
Abstract
Objective
Equitable elimination of cervical cancer in Australia within the next decade will require high National Cervical Screening Program (NCSP) participation by all subgroups of women. The aim of this study was to examine the participation of immigrants compared to Australian-born women.
Methods
Participation in the NCSP (≥1cytology test) over a 3-year (2010–2012) and 5-year (2008–2012) period, by place of birth and time since immigration was examined using individually linked data of 67,350 New South Wales (NSW) women aged ≥45 enrolled in the 45 and Up Study.
Results
Three-year cervical screening participation was 77.0% overall. Compared to Australian-born women (77.8%), 3-year participation was lower for women born in New Zealand (adjusted odds ratio 0.77, 95% confidence interval 0.69–0.87), Oceania (0.67, 0.51–0.89), Middle East/North Africa (0.76, 0.60–0.97), South-East Asia (0.72, 0.60–0.87), Chinese Asia (0.82, 0.69–0.97), Japan/South Korea (0.68, 0.50–0.94), and Southern/Central Asia (0.54, 0.43–0.67), but higher for women from Malta (2.85, 1.77–4.58) and South America (1.33, 1.01–1.75). Non-English-speaking-at-home women were less likely to be screened than English-speaking-at-home women (0.85, 0.78–0.93). Participation increased with years lived in Australia but remained lower in immigrant groups compared to Australian-born women, even after ≥20 years living in Australia. Similar results were observed for 5-year participation.
Conclusions
Women born in New Zealand, Oceania, and parts of Asia and the Middle East had lower NCSP participation, which persisted for ≥20 years post-immigration. The NCSP transition to primary HPV screening, and the introduction of the universal self-collection option in 2022, will offer new opportunities for increasing screening participation for these groups.
Introduction
In 1991, Australia introduced the National Cervical Screening Program (NCSP), recommending 2-yearly conventional cytology for asymptomatic women and people with a cervix aged 20–69 (the pre-renewed NCSP). In December 2017, the NCSP changed to 5-yearly primary human papillomavirus (HPV) testing for women aged 25–69, with HPV 16/18 genotyping and cytology triage for non-16/18 HPV types, and an exit test for women aged 70–74 (renewed NCSP). With the introduction of the renewed NCSP, women aged ≥30 who were ≥2 years overdue for screening were eligible for HPV screening on a self-collected vaginal sample (self-collection). Since July 2022, all women eligible for cervical screening have had the option of self-collection.1,2
After the introduction of the NCSP, cervical cancer incidence and mortality in Australia halved between 1991 and 2002, with 9–10 new cases diagnosed, and two deaths, per 100,000 women each year. However, since 2002 incidence and mortality rates have remained steady.3,4 It is estimated that in 2015–2016, around 55% of women aged 20–69 participated in the NCSP nationally, with lower participation for women in the lowest socio-economic groups and those living in very remote areas. 5
Participation has been shown to be lower among some immigrant sub-groups. 6 In a recent review of studies covering the mid-1980s to early-2000s, South-Asian-born women consistently had the lowest screening rates compared to Australian-born women. 6 Included studies were mostly limited to immigrants from a small range of countries and many were surveys. The two most recent data linkage studies, which included NSW women admitted to hospital or giving birth in 2000–2001 (with Pap Test Register records until 2006), found that older women born in South Central Asia 7 and younger immigrant women from Asian and Middle-Eastern countries 8 were less likely to be screened for cervical cancer at the recommended interval than Australian-born women. Pap test rates for women living in areas with higher proportions of women from non-English-speaking backgrounds were lower than for women from areas with lower proportions. 6 Higher Pap test rates were seen among women who had lived in Australia for longer. 6
The proportion of Australia's population born overseas increased from 23.0% in 2000 to 29.8% in 2020. 9 The predominant countries of origin of immigrants have changed over time. After World War II immigrants were mainly from North-West Europe, and later Southern and Eastern Europe, with arrivals in the 1970s from South-East Asia, and more recently also from other Asian countries. 10 In 2011, of the overseas-born population (26% of the population), 21% were born in the United Kingdom, 9% in New Zealand and 6% in each of China and India. 10
Australia is on track to eliminate cervical cancer (defined as achieving a population average of <4 new cases per 100,000 women annually) between 2028 and 2035. 11 Cervical screening is the driver of the timing of cervical cancer elimination in the short and medium term. 12 Ensuring screening of underserved groups, including gender and sexually diverse people, Indigenous, and culturally and linguistically diverse (CALD) women, is vital to achieving equitable outcomes in all groups of women and people with a cervix in Australia. However, women from CALD backgrounds are heterogeneous, and understanding differences in screening rates and in socio-demographic factors between these groups is important to ensure the targeting of screening programmes. Analysis of linked data offers the opportunity to understand historical screening rates in these groups of women. There has not been a recent comprehensive analysis covering women from all geographical regions and which also considers time since immigration.
In this study we update and expand on previous studies, by examining the participation of immigrant women in the NCSP compared to Australian-born women up to 2012, including women from all the major regions globally, using individually linked data and accounting for differences in multiple socio-demographic and health factors.
Materials and methods
Datasets
The 45 and Up Study is a longitudinal study of 267,153 NSW residents aged ≥45, randomly sampled from the general population enrolled in the Medicare Australia database, which includes records for all citizens, permanent residents, and some temporary residents and refugees.13,14 Individuals aged ≥80 and residents of regional areas were oversampled by a factor of 2, and all individuals resident in remote areas were sampled. Sampled individuals were sent an invitation to participate. If they consented, participants completed a postal baseline questionnaire on enrolment between 2006 and 2009, including socio-demographic and general health details and health behaviours. Participants agreed to their details being linked to databases of routinely collected health information including: (i) the NSW Pap Test Register (NSW PTR), which collected data on women who have a Pap test including information on Pap tests, cervical histology and HPV DNA tests. The PTR data were recorded up to December 2013, and only included data from the pre-renewed NCSP (HPV tests were only performed for triage or test of cure); (ii) the NSW Admitted Patient Data Collection (NSW APDC), which records all inpatient admissions to NSW public and private hospitals; (iii) Medical Benefits Schedule (MBS), which includes subsidised outpatient medical services and some inpatient hospital procedures covered by the MBS; and (iv) the NSW Registry of Births, Deaths and Marriages: Death Registrations (NSW RBDM Death).
Study cohort/sample
The study cohort was derived from females in the 45 and Up Study13,14 aged 45–69 throughout the study period, 2008–2012. For the current analysis, women were excluded if they (i) were aged <45 at time of baseline questionnaire; (ii) were aged ≥70 on 31/12/2012 (as not eligible for routine cervical screening for the whole study period); (iii) had an invalid or missing entry for country of birth; (iv) self-reported having had a hysterectomy in the baseline questionnaire; (v) had a record of hysterectomy in the APDC or MBS datasets prior to 31 December 2012; (vi) died prior to 31 December 2012. Women were excluded from the main analyses if they had an abnormal cytology test, or any histology test recorded in the 5 years prior to the participation period, as they may have been undergoing more intensive testing as follow-up of an abnormal cytology test and were not part of the routine screening programme.
Statistical analysis
Descriptive statistics were used to summarise the data. For the primary analyses, we examined cervical screening participation over a 3-year (2010–2012) and 5-year period (2008–2012), stratified by country or region of birth. Women were considered to have participated in the cervical screening programme if they had at least one cytology test recorded in the stated time period. We used a 3-year window to capture participating women, in line with prior analyses, 7 and because, in the cytology-based programme, women were sent a reminder if they had not been screened within 27 months of their last routine negative cytology test.
Supplementary analyses examined 3-year and 5-year participation among immigrant women stratified by (i) women who spoke a language at home other than English compared to women who spoke English at home; (ii) the number of years immigrant women had lived in Australia, calculated in 2009 (by category <5, 5–9, 10–14, 15–19, 20–24, 25–29, 30–34, 35–39 and ≥40); and (iii) overseas-born women who had lived in Australia for ≥20 years, compared to Australian-born women.
For the primary analyses, there were 26 categories for place of birth, incorporating individual countries of birth included in the 45 and Up Study baseline questionnaire and other countries grouped according to the Australian Bureau of Statistics Standard Australian Classification of Countries, 2016 15 (see Supplemental material, Table S1). Countries reported individually were excluded from their associated region. For the supplementary analyses of years living in Australia, 12 categories for place of birth were used (Australian-born women were excluded from the analyses of years lived in Australia) (see Table S2).
We performed logistic regression to estimate odds ratios (ORs) and 95% confidence intervals (CI) for the dependent variable ‘screening participation’ (yes/no) adjusted for variables known to influence either screening behaviour and/or cervical precancer/cancer risk, including age, remoteness of residence (measured using the Accessibility/Remoteness Index of Australia, 2006), 16 socio-economic status (SES) of residence (measured using the Index of Relative Socio-economic Disadvantage, 2006), 17 household income, highest level of education, health insurance status, parity, marital status, menopausal hormone therapy (MHT) status, smoking status, language other than English spoken at home, and place of birth. We tested for all two-way interactions between place of birth and other covariates, and reported the results where interactions were significant. In sensitivity analyses, we varied the time prior to the participation period over which we looked for prior abnormal cytology and histology results before excluding women from the analyses (2 years or no exclusion, compared to 5 years for the main analyses). Data were analysed using STATA version 16 (STATA Corp, TX, USA).
Ethics approval
The 45 and Up Study was approved by the University of New South Wales Human Research Ethics Committee. This study was approved by the NSW Population and Health Services Research Ethics Committee (approval number 2019/ETH01746).
Results
Of 267,153 baseline 45 and Up Study participants, there were 67,711 females aged ≥45 eligible for cervical screening between 2008 and 2012; after the exclusion of the 361 females (0.5%) with a missing/invalid country of birth, 67,350 women were included in the study. Socio-demographic and health characteristics of the screen-eligible women on the baseline questionnaire by place of birth are shown in Table 1. Of the eligible women, 76.1% were born in Australia, 13.1% in Europe, 4.7% in Asia, 2.3% in New Zealand, 1.9% in the Middle East/Africa, 1.5% in the Americas and 0.4% in Oceania (other). The proportion of overseas-born women in our study compared to all NSW residents aged 45–74 in June 2006 is shown in Table 2.
Socio-demographic and health characteristics of women eligible for cervical screening 2008–2012 in the 45 and Up Study, New South Wales, Australia, by place of birth at baseline*.
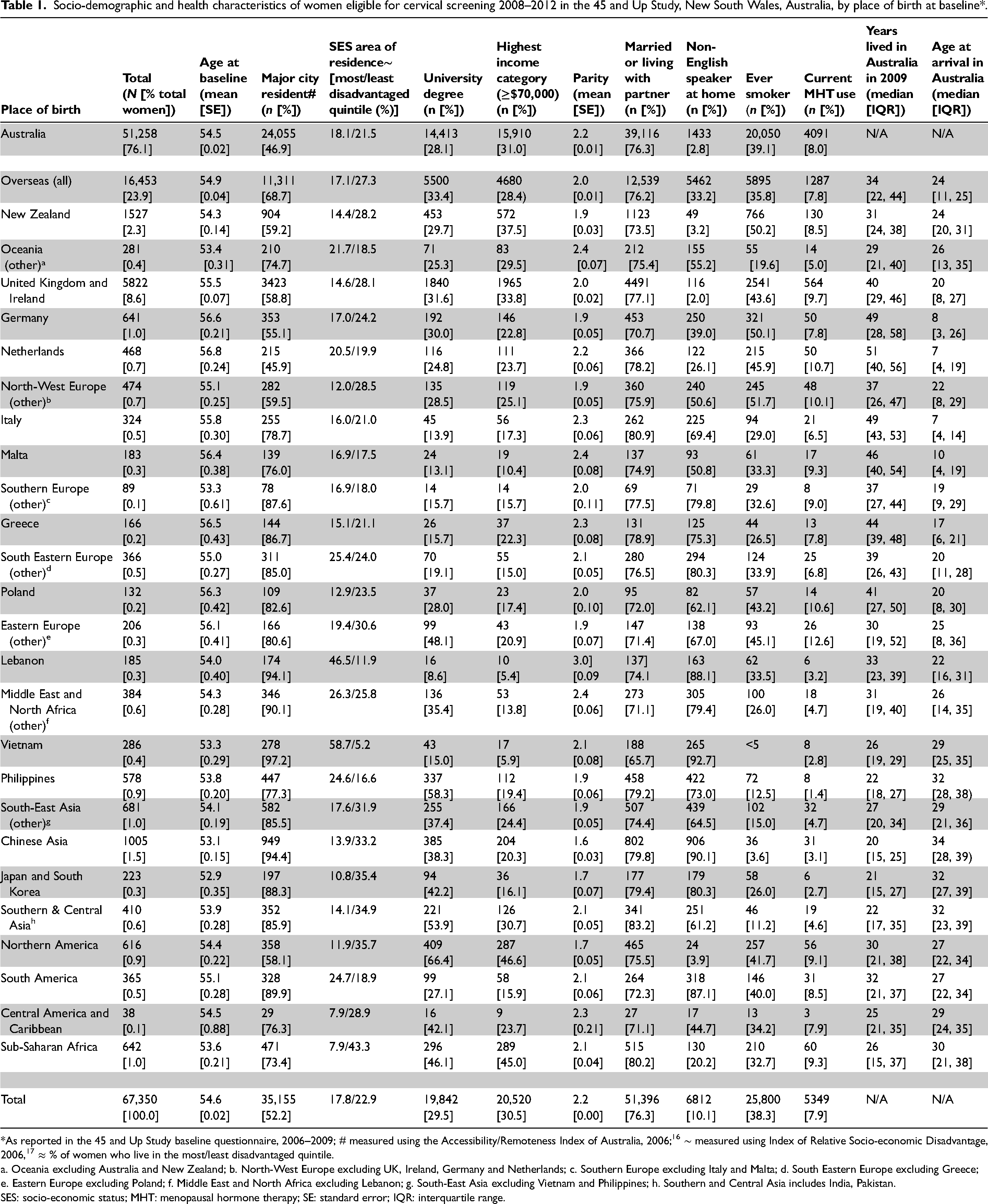
*As reported in the 45 and Up Study baseline questionnaire, 2006–2009; # measured using the Accessibility/Remoteness Index of Australia, 2006; 16 ∼ measured using Index of Relative Socio-economic Disadvantage, 2006, 17 ≈ % of women who live in the most/least disadvantaged quintile.
a. Oceania excluding Australia and New Zealand; b. North-West Europe excluding UK, Ireland, Germany and Netherlands; c. Southern Europe excluding Italy and Malta; d. South Eastern Europe excluding Greece; e. Eastern Europe excluding Poland; f. Middle East and North Africa excluding Lebanon; g. South-East Asia excluding Vietnam and Philippines; h. Southern and Central Asia includes India, Pakistan.
SES: socio-economic status; MHT: menopausal hormone therapy; SE: standard error; IQR: interquartile range.
Country of birth and language other than English spoken at home in the study cohort (women in 45 and Up Study aged ≥45 years in 2006–2009 eligible for cervical screening) compared to NSW/Australian population data.
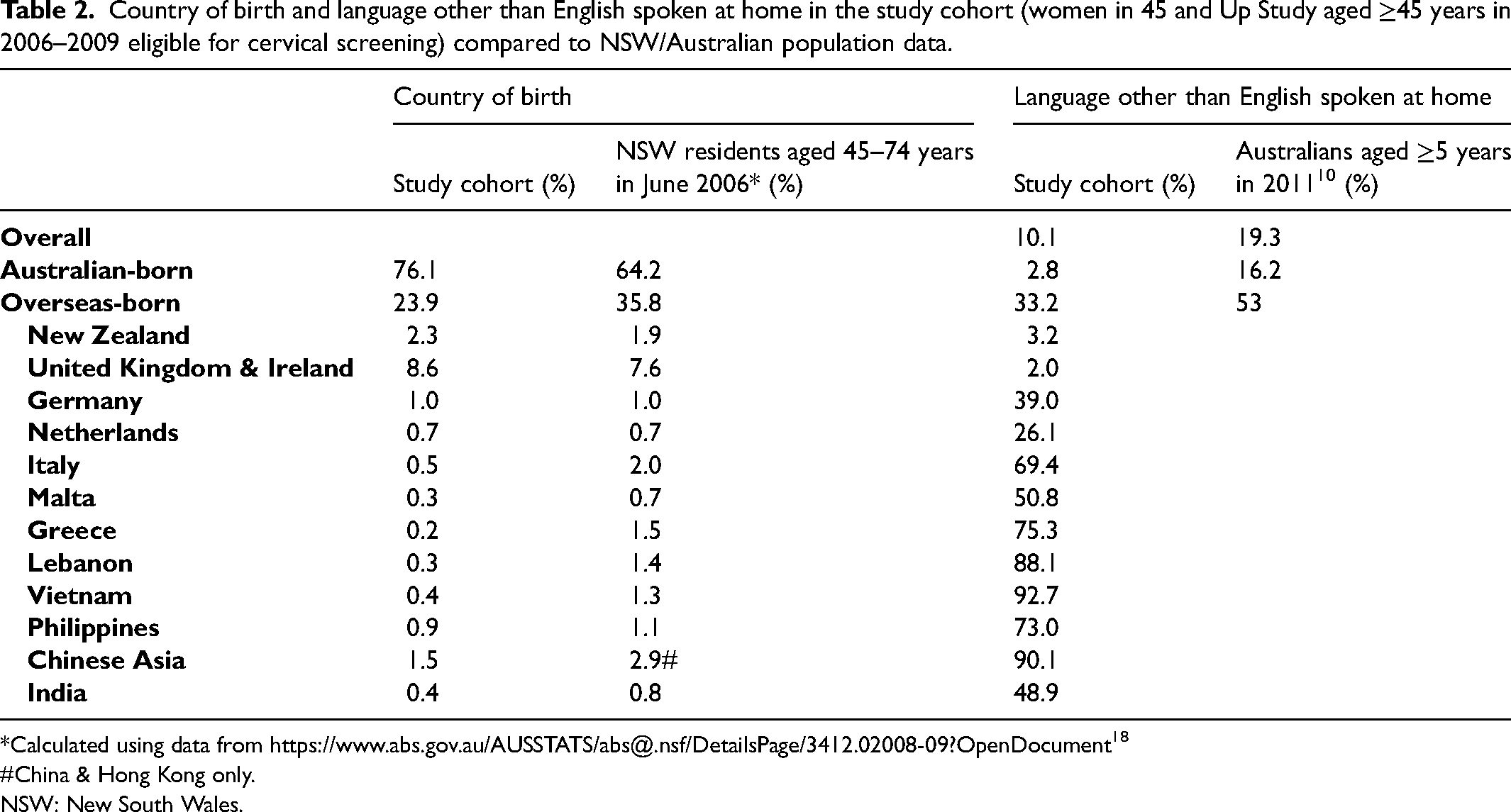
*Calculated using data from https://www.abs.gov.au/AUSSTATS/abs@.nsf/DetailsPage/3412.02008-09?OpenDocument 18
#China & Hong Kong only.
NSW: New South Wales.
The mean age of the study cohort was 54.6 years at baseline. Compared to Australian-born women, women born overseas (except in the Netherlands) were more likely to be resident in a major city, but other characteristics varied by place of birth. Overall, 10.1% of study-cohort women spoke a language at home other than English, varying from 2 to 4% in women born in English-speaking countries, to >80% in women from South Eastern Europe, Lebanon, parts of Asia and South America (Table 1). This compares to 19.3% of the overall population aged >5 in Australia in 2011 (Table 2).
After excluding women with an abnormal cytology test or any histology test in the 5 years prior to the participation windows, 63,772 women were eligible for screening between 2010 and 2012, and 62,882 between 2008 and 2012 (Table 3). Overall, 77.0% and 83.8% of the eligible women were recorded as having at least one cytology test in 2010–2012 and 2008–2012 respectively (Table 3). Australian-born women had 3-year and 5-year participation rates of 77.8% and 84.5% respectively, while overseas-born women had participation rates of 74.3% and 81.5%. By comparison, reported 3-year and 5-year participation rates in NSW were 71.7% and 83.8% over the same time periods (women aged 45-69). 19
Three-year (2010–2012) and 5-year (2008–2012) participation rates and odds ratios for participation in the cervical screening programme, by place of birth and language spoken at home.
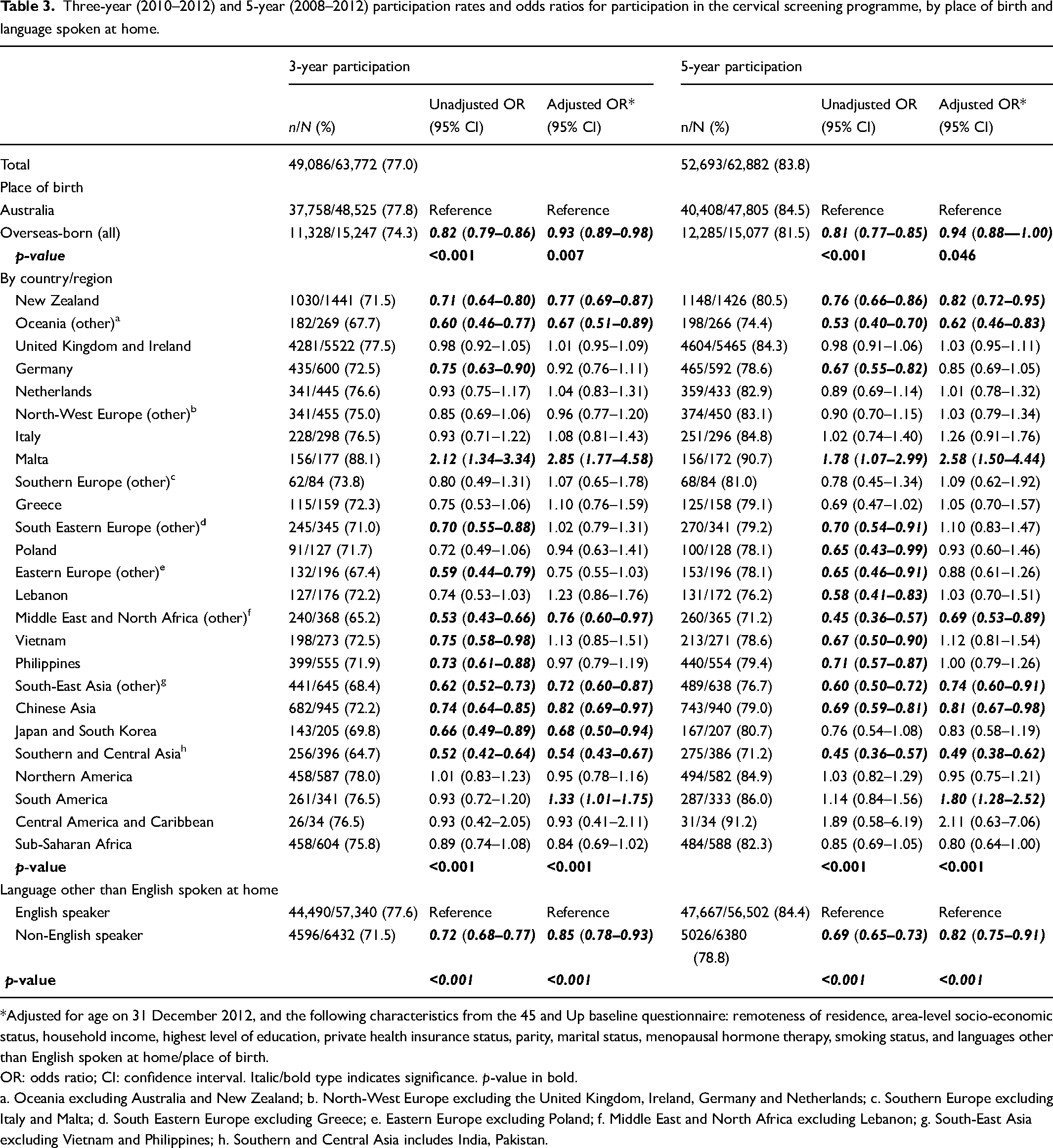
*Adjusted for age on 31 December 2012, and the following characteristics from the 45 and Up baseline questionnaire: remoteness of residence, area-level socio-economic status, household income, highest level of education, private health insurance status, parity, marital status, menopausal hormone therapy, smoking status, and languages other than English spoken at home/place of birth.
OR: odds ratio; CI: confidence interval. Italic/bold type indicates significance. p-value in bold.
a. Oceania excluding Australia and New Zealand; b. North-West Europe excluding the United Kingdom, Ireland, Germany and Netherlands; c. Southern Europe excluding Italy and Malta; d. South Eastern Europe excluding Greece; e. Eastern Europe excluding Poland; f. Middle East and North Africa excluding Lebanon; g. South-East Asia excluding Vietnam and Philippines; h. Southern and Central Asia includes India, Pakistan.
Participation among overseas-born women by place of birth was significantly different compared to Australian-born women for both 2010–2012 and 2008–2012 (p < 0.001). Compared to Australian-born women, women had lower screening 3-year participation if they were born in Southern and Central Asia (adjusted odds ratio [aOR] 0.54, 95% confidence interval [CI]: 0.43–0.67), Oceania (0.67, 0.51–0.89), Japan and South Korea (0.68, 0.50–0.94), South-East Asia (0.72, 0.60–0.87), Middle East and North Africa (0.76, 0.60–0.97), New Zealand (0.77, 0.69–0.87) or Chinese Asia (0.82, 0.69–0.97) (Table 3). Additionally, women born in Germany, South Eastern Europe, Eastern Europe, Vietnam and the Philippines had significantly reduced unadjusted odds of 3-year participation compared to Australian-born women, but adjusted odds were no longer significantly different to Australian-born women. Women from Malta (2.85, 1.77–4.58) and South America (1.33, 1.01–1.75) had greater odds of screening participation over the 3 years compared to Australian-born women (Table 3). While participation increased for the 5-year period, adjusted relative screening participation was generally similar to 3-year participation in immigrant groups compared to Australian women except for Japanese/South Korean-born women, for whom 5-year participation was no longer significantly lower compared to Australian-born women (Table 3).
All the socio-demographic and health covariates were associated with lower screening participation (Table S3). The interaction term for place of birth and parity was borderline significant for 3-year participation (p = 0.05) and significant for 5-year participation (p = 0.04). Therefore, ORs for place of birth were calculated by parity modelled as a continuous variable (Tables 4, S4, S5). Parity was positively associated with participation in women born in some countries/regions, e.g. Australia, South Eastern Europe (other), Lebanon, South-East Asia (other), Chinese Asia, South America, and Sub-Saharan Africa. By contrast, it was negatively associated with participation in women from other regions/countries, e.g. Oceania, Germany, Southern Europe, Eastern Europe (other), Japan/South Korea, and Northern America.
Three-year (2010–2012) and 5-year (2008–2012) ratesⱡ and odds ratios for participation in the cervical screening programme by place of birth and parity^.
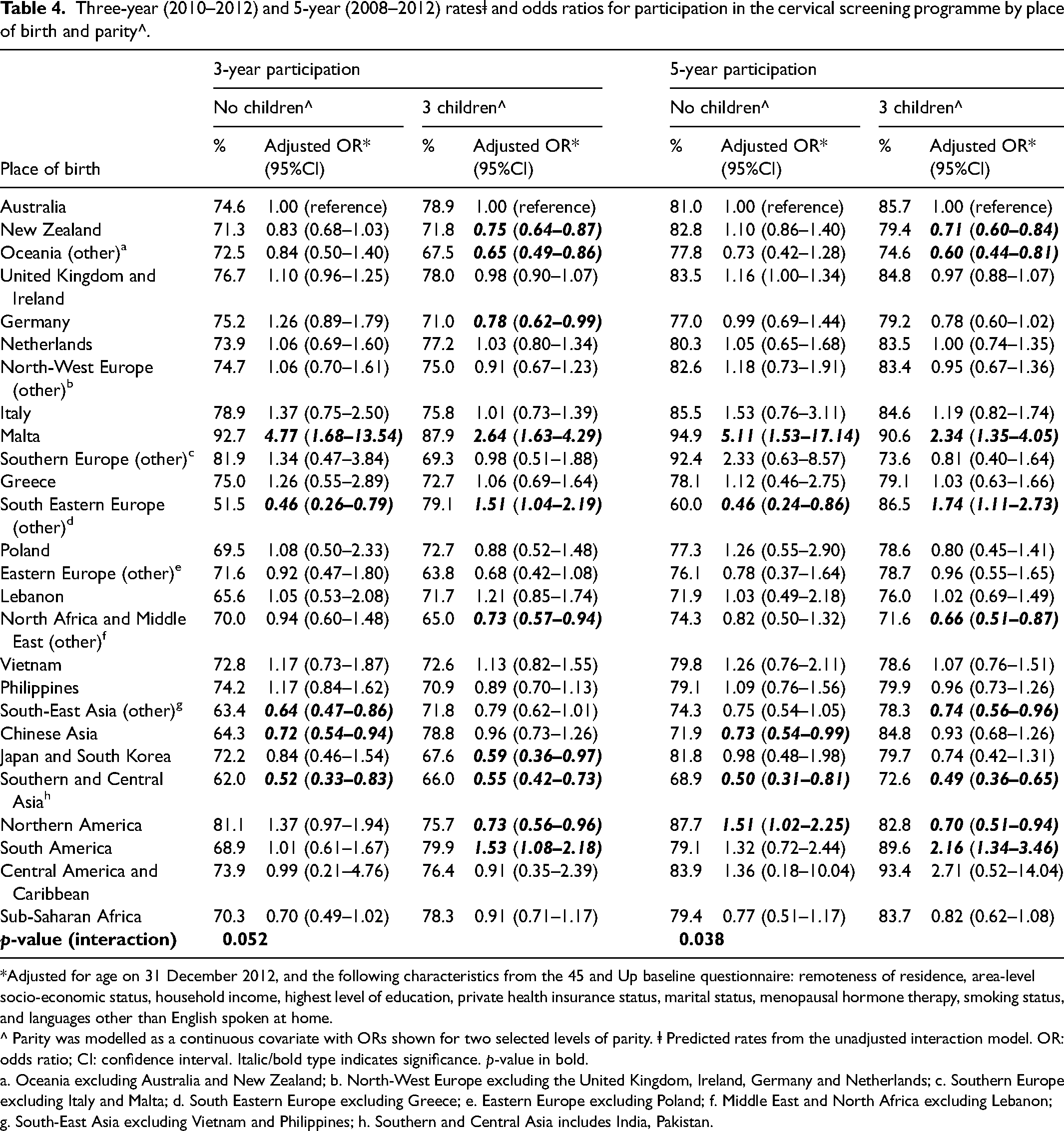
*Adjusted for age on 31 December 2012, and the following characteristics from the 45 and Up baseline questionnaire: remoteness of residence, area-level socio-economic status, household income, highest level of education, private health insurance status, marital status, menopausal hormone therapy, smoking status, and languages other than English spoken at home.
^ Parity was modelled as a continuous covariate with ORs shown for two selected levels of parity. ⱡ Predicted rates from the unadjusted interaction model. OR: odds ratio; CI: confidence interval. Italic/bold type indicates significance. p-value in bold.
a. Oceania excluding Australia and New Zealand; b. North-West Europe excluding the United Kingdom, Ireland, Germany and Netherlands; c. Southern Europe excluding Italy and Malta; d. South Eastern Europe excluding Greece; e. Eastern Europe excluding Poland; f. Middle East and North Africa excluding Lebanon; g. South-East Asia excluding Vietnam and Philippines; h. Southern and Central Asia includes India, Pakistan.
Sensitivity analyses varying the time prior to the participation period over which we looked for prior abnormal cytology and histology results before excluding women from the analyses (no exclusion or 2 years versus 5 years in the main analyses), were not substantially different from the main analyses (results not shown).
The length of time immigrant women had lived in Australia was significantly associated with 3-year and 5-year participation in the NCSP, after adjusting for place of birth, age, remoteness of residence, area-level SES, income, education, health insurance status, parity, marital status, MHT status, smoking status, and language other than English spoken at home (p < 0.001) (Table S6). The odds of participating increased with years lived in Australia but plateaued from ≥15–19 years of living in Australia. For 3-year participation, there was a significant interaction between years of living in Australia and place of birth (Table S7). Compared to Australian-born women, immigrant women who had lived in Australia for ≥20 years and who were born in New Zealand, Oceania, North-East Asia and Southern and Central Asia had significantly lower odds of 3-year and 5-year screening participation than Australian-born women; by contrast, women from South and Central America had persistently significantly higher screening participation (Table 5).
Three-year (2010–2012) and 5-year (2008–2012) rates and odds ratios for participation in the cervical screening programme among Australian-born women and immigrant women who have lived in Australia for 20 years or more.
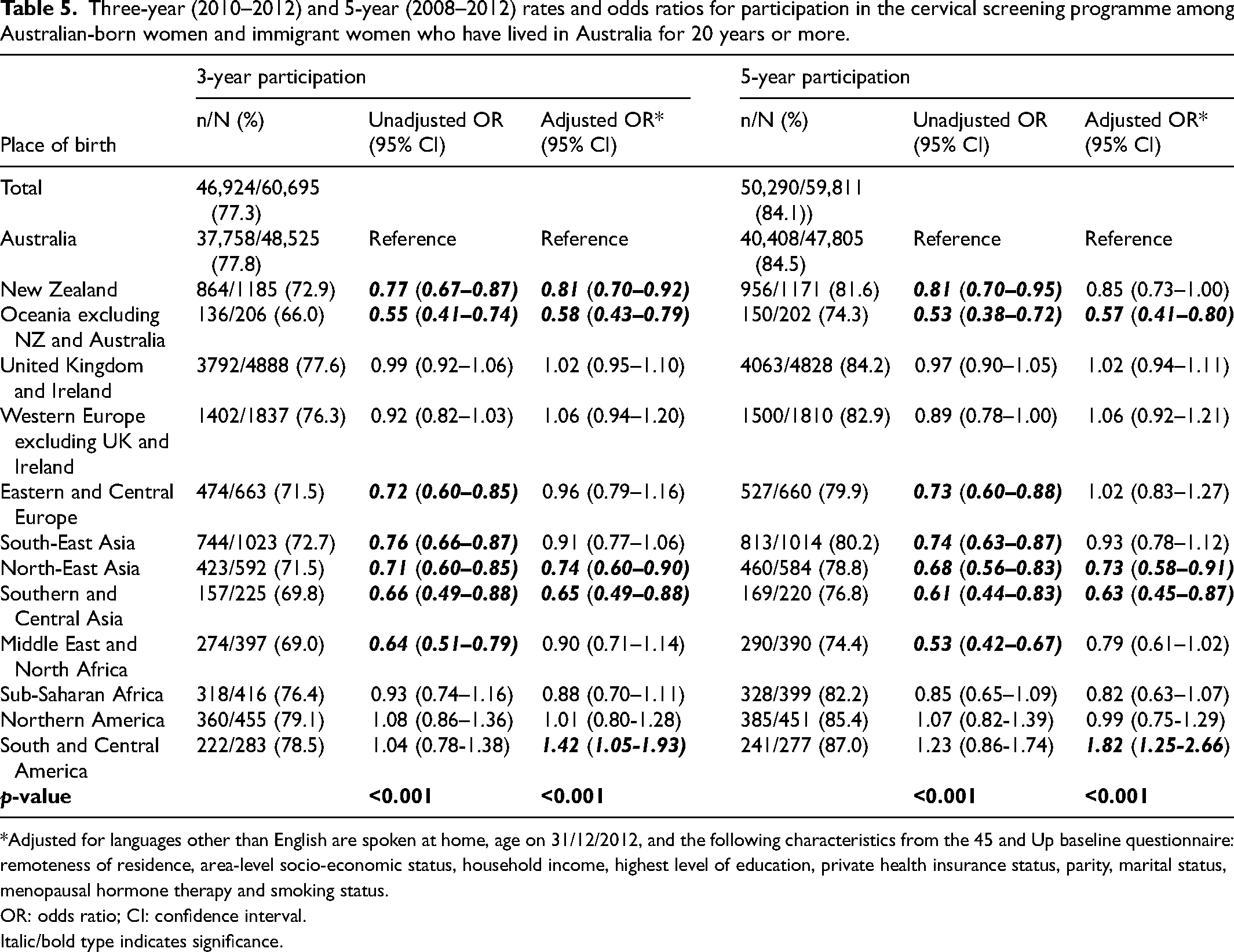
*Adjusted for languages other than English are spoken at home, age on 31/12/2012, and the following characteristics from the 45 and Up baseline questionnaire: remoteness of residence, area-level socio-economic status, household income, highest level of education, private health insurance status, parity, marital status, menopausal hormone therapy and smoking status.
OR: odds ratio; CI: confidence interval. Italic/bold type indicates significance.
Discussion
This is the first Australian data linkage study examining screening in immigrant women from all regions globally. We found that groups previously identified as being underscreened 6 continue to have lower participation in the NCSP than Australian-born women. This includes women from Southern/Central Asia, South-East Asia and the Middle East/North Africa. In addition, our study identified other groups to be underscreened, including women born in New Zealand, Oceania, Japan/South Korea, and Chinese Asia. Higher 3-year and 5-year participation were seen in immigrant women from Malta and South America, the reasons for which are unclear.
Our study confirmed previous findings that participation by immigrant women increased with time lived in Australia, 6 for about 10–15 years after migration. However, we showed that relative participation plateaued at 15–19 years after arrival to Australia. While women who have lived in Australia for >20 years may be expected to have undergone a greater degree of acculturation than more recent immigrants, we found a persisting lower level of participation in some groups of overseas-born women even after decades of living in Australia.
A recent study of infection-related cancers diagnosed between 2005 and 2014 in Australia found women born in New Zealand, Polynesia (in the Oceania region) and the Philippines had an increased incidence of cervical cancer compared to Australian-born women. 20 We found significantly lower screening participation rates in women born in New Zealand and Oceania. Conversely, other groups that we identified as having relatively lower screening rates had a lower cervical cancer incidence rate compared to Australian-born women, including women born in the Middle East, North Africa, and Southern Asia. While screening is crucial in reducing cervical cancer incidence in immigrant women, other factors may affect cervical cancer risk, including HPV exposure (related to sexual behaviour; HPV infection is lower in some of the countries of birth) 20 as well as potential co-factor exposure (i.e., oral contraceptive use, smoking, and HIV infection). 21
To our knowledge, New Zealand-born women have not previously been identified as an underscreened group of women in Australia. This group of women have an elevated incidence of cervical cancer compared to Australian-born women, 20 and are one of the larger groups of immigrant women (Table 2). Further studies are needed to investigate if specific subgroups of New Zealand-born women in Australia should be considered, as coverage rates in Māori, Pacific and Asian women within New Zealand are lower compared to those in European/other women. 22
In all groups of immigrant women with relatively lower screening rates, adjusting for socio-demographic/health factors attenuated the difference in screening compared to Australian-born women. In some immigrant groups, including women from the Philippines (a group with higher cervical cancer rates), Vietnam and parts of Europe, the unadjusted participation rate was significantly lower, but the association was no longer significant in the adjusted analysis. This suggests that differences in screening participation between these groups of overseas-born and Australian-born women are, partly or largely, explained by differences in socio-demographic and health characteristics related to lower screening participation (e.g., lower area-level SES).
A limitation of our analysis pertains to the representativeness of the women included in the 45 and Up Study compared to the population of immigrant women in Australia eligible for cervical screening. The study cohort is limited to women aged ≥45 in 2006–2009, but is consistent with the general population of overseas-born females aged ≥45 in Australia being longer-standing immigrants. 10 As the baseline questionnaire was only available in English, participation was limited to women with adequate literacy in English. 13 In our study, 33.4% of overseas-born women reported speaking a language other than English at home. In the general population, 49% of longer-standing migrants reported speaking another language at home in 2011, but 51% of this group also reported speaking English well. 10 While the overall 3-year participation rate in 2010–2012 (77.0%) was higher than the rate reported for NSW women aged 45–69 (71.7%) over this time period, 19 the 5-year participation rate (2008–2012) was consistent between our study (83.8%) and figures reported for women aged 45–69 in NSW (83.8%). 19 The cohort included in the 45 and Up Study has a higher proportion of Australian-born and English-speaking-at-home women who have slightly better screening coverage. However, it has previously been found that, while the absolute prevalence of studied factors/exposures in the 45 and Up Study might vary from state/national data, the estimates of relative measures of effect were consistent. 23
Our study examines participation in the cytology-based NCSP, which involved 2-yearly screening. Five-yearly HPV testing has been recommended since December 2017 and so, while 2-year participation would be relevant to the transition period, most women have now had their first HPV test and transitioned to a 5-year recommendation. There are, however, currently no comprehensive data available since the change in the screening programme for participation by CALD status, with the data on the National Cancer Screening Register being incomplete in 85% of women. 24 Our data are important for obtaining information on short- and long-term screening coverage in immigrant women. Yearly updates assessing the progress of the components important for cervical cancer elimination in Australia 25 will assess CALD participation in the future, as it becomes available.
Strengths of this study include the use of routinely collected data from a screening register, the NSW PTR, rather than self-reported screening which overestimates participation. 26 The data covers a long period of time post-immigration, allowing for the unique exploration of time since migration effects. We included screening participants from all regions and examined immigrant women from individual countries with large populations in NSW. A particular strength of our study was that we were able to examine and account for multiple potential confounders. We were also able to exclude women who had had a hysterectomy prior to baseline or prior to the end of the participation windows using self-reported hysterectomies from the baseline questionnaire, or documented hysterectomy between baseline and 31 December 2012 using APDC/MBS datasets, respectively.
Between December 2017 and June 2022, women aged ≥30 who were overdue for screening by ≥2 years were eligible for screening using a self-collected vaginal sample. However, uptake was very low under these highly restricted criteria, 27 with barriers including difficulty identifying eligible women for practitioners and poor awareness of the self-collection option by potential participants. 28 On 1 July 2022, the option of self-collection was extended to all screen-eligible women and people with a cervix within the NCSP. 2 This includes non-speculum ‘self-collection’ of a vaginal sample by a clinician, 1 which has previously been shown to be a favoured alternative in CALD women, particularly Asian-born women, who lacked the confidence to take their own specimen. 29 The change, supported by multi-language consumer resources, 30 provides new opportunities to improve screening programme participation by groups of women who have been hard to reach.
Short- and medium-term elimination goals rely on screening. However, ensuring catch-up HPV vaccination of adolescents and younger women immigrating from countries without a routine vaccination programme (funded for those aged up to 25) is vital to ensure equitable elimination of cervical cancer in the longer term in all groups of women in Australia.12,31
Our study identifies groups of immigrant women underscreened for cervical cancer precursors, with lower screening participation persisting for decades after immigration. Self-collection may offer a more acceptable alternative to these groups of women, and may be complemented by other, community-led co-designed approaches to increase screening, to support the achievement of elimination of cervical cancer across Australia.
Supplemental Material
sj-docx-1-msc-10.1177_09691413231184334 - Supplemental material for Participation in the national cervical screening programme among women from New South Wales, Australia, by place of birth and time since immigration: A data linkage analysis using the 45 and up study
Supplemental material, sj-docx-1-msc-10.1177_09691413231184334 for Participation in the national cervical screening programme among women from New South Wales, Australia, by place of birth and time since immigration: A data linkage analysis using the 45 and up study by Susan Yuill, Sam Egger, Megan A Smith, Louiza Velentzis, Marion Saville, Erich V Kliewer, Deborah Bateson and Karen Canfell in Journal of Medical Screening
Footnotes
Acknowledgements
This research was completed using data collected through the 45 and Up Study (![]() ). The 45 and Up Study is managed by the Sax Institute in collaboration with major partner Cancer Council NSW; and partners: the Heart Foundation; NSW Ministry of Health; NSW Department of Communities and Justice; and Australian Red Cross Lifeblood. We thank the many thousands of people participating in the 45 and Up Study, the Centre for Health Record Linkage for the record linkage, Services Australia, the NSW Ministry of Health and Cancer Institute NSW for the use of their data, and the Secure Unified Research Environment (SURE) for provision of secure data access.
). The 45 and Up Study is managed by the Sax Institute in collaboration with major partner Cancer Council NSW; and partners: the Heart Foundation; NSW Ministry of Health; NSW Department of Communities and Justice; and Australian Red Cross Lifeblood. We thank the many thousands of people participating in the 45 and Up Study, the Centre for Health Record Linkage for the record linkage, Services Australia, the NSW Ministry of Health and Cancer Institute NSW for the use of their data, and the Secure Unified Research Environment (SURE) for provision of secure data access.
Availability of data
The data were provided by a third party and were accessed using the Secure Unified Research Environment (SURE), a secure computing environment that can be accessed remotely to analyze linked health data. As data could potentially compromise participant confidentiality, on-provision is not permitted. The data are available to all researchers but will require approval from an Australian Human Research Ethics Committee and the data custodians. Data access enquires can be made to the Sax Institute (see ![]() ).
).
Conflict of interest disclosure
MSm receives contract funding to her institution from Commonwealth Department of Health (Australia), the Ministry of Health (New Zealand), and the National Screening Service (Ireland) for projects related to cervical cancer control. MSa is an investigator on the Compass trial for which her organisation, ACPCC. has received kits and partial funding from Roche. VCS Pathology has also received free test kits from Roche, Seegene, Cepheid, Becton Dickinson, Abbott, AusDiagnostics and Atila Biosystems for research purposes. DB is a co-PI on a major implementation programme Elimination of Cervical Cancer in the Western Pacific which has received support from the Minderoo Foundation and the Frazer Family Foundation and equipment donations from Cepheid Inc. DB receives contract funding from Commonwealth Department of Health, Australia to her institution for work to monitor the safety of the NCSP. KC is co-PI of an investigator-initiated trial of cervical screening, ‘Compass’, run by the Australian Centre for Prevention of Cervical Cancer (ACPCC), which is a government-funded not-for-profit charity. Compass receives infrastructure support from the Australian government and the ACPCC has received equipment and a funding contribution from Roche Molecular Diagnostics, USA. KC is also co-PI on a major implementation programme Elimination of Cervical Cancer in the Western Pacific which has received support from the Minderoo Foundation and the Frazer Family Foundation and equipment donations from Cepheid Inc. KC receives contract funding from Commonwealth Department of Health, Australia to her institution for work to monitor the safety of the NCSP. KC also receives support for a range of other Australian and international government projects including support from philanthropic organisations, WHO, and government agencies related to cervical cancer control.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Susan Yuill receives a scholarship from Cancer Council NSW. Megan Smith receives salary support from the National Health and Medical Research Council (APP1159491) and Cancer Institute NSW (ECF181561). Karen Canfell receives salary support from the National Health and Medical Research Council (APP1194679).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.