
Abstract

Despite being documented it is not widely recognized that important causal risk factors of potential significance in the primary prevention of disease usually make poor screening tests. 1 This arises because the quantitative association between causal risk factors and disease is usually too small for the risk factor to be a useful screening test. Two examples are the measurement of serum cholesterol as a screening test for heart attacks 1 and blood pressure measurement as a screening test for stroke. 2 While these risk factors are the drivers of heart attacks and strokes throughout the world, when considered as screening tests, they typically have detection rates (sensitivities) for a 5% false positive rate (DR5) of no more than 15% to 20%. Even non-causal risk factors have been invoked as screening tests when their screening performance is poor, for example, coronary calcification as a possible test for coronary heart disease. 3 There is a numerical relationship between measures widely used in investigating causal risk factors such as relative risk or odds ratios and measures of screening performance such as the DR5. A web-based Risk-Screening Converter is available on the Medical Screening Society website (https://www.medicalscreeningsociety.com/rsc.asp). The Risk-Screening Converter converts measures identified as risk factors in epidemiological studies which have a Gaussian distribution into measures of screening performance of potential tests and vice versa. The Converter can be used to determine whether measures such as the odds ratio across the highest and lowest quintile groups of a risk factor are large enough to be considered as a screening test.
For example, the Risk-Screening Converter can be used to show that cholesterol is not a good screening test for ischaemic heart disease. In a study of the concentration of total cholesterol in men with a future ischaemic heart disease event 4 the odds ratio between the highest and lowest quintile groups of the distribution of serum total cholesterol was approximately 3.3, similar to the results from other studies.5,6 When this odds ratio is entered into the Risk-Screening Converter (see Figure 1) an estimated DR5 of 11.2% is obtained showing that serum cholesterol measurement in adults is not a good screening test for ischaemic heart disease despite it being widely used for this purpose.
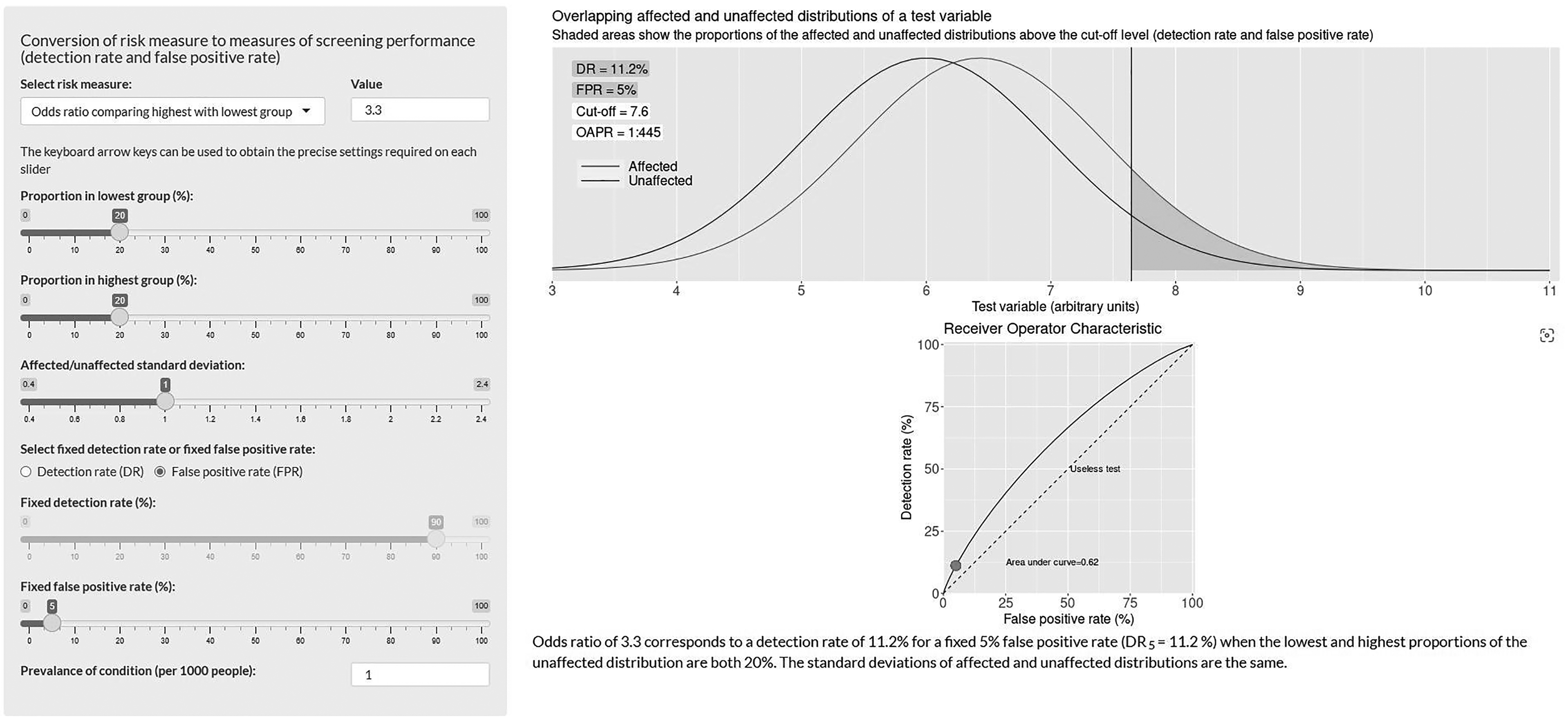
A screenshot from the Risk-Screening Converter illustrating the screening performance of a screening test for future ischaemic heart disease events using total cholesterol measurements. The figure shows that the odds ratio of having future ischaemic heart disease events between the highest and lowest quintile groups of a total cholesterol level of 3.3 converts to a DR5 of 11.2%.
The Converter has been used in a study to assess the incremental value of polygenic risk scores (PRS) over traditional risk factor scores in the prediction of coronary heart disease events. 7 The study used the results from five cohorts. The cohort with the most discriminatory PRS 8 reported an odds ratio of 4.51 between the highest and lowest quintile groups of the distribution of PRS. The Converter was used in the study 7 to show that this odds ratio corresponds to a false positive rate of 77.1% at a 90% detection rate (FPR90), which is equivalent to a DR5 of 13.5%. The Converter shows that adding a PRS to traditional risk scores adds only a few percentage points to the DR5.
The Risk-Screening Converter may be helpful in distinguishing genuinely worthwhile screening tests from tests of little or no value.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
The Editors
Journal of Medical Screening