
Abstract
The objective was to determine if a screening tool for obstructive sleep apnea could be used to predict adverse perinatal outcomes. This was a prospective observational study of patients receiving prenatal care and universally screened for obstructive sleep apnea with the STOP Questionnaire (four questions related to
Introduction
Obstructive sleep apnea (OSA) is a condition characterized by recurrent upper airway obstruction, hypoventilation, and intermittent nocturnal hypoxia. Given the increasing incidence of obesity among reproductive-aged women, OSA presents unique complications during pregnancy including increased risk for gestational diabetes, preeclampsia, cesarean delivery, preterm delivery (PTD), fetal growth restriction (FGR), wound complications, neonatal intensive care unit (NICU) admission, and hyperbilrubinemia.1–3 The most accurate method to diagnose OSA remains polysomnography, but its cost and prolonged time involvement presents clear limitations.
4
Screening questionnaires such as the Berlin, modified Berlin, Epworth Sleepiness Scale, OSA50 questionnaires, sleep apnea clinical scores, STOP-Bang, and STOP are tools for identifying potential OSA.
5
In a recent systemic review, the STOP Questionnaire (four questions related to
Patients/Methods
The research method employed was a prospective observational study of patients receiving prenatal care at a tertiary care clinic during a 1-year time period (June 2013 to May 2014). Patients were universally screened for OSA using the STOP Questionnaire, which consists of four concise questions: (1) Do you
Univariate analysis on the following adverse perinatal outcomes: cesarean delivery, preeclampsia, PTD (<37 weeks), low birth weight (LBW) (<2500 g), FGR, and NICU admission, compared positive versus negative screens. Significant outcome variables were included in a backwards logistic regression with the following confounding variables: maternal age, body mass index, parity, previous stillbirth, previous PTD, maternal ethnicity, hypertension disorder, diabetes, gastroesophageal reflux disease, asthma, chronic obstructive pulmonary disease, depression, thyroid disorder, polyhydramnios, oligohydramnios, history of stroke, history of heart attack, and history of heart failure.
Results
Included in analysis were 442 (84.8%) patients with a mean age of 25.3 ± 5.6 years and high tobacco (241; 54.5%) and illicit drug use (155; 35.1%). The mean body mass index of those who screened positive was statistically significantly higher than of those that screened negative (33.0 ± 9.5 vs 29.4 ± 7.9; p = 0.003). In addition, rates of hypertension (21.9% vs 4.2%; p < 0.001), asthma (25% vs 13.5%; p = 0.023), thyroid disease (10.9% vs 3.2%; p = 0.012), substance use (45.3% vs 33.3%; p = 0.045), and depression (37.5% vs 20.9%; p = 0.005), were statistically significantly higher in women screening positive versus negative. Positive STOP screens were assessed in 64 (14.5%) patients and were statistically significantly associated with more PTD (23.4% vs 10.1%; p = 0.006, significance was adjusted to 0.008 due to the number of tests), LBW infants (20.3% vs 10.3%; p = 0.023) and NICU admissions (14.1% vs 6.3%, p = 0.039). Backward logistic regression indicated that a positive STOP screen was associated with PTD and NICU admission. For PTD, history of PTD was the strongest predictor with an odds ratio (OR) of 4.2 (95% confidence interval (CI) 2.0–8.8), followed by a positive STOP screen with an OR 2.8 (95% CI 1.4–5.8) and nulliparity with an OR 2.3 (95% CI 1.2–4.4). For NICU admission, a positive STOP was the only significant predictor with 2.5 OR (95% CI 1.1–5.7; p = 0.036).
The positive STOP screening test performance (Table 1) had a specificity around 86% for all outcomes, but was low in sensitivity (preterm 28.3%, NICU 27.3%, and LBW 25%). False positive rate for all outcomes was less than 15%.
Positive screening test performance for perinatal outcomes.
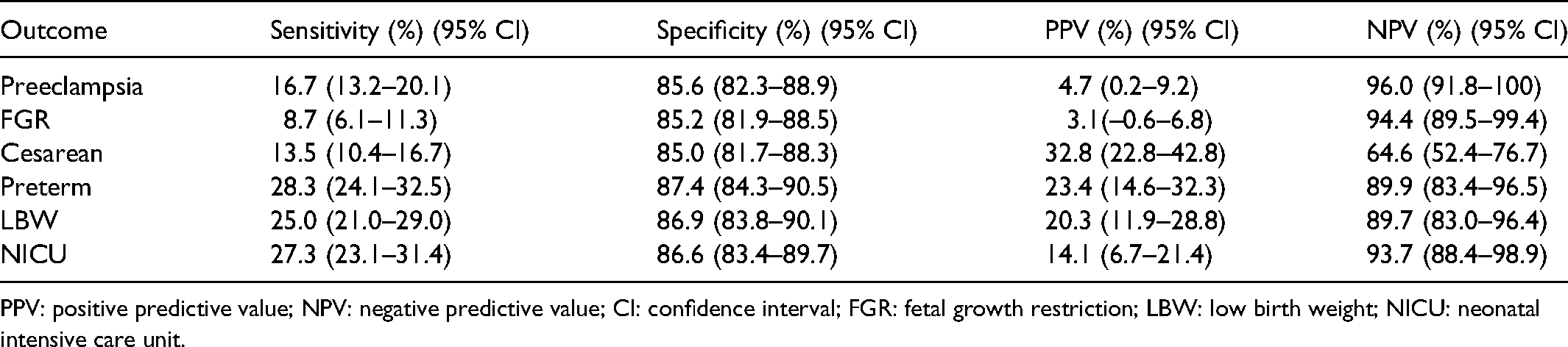
PPV: positive predictive value; NPV: negative predictive value; CI: confidence interval; FGR: fetal growth restriction; LBW: low birth weight; NICU: neonatal intensive care unit.
Discussion
Our study corroborated others that found a positive STOP screen associated with a statistically significant increased risk of LBW, PTD, and NICU admission, and those that found that a positive STOP screen was predictive of PTD and NICU admission using logistic regression. However, a positive STOP screen was not associated with caesarean delivery, FGR, or cardiovascular outcome perhaps because of the high prevalence of obesity among the study population.
While self-assessments or screening tools for OSA have independently been shown to be predictive of PTD, they have not included the STOP questionnaire. Our finding of a positive STOP screen predicting NICU admissions, with an OR of 2.5, is similar to the results of a study that found women with sleep disorder breathing had a higher rate of infants admitted to the NICU (OR = 1.90; CI: 1.38–2.61) 7 and a systematic review reporting a significant association between sleep disorder breathing and NICU admission (OR = 2.43; 95% CI, 1.61–3.68; p < 0.001). 8 This study is an example of finding reasonable association between the screening tool and outcome, but screening performance is too low and therefore does not pass the test of being a worthwhile screening tool. 9
Our study had several strengths (a prospective design, moderate sample size and inclusion of confounding variables) and limitations (single center, conducted several years ago (2013–2014). There was potential inaccuracy in screening results as responses were self-reported and the clinic setting might not be representative of all obstetric clinics because of higher than usual rates of tobacco and substance use. With higher rates of overweight and obese patients, there could be an obesity-related effect that was not accounted for during our analyses. There may be other confounding variables we may not have considered that could impact birth outcome.
Conclusion
In summary, our study suggests that the STOP screening questionnaire as a stand-alone tool for predicting perinatal outcomes has limited performance. However, it could be explored in combination with other factors, especially if this can increase the sensitivity for preterm birth and NICU admission where the sensitivity for STOP alone was modest. OSA is likely to become more prevalent during pregnancy with the worldwide trend in increasing obesity rates. Thus, there will be an even greater need to screen for OSA.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.