67 as eHealth information and services facilitated a more active involvement in their own care, empowered by experience. 55,58,71,72,73,76,75
Protection
Major concerns were caused by worries about third-party access to protected eHealth data, either intentional or unintentional. 56,71,67 Citizens in the study feared the possibility that false information added to their records would lead to poor medical decisions by healthcare personnel and consequential patient harm. 61
Defence of rights
Citizens were concerned that the misuse of personal and normally protected data might lead to social isolation, 68 stigma, discrimination or rejection at work 56 if the information was used for harmful purposes by others. 57,58 Particularly worrying was that sensitive data, for example, sexually transmitted diseases, mental health diagnoses or drug use, might be made public, causing problems for the individuals concerned. 52,54,66
Advocation
Citizens expressed concern that the lack of data protection, errors in transferring personal information or a mix-up of identities could jeopardize patient care. 71,61 Different patient groups and varying illnesses lead to different needs within eHealth services, which should be taken into account in the development of eHealth services. 72 Some citizens also feared that they would receive a lower level of care if eHealth data, showing the use of intoxicants, were available to others without advocating in their interests. 54 Sometimes information is shared wrongly or against the citizen’s wishes. 53,60
Theme 3: Justice in eHealth
The sub-themes were equality and equity and the avoidance of inequality (Figure 2).
Equality and equity
Equality and equity in this context mean that everyone has equal opportunity of access to similar services. 32 However, the equitable use of eHealth services was perceived to be difficult in circumstances where there was no or intermittent Internet connection, 71,72,73,68 Internet skills were poor, 60,72,67,68,74 mental capacity was reduced, 72,75,74 numerical skills were low 74 or the eHealth services being used were difficult to understand. 55,65 Some older people found it difficult to use eHealth services, 73,65,74 while others just did not want to use them. 71,60,69 Although updating information technology is costly, 65 it has been suggested that anyone who cannot afford to buy a suitable device should still be able to use the Internet if they wished. 73
Avoidance of inequality
Avoidance of inequality is concerned with achieving justice. Citizens were concerned about possible inequality in their treatment and care if they were unsure how to use the Internet or eHealth services. 72,67 The consequences discussed were about doing something wrong, 76 experiencing discrimination 57 or stigmatization. 57 –71,70
Theme 4: Trust in eHealth
Trust in eHealth consisted of three sub-themes: the competence of healthcare professionals; the accuracy, legitimacy and processing of data; and safety and response of security (Figure 2).
Competence of eHealth professionals
Success in eHealth systems had a positive effect on trust. 59,61,66 Surveys revealed that citizens wanted competent professional support with eHealth services 60 and human contact to help them address health issues. 71 Citizens wanted digital services to improve caring, not to replace personal contact, 60,72 which they feared. 58
Accuracy, legitimacy and processing of data
Concerns about accuracy, legitimacy and processing of data were considered in terms of confidentiality and the integrity of eHealth data. 52,60,61 Concerns were caused by the possible use of inadequate or incorrect information in healthcare, 61,65 the inaccurate transfer of eHealth data between different healthcare organizations, 52 poor quality of eHealth data 77 and diversity of data, and inconsistency and complexity with so many different systems and solutions. 75,69
Safety and response of security
Information security had to be addressed proportionally, with the information secured requiring agreed standards and rules to protect the security of eHealth data 53,60 and to ensure safe, accurate data retention. 57 Citizens expressed confidence in eHealth services and the social responsibility taken with their personal data. 67
Discussion
This review explores the service users’ perspective of the ethical issues surrounding eHealth services found in the social care and healthcare literature. An extensive database-led literature search found very little empirical research on the subject, which suggests there may be more research to be done in this fast-moving area of healthcare. Four main themes were identified: privacy in eHealth, beneficence and nonmaleficence in eHealth, justice in eHealth and trust in eHealth.
Privacy in eHealth
The results of the review highlighted that health information sharing facilitates access to information, decision-making, 57,77,65,66,68,70 and access to treatment. 72,73,68 This finding concurs with the aim of the European Commission to improve the health of citizens by enhancing the quality and accessibility of eHealth tools to make them more efficient, user-friendly and more widely accepted. 12 However, in this review, the most critical ethical issue in the use of eHealth services was concerned with sharing information. Citizens raised concerns about maintaining privacy when sharing and transmitting health information. Patients wanted to decide for themselves how and with whom to share their health information, 56,65,66,67,69 which, according to the ethical principles of The European Health Telematics Association (EHTEL), is their right. 3 Two studies suggested that more attention to ethics and risk management should be considered. 20,21
In this review, healthy citizens were more interested in eHealth services than those with poor health, and women wanted more security in eHealth systems than men. 62 People with poor health and long-term illnesses agreed to share eHealth information more readily, considering that this would make access to healthcare services faster and easier. 71,73,70 Many citizens wanted the right to give informed consent for sharing personal data, which would increase trust in eHealth services. Being able to give informed consent assumes the patient owns their eHealth information. 3 Since the same information may be held on several data files, for example, occupational therapy, nursing and medical files, it may be difficult for an individual patient to control access to these files through conventional informed consent procedures. It remains to be seen what information about citizens will be shared without this type of data protection. 53,56
Beneficence and nonmaleficence in eHealth
eHealth information and services facilitated a more active involvement in their own care, empowered by experience, 55,58,71,72,73,76,75 which supports the aim of the European Commission 2 and the Finnish Ministry of Social Affairs and Health 15 to improve citizens’ health and interest in their own care by improving the availability of health information.
Citizens sought protection from situations where disclosure of eHealth information might lead to discrimination, 57,58 unwarranted access to protected health information by third parties 56,71,67 or a similar disclosure of sensitive information. 52,54,66
Healthcare professionals normally advocate for their patients providing this protection to reduce the risk of harm to the patient, 33,34 and the need for this protection has been acknowledged in previous studies. 1,6,7 However, there may be times when information is shared wrongly or against the citizen’s wish. 53,58 According to the European Union Agency for Fundamental Rights 2 and the Finnish Constitution, 30 every citizen has the right to life as well as to personal freedom, integrity and security, which needs to be realized even if sensitive information is used in eHealth services.
Justice in eHealth
Justice in eHealth is concerned with the way equality and equity in eHealth are managed across healthcare populations. 2,30 According to Statistics Finland, only 19% of 75- to 89-year-olds had accessed information on the websites of public authorities or public service providers, while 35% of this age group had used the Internet for banking purposes. 13 When citizens do not use appropriate eHealth websites, injustice can occur in, for example, access to services. This current review showed that justice was hampered by poor Internet access, poor Internet skills, cognitive skills and numerical skills, or difficulty understanding the digital services provided. Other challenges include age-related access difficulties, 13,73,65,74 a reluctance to use digital services and the costs associated with digital devices and Internet access. 73,65
These issues present challenges to eHealth services and also challenge the implementation of the Anti-Discrimination Act (1977) and the Charter of Fundamental Rights of the European Union. 2,3 This Act and Charter obliges society to organize digital services so that they are accessible to everyone. It is one’s choice not to use digital services, but the goal is to find ways to make digital services available to anyone who wants it. Social care and healthcare organizations need to embrace these challenges because without some assistance a significant minority of people may not, for example, book an appointment which could lead to the unequal treatment of citizens. There is a moral obligation in society 4,31 to avoid inequalities where possible, 2,30 although it is acknowledged that a lack of education and, in some cases, a lack of physical and intellectual skill complicate the use of digital services, leading to inequalities. 72,65,75,74
Trust in eHealth
Citizens reported concerns about the competence of healthcare professionals in terms of accuracy, legitimacy, safety, data processing and the proportional response to the security of data. Surveys revealed that citizens wanted competent professional support 60 and human contact to address health issues. 71 They wanted eHealth services to improve caring, not to replace personal contact, 60,72 consistent with previous studies. 1,7 Many objected to digital services because they feared that social contact would decline or end. 55,71,60,72
Transparent standards and rules are required to protect eHealth security. 35 Overall, it is necessary to assess the benefits, drawbacks, risks and consequences of the use of technology for the individual and the community. 33,34 Human privacy and integrity must be respected and individuals must also be able to refuse to use technology. The Human/Technology Adaptation Fit Theory for Healthcare model could be used to help citizens and professionals understand the privacy rules, to take steps to protect their data and to demand or organize a higher level of data protection from healthcare providers where necessary.
The review also revealed positive feedback on the use of digital services by service users for information purposes. The provision of health information digitally led to a better understanding of the citizen’s own health and its determinants. 55,60,77,64,65 –75 In turn, this made it easier for individuals to talk about personal health with their physician, including understanding the physician more clearly 77,65,75,69 and demonstrating an increased commitment to treatment. 75 It has been suggested that a new professional role of patient consultant could act between physicians and eHealth service users when they want to question significant issues captured in eHealth information. 72,61
Digital inequalities occur in social care and healthcare and have varying causes. The results of the review highlight the need for further research on how these inequalities have an impact on the treatment and care of individuals. 1,6,7
Strengths and limitations of review
The data selection process was undertaken by the first author (A.J.) and discussed and verified in the research group (M.S. and R.S.). Based on database and manual searches, the quality of the studies discovered was evaluated using a systematic evaluation tool, 47 which helped to reduce bias and misconceptions. 46 The surveys represented citizens’ opinions from a number of different nationalities and countries, including developing countries. The responses may include the effects of cultural differences and the spontaneous bias of some respondents during data collection. The study followed good scientific practice, including honesty and care with accuracy throughout the research process. The work of the other researchers was treated with respect in accordance with the reference practices. 78
There are some limitations which need to be taken into consideration when interpreting the results of this review. Despite an extensive literature search based on relevant databases and a manual search of reference lists, very little empirical research was found. There may be some studies published in other languages, and others, not published in international scientific journals, though relevant to this review, were excluded.
Conclusion
This review provides a new insight into the ethical issues in eHealth services and highlights their importance in the development of technological and digitalized services. Users of digital services require an ever-increasing skill-set, usable equipment and a functional Internet connection. The independent use of eHealth services requires users to be proactive and eager to become familiar with the services provided. Social care and healthcare professionals need to be trained to guide citizens in the use of digital services in a customer-oriented way.
Digital inequalities which, for example, reduce digital access opportunities and increase discrimination were found to occur in social care and healthcare. This type of inequality is a cause for concern in a just and equal society, and ways to maintain and improve the application of justice in eHealth need to be considered.
The information generated in this study can be used in developing digital services, to make sure relevant ethical issues are considered in eHealth service design and implementation from a service users’ perspective. Further research on the experiences of users of digital services and the availability and usability of digital services would be useful prior to empirical research on how digital eHealth services could be developed in the future.
Footnotes
Acknowledgements
We wish to thank Professor Elina Haavisto for her valuable comments regarding the earlier version of the manuscript. The language was edited by Dr Norman Rickard, RN, PhD, and is gratefully acknowledged.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.