
Abstract
Objective
To analyse the positive rates of low-grade (LSIL) and high-grade (HSIL) squamous intraepithelial lesions, and cervical cancer (CC), and identify groups at high risk for CC in Guangxi.
Setting
CC screening options in Guangxi, which is the only minority autonomous area in South China, include the National Cervical Cancer Screening Project (NCCSP) and physical examination (PE).
Methods
This study was based on PE and NCCSP sample data obtained from 2012 to 2019. We calculated the positive rates of LSIL, HSIL, and CC; analysed the adjusted odds ratio (aOR) and 95% confidence intervals (CI) of the variables in multivariate logistic regression; and subsequently identified groups at high risk for CC.
Results
The positive rates of LSIL, HSIL, and CC for the total of 873,880 samples were 1.89%, 0.60%, and 0.03%, respectively. Females over 64 years of age (vs. 50–64; aOR = 2.05; 95% CI, 1.71–2.46; P < 0.001) and those from urban (vs. rural; aOR = 1.66; 95% CI, 1.57–1.76; P < 0.001), minority (vs. non-minority; aOR = 1.24; 95% CI, 1.13–1.35; P < 0.001), and coastal (vs. inland; aOR = 1.15; 95% CI, 1.06–1.25; P = 0.001) areas were associated with a high risk of HSIL. Females over 64 (vs. 50–64; aOR = 4.37; 95% CI, 2.88–6.63; P < 0.001) and those from urban (vs. rural; aOR = 3.05; 95% CI, 2.36–3.95; P < 0.001) areas were significantly associated with a high risk of CC.
Conclusion
Females from urban areas in Guangxi are at high risk for CC. Public health strategies should focus on high-risk populations.
Abbreviations
cervical cancer.
national cervical cancer screening project.
physical examination.
adjusted odds ratios.
confidence intervals.
low-grade squamous intraepithelial lesion.
high-grade squamous intraepithelial lesion.
cervical intraepithelial neoplasia 1.
cervical intraepithelial neoplasia 2.
cervical intraepithelial neoplasia 3.
Introduction
Cervical cancer (CC) is the fourth leading cause of cancer-related death in females worldwide. 1 In 2018, approximately 570,000 new cases were reported worldwide and more than 31,100 patients died directly from CC. 2 CC puts a heavy social and economic burden on individuals, families, and countries.3,4 It is also the second most common cancer that endangers females’ physical and mental health in China, 5 where its incidence and mortality are increasing.6,7 Human papillomavirus (HPV) vaccines and population-based screening are considered to be effective methods to address CC. 8
To improve the public health status of females, the health department of China implemented the National Cervical Cancer Screening Project (NCCSP) in 2009. Rural females between 35 and 64 years of age are the main target of NCCSP, and this service is free. The NCCSP also allows urban females to pay for this service. Physical examination (PE) is a program run by the Department of Health Examination in public and private hospitals. PE for females includes a CC test, and the primary PE customers are urban females. PE is not a free service, and CC test charges range between $55 and $90, depending on which reagents the customers choose. Although hundreds of hospitals in Guangxi have implemented PE to date, there are no exact data on its coverage. The NCCSP and PE programmes are voluntary and not mutually exclusive, and females are free to select either programme. It is estimated that approximately 0.26% of women have undergone both the NCCSP and PE programmes. Although health departments recommend that women undergo CC screening every three years, the NCCSP only covered 21.9% of target people in rural areas due to funding limitations, which is far below the expected rate of 80% noted in a recent report from the National People's Congress of Guangxi. It is estimated that approximately 3.9% of women have undergone CC screening multiple times. The exact data for PE coverage have not been reported.
Liquid-based cytological testing for CC screening is a conventional examination for adult females. This method has been widely used in NCCSP and PE programmes for several years. According to local health authorities, approximately 2.2 million samples were collected during the CC screening project in Guangxi from 2011 to 2020. After taking some factors into account, such as testing cost, efficiency, and capacity, 9 approximately 1 million cytology samples from local health departments and hospitals have been delivered to and tested by an independent clinical laboratory (ICL) since 2012, based on cooperation contracts. Two other independent gene laboratories participated in the Guangxi CC screening project. However, they mainly performed HPV diagnosis. This study is based on the data from the ICL. The sources of cytology samples included the NCCSP and PE programmes of 105 counties, which represent approximately 94.5% (105/110) of Guangxi. Samples from the remaining five counties were tested by local hospitals but were excluded as the data were not shared. Although not all samples were included, the study still covered a statistically representative sample of CC screening.
Many studies have reported the incidence of CC based on data from the NCCSP in China, and this condition primarily affects females aged 35 to 64 years. However, only a limited number of studies have focused on populations at a high risk of CC in minority areas, such as Guangxi, which is the only ethnic minority autonomous region in South China. In addition to NCCSP samples, PE samples were included in this study. Compared with NCCSP, the main target population of PE is urban females. This paper aims to analyse the positive rates of low-grade (LSIL) and high-grade (HSIL) squamous intraepithelial lesions, and CC, and identify groups at high risk for CC in Guangxi.
Materials and methods
Study population
This study was based on data from the laboratory database system (LDS) of an ICL in Guangxi. LDS is a data management platform that is used to collect and manage information on samples, including test methods, cytology types, diagnosticians, and diagnoses.
The NCCSP samples included in the study met the inclusion and exclusion criteria. The following inclusion criteria were employed: 1) The type of cytology sample was a liquid-based cytology cervical smear, and the date of diagnosis ranged from January 1, 2012 to October 31, 2019. 2) The origin of cytology samples was NCCSP in Guangxi. 3) Cytology samples had a defined cytopathology diagnosis. The exclusion criteria were as follows: 1) cytology samples obtained from other projects, 2) cytology samples from other provinces, and 3) unqualified cytology samples or without defined diagnosis.
PE samples included in the study met the inclusion and exclusion criteria. The inclusion criteria were as follows: 1) the type of cytology sample was liquid-based cytology cervical smear, and the date of diagnosis was from January 1, 2012 to October 31, 2019. 2) The origin of cytology samples was PE in Guangxi. 3) Cytology samples should qualify and have defined cytopathology diagnosis. The exclusion criteria were as follows: 1) cytology samples obtained from projects other than PE, 2) cytology samples from other provinces, and 3) unqualified cytology samples or samples without a defined diagnosis (Figure 1).
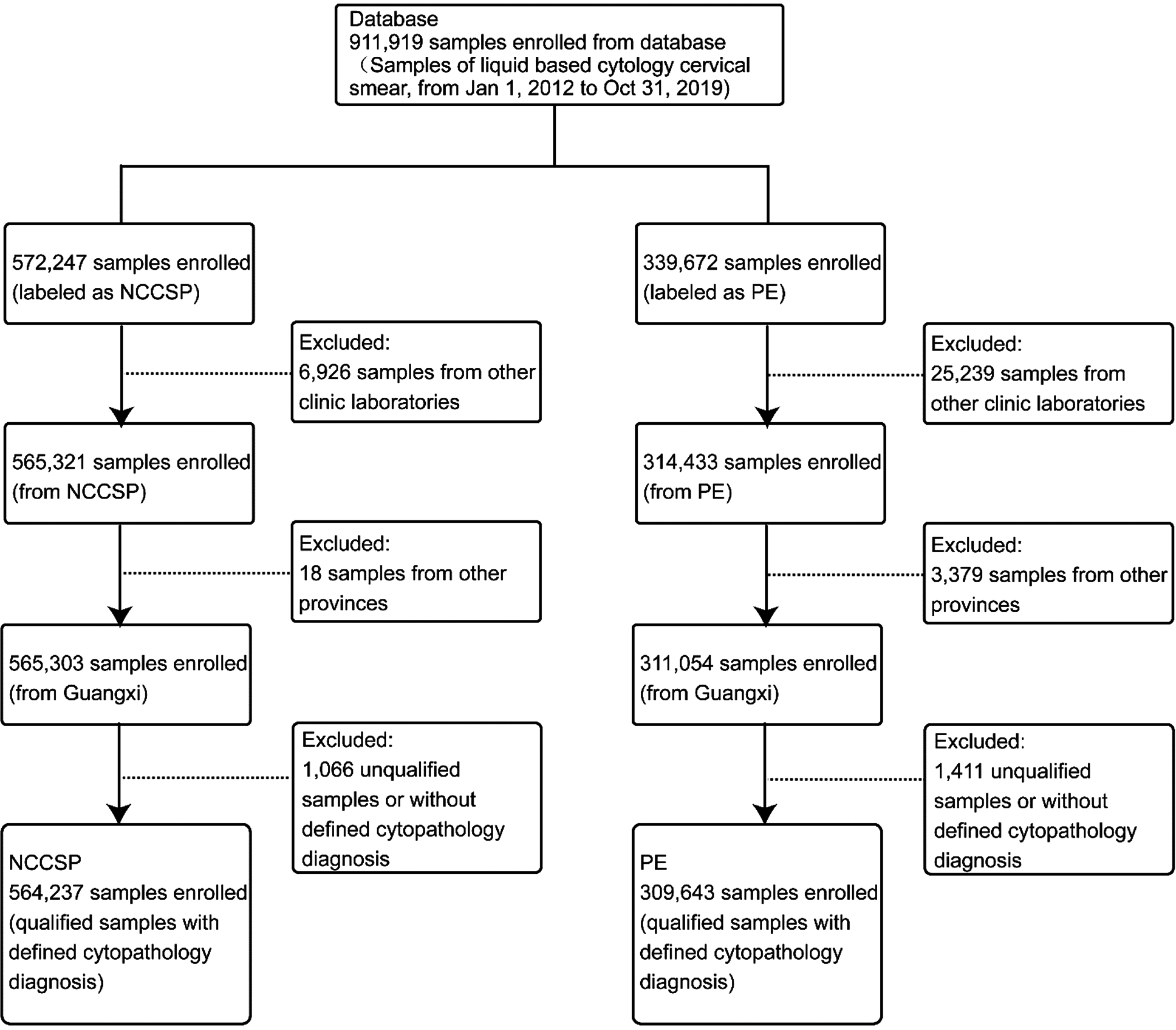
Flowchart of sample inclusion and exclusion criteria. PE: Physical examination; NCCSP: National cervical cancer screening project.
Study variables
Diagnoses of cytological testing of cervical cells were classified into the following types based on the Bethesda System for reporting cervical cytology 10 : 1) atypical squamous cells encompassing cells of undetermined significance (ASC-US) and not excluding HSIL (ASC-H); 2) LSILs encompassing HPV/mild dysplasia / cervical intraepithelial neoplasia (CIN) 1; 3) HSIL encompassing moderate and severe dysplasia, carcinoma in situ, CIN 2 and CIN 3; and 4) squamous cell carcinoma.
The characteristics of the samples were defined as based on the following subgroups for rate calculations: 1) districts (urban or rural); 2) GDP 11 (< 6228.0 USD$ per year or ≥ 6228.0 USD$ per year based on the average exchange rate of renminbi against dollars (6.8985 to 1) in 2019); 12 3) minority status (minority or non-minority areas); 4) geography (coastal or inland areas); 5) sample source (NCCSP or PE); and 6) age (< 35, 35–49, 50–64, or > 64 years).
Statistical analysis
Sample structures (encompassing detection time and other variables—see Table 1) between PE and NCCSP were compared by chi-square testing, and the positive rates of LSIL, HSIL, and invasive cancer were calculated according to age stratification. Adjusted odds ratios (aORs) and 95% confidence intervals (95% CIs) of variables were calculated using the multivariate logistic regression model. Considering the structural difference between PE and NCCSP (Table 1), sample origin (PE or NCCSP) was controlled for covariables in the multivariate logistic regression model. All statistical procedures of this paper were performed using IBM SPSS statistic version 22; statistical approaches and procedures were recorded as syntax of SPSS for review. Graphs were generated using draw.io version 14.4.3. The level of significance was set at α = 0.05.
Sample characteristics of CC screening tested by ICLs in Guangxi, China, 2012–2019. a
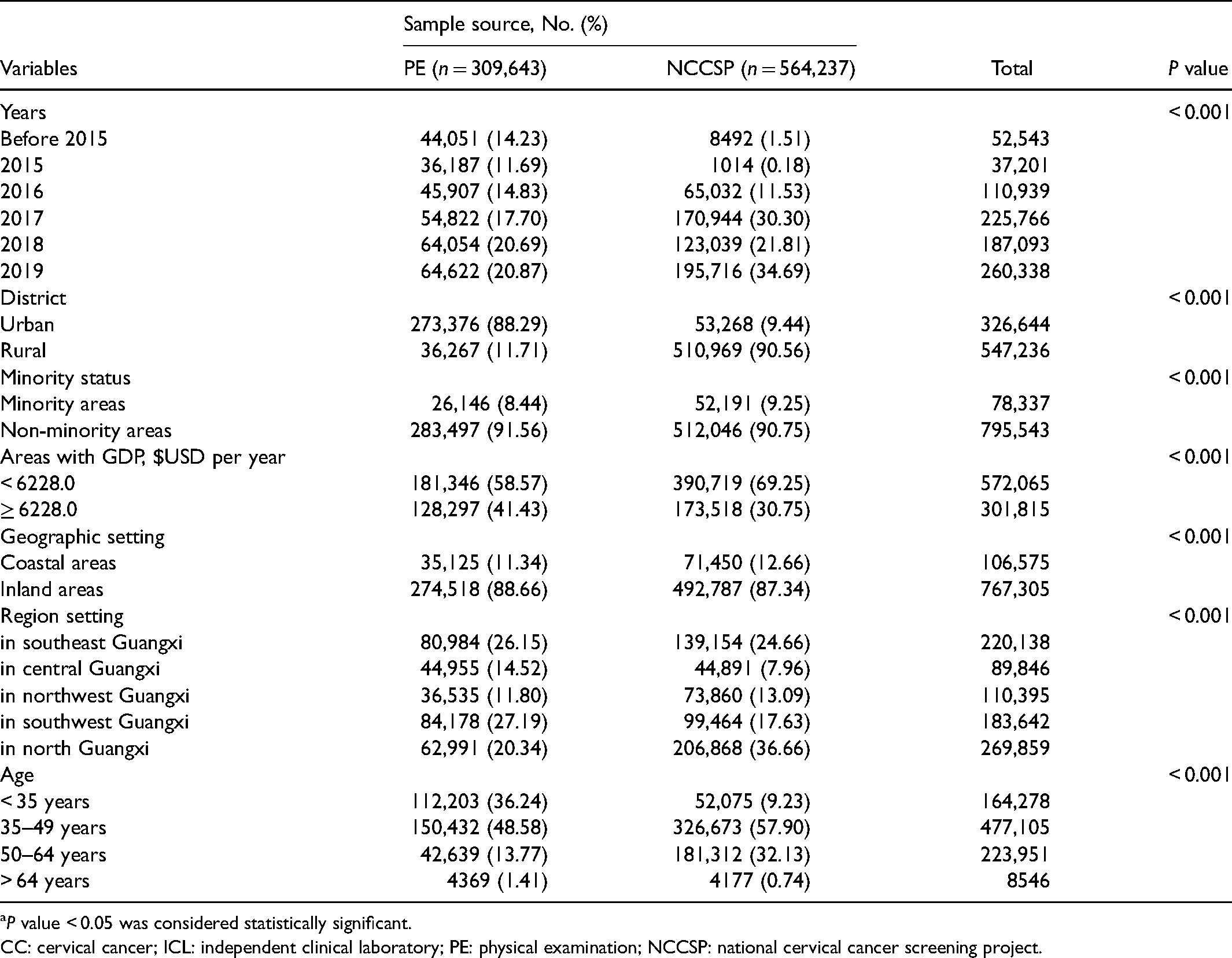
P value < 0.05 was considered statistically significant.
CC: cervical cancer; ICL: independent clinical laboratory; PE: physical examination; NCCSP: national cervical cancer screening project.
Results
Characteristics
A final total of 873,880 samples were included in the study, and the PE and NCCSP sample groups included 309,643 and 564,237 individuals, respectively (Table 1). The average age of women receiving PE services was 39.00 ± 10.29 years, which was younger than that of women involved in the NCCSP (45.26 ± 8.83 years, P < 0.001). The sample structures of PE and NCCSP were different, and the proportions of patients aged 35 to 64 in the two groups were 62.35% and 90.03%, respectively. A total of 88.29% of the PE samples were collected from urban areas, and 90.56% of the NCCSP samples were obtained from rural areas (P < 0.001). The proportions of samples from non-minority areas, inland areas, and areas with GDP ≥ 6228.0 (USD$ per year) in the PE group were 91.56%, 88.66%, and 41.43%, respectively. These values were greater than those noted in the NCCSP group (90.75%, P < 0.001; 87.34%, P < 0.001; and 30.75%, P < 0.001, respectively) (Table 1). The PE and NCCSP sample sizes from 2012 to 2019 are presented in Figure 2.
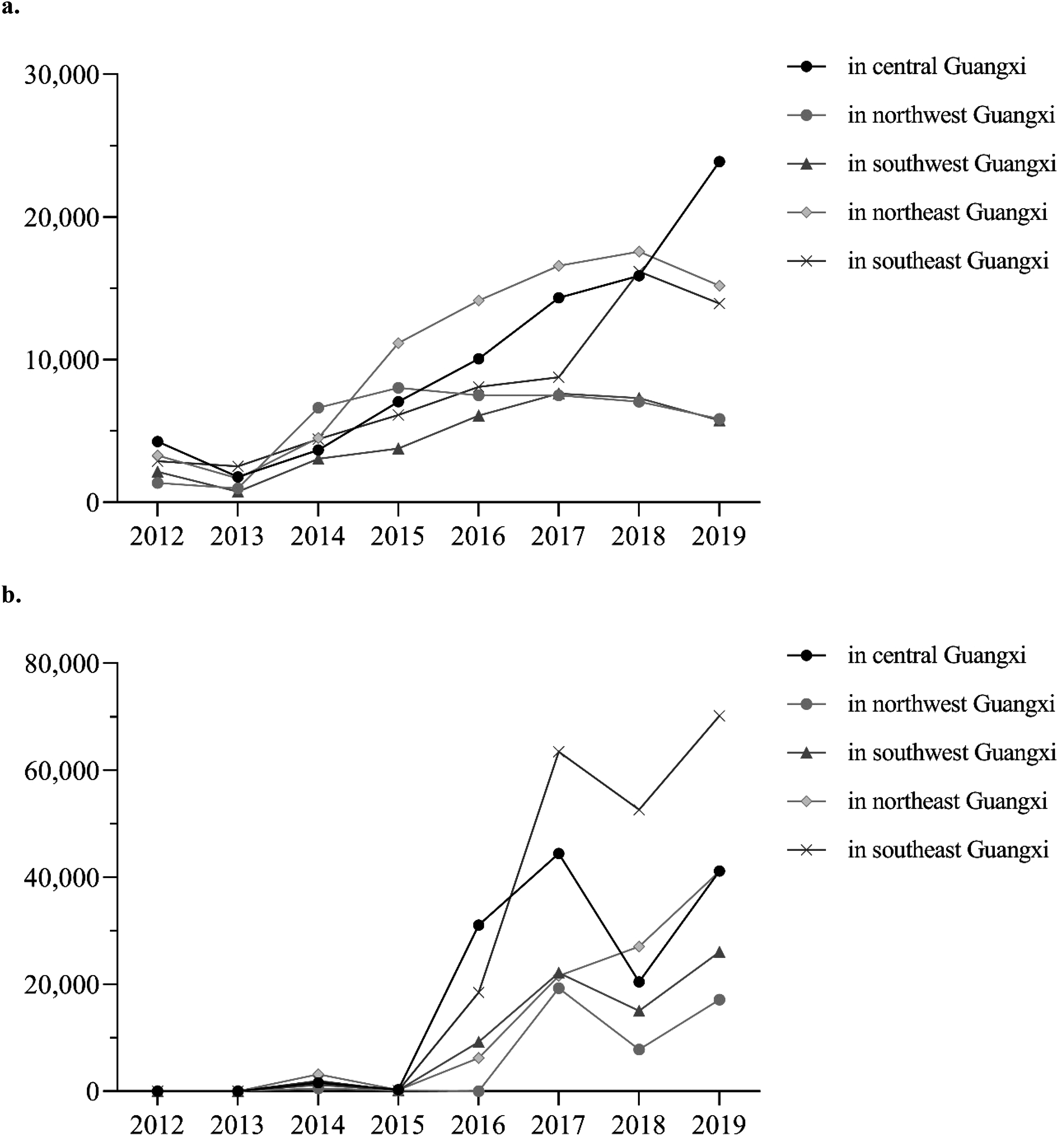
Annual sample size for (a) PE and (b) NCCSP in guangxi zhuang autonomous region from 2012 to 2019. The total sample size for PE was 309,643, and for NCCSP was 564,237. PE: Physical examination; NCCSP: National cervical cancer screening project.
Positive rates
The positive rates of LSIL, HSIL, and invasive cancer in all 873,880 participants were 1.89% (16,500/873,880), 0.60% (5262/873,880), and 0.03% (247/873,880, 28.26/100,000), respectively. The positive rates in the PE samples were 2.32% for LSIL (7184/309,643), 0.78% for HSIL (2417/309,643), and 0.05% for invasive cancer (142/309,643). These values were greater than those noted in NCCSP samples (1.65% for LSIL [9316/564,237], 0.50% for HSIL [2845/564,237], and 0.02% [105/564,237] for invasive cancer). The results were stratified by age (Table 2).
Comparison of the positive rates of LSIL, HSIL, and invasive cancer identified by PE or the NCCSP. a
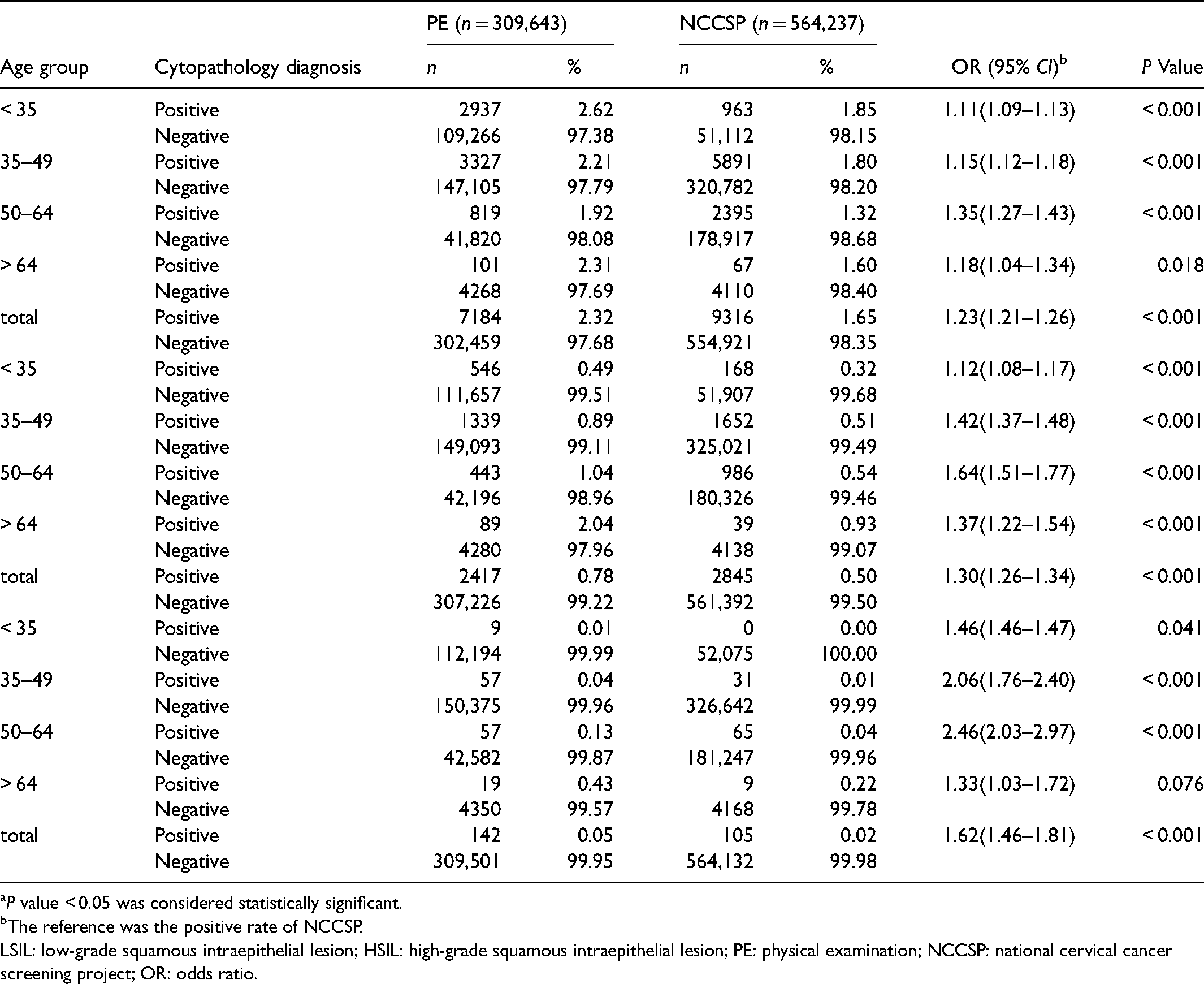
P value < 0.05 was considered statistically significant.
The reference was the positive rate of NCCSP.
LSIL: low-grade squamous intraepithelial lesion; HSIL: high-grade squamous intraepithelial lesion; PE: physical examination; NCCSP: national cervical cancer screening project; OR: odds ratio.
High-risk population
The variable “sample source” (samples from NCCSP or PE) was controlled for covariables, and other significant variables in single factor analysis were entered into the multivariate logistic regression model. The results showed that females from coastal areas (vs. inland areas; aOR = 0.90; 95% CI, 0.86–0.95; P < 0.001) were significantly associated with a low risk of LSIL. Urban areas (vs. rural; aOR = 1.23; 95% CI, 1.19–1.27; P < 0.001), age < 35 years (vs. 50–64; aOR = 1.54; 95% CI, 1.50–1.62; P < 0.001), 35–49 years (vs. 50–64; aOR = 1.33; 95% CI, 1.27–1.38; P < 0.001), and > 64 years (vs. 50–64; aOR = 1.30; 95% CI, 1.12–1.53; P = 0.001) were significantly associated with a high risk of LSIL (Table 3).
Positive rates and multivariate logistic regression for LSIL. a
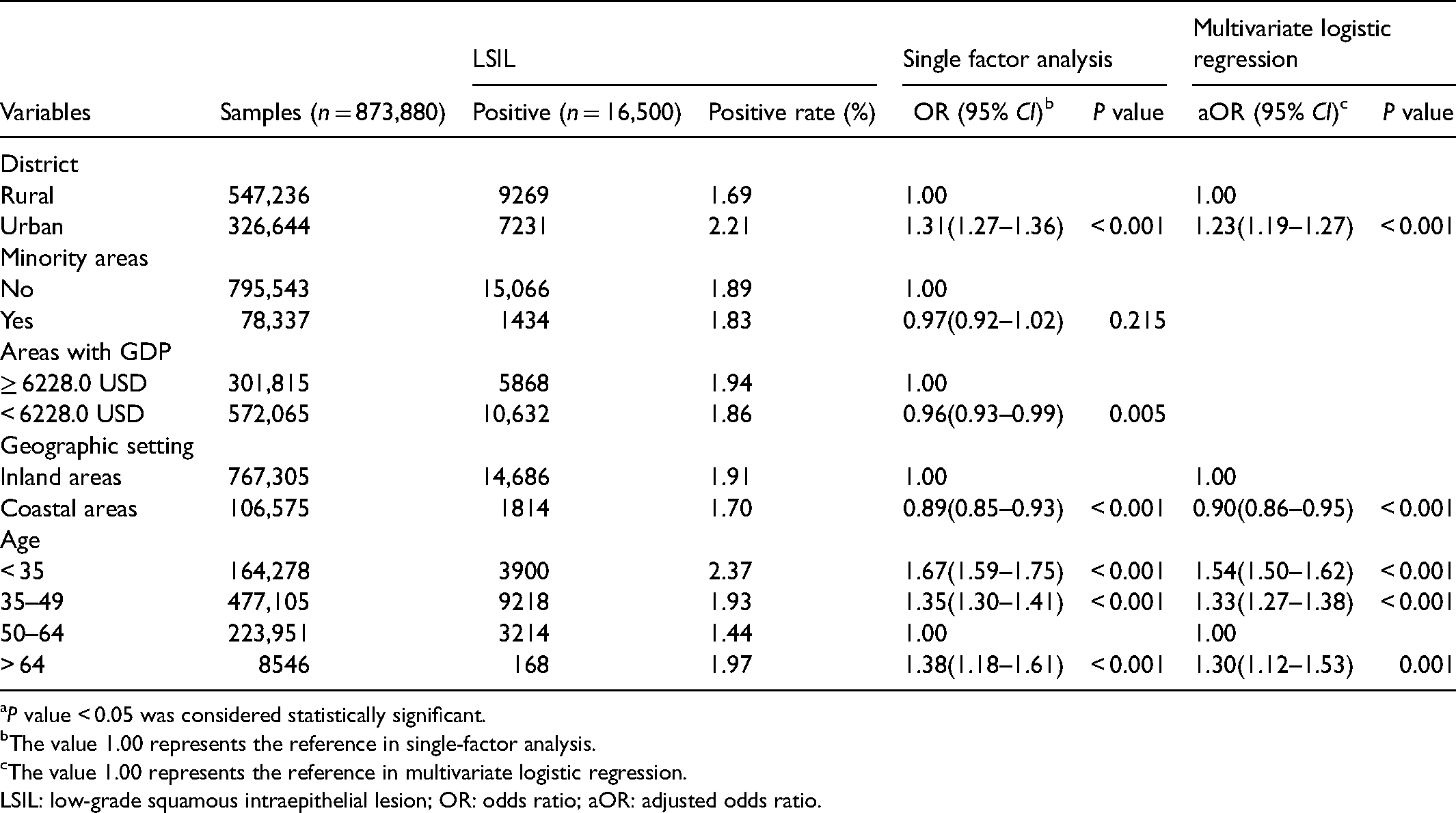
P value < 0.05 was considered statistically significant.
The value 1.00 represents the reference in single-factor analysis.
The value 1.00 represents the reference in multivariate logistic regression.
LSIL: low-grade squamous intraepithelial lesion; OR: odds ratio; aOR: adjusted odds ratio.
Females aged over 64 (vs. 50–64; aOR = 2.05; 95% CI, 1.71–2.46; P < 0.001) and females from urban (vs. rural; aOR = 1.66; 95% CI, 1.57–1.76; P < 0.001), minority (vs. non-minority; aOR = 1.24; 95% CI, 1.13–1.35; P < 0.001), and coastal (vs. inland; aOR = 1.15; 95% CI, 1.06–1.25; P = 0.001) areas were associated with a high risk of HSIL. Females under 35 (vs. 50–64; aOR = 0.57; 95% CI, 0.52–0.62; P < 0.001) were associated with a low risk of HSIL (Table 4).
Positive rates and multivariate logistic regression for HSIL. a
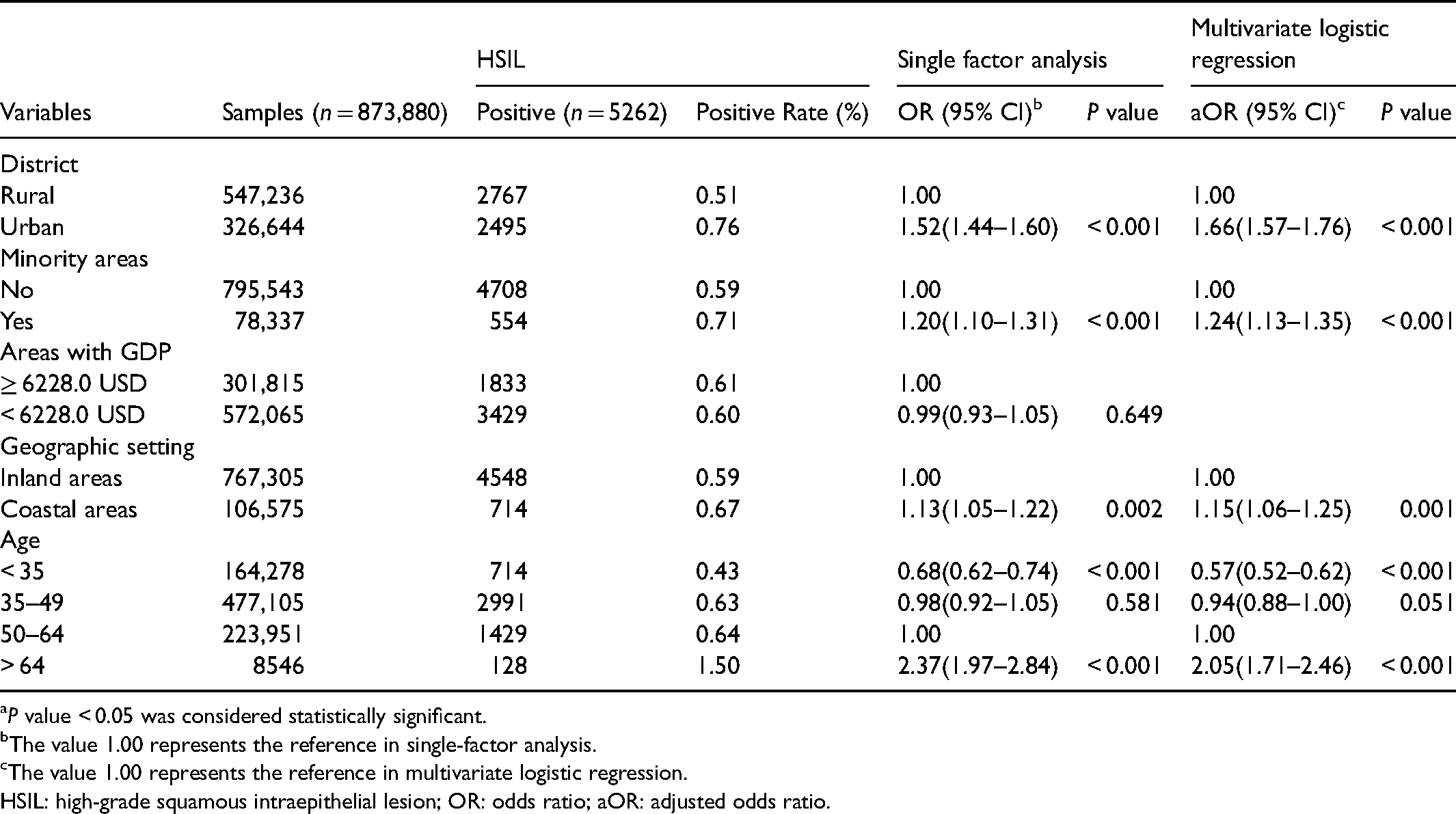
P value < 0.05 was considered statistically significant.
The value 1.00 represents the reference in single-factor analysis.
The value 1.00 represents the reference in multivariate logistic regression.
HSIL: high-grade squamous intraepithelial lesion; OR: odds ratio; aOR: adjusted odds ratio.
Females over 64 (vs. 50–64; aOR = 4.37; 95% CI, 2.88–6.63; P < 0.001) and females from urban areas (vs. rural; aOR = 3.05; 95% CI, 2.36–3.95; P < 0.001) were significantly associated with a high risk of invasive cancer. Females under 35 (vs. 50–64; aOR = 0.07; 95% CI, 0.03–0.13; P < 0.001) and 35–49 (vs. 50–64; aOR = 0.30; 95% CI, 0.23–0.40; P < 0.001) were significantly associated with a low risk of invasive cancer (Table 5).
Positive rates and multivariate logistic regression for invasive cervical cancer. a
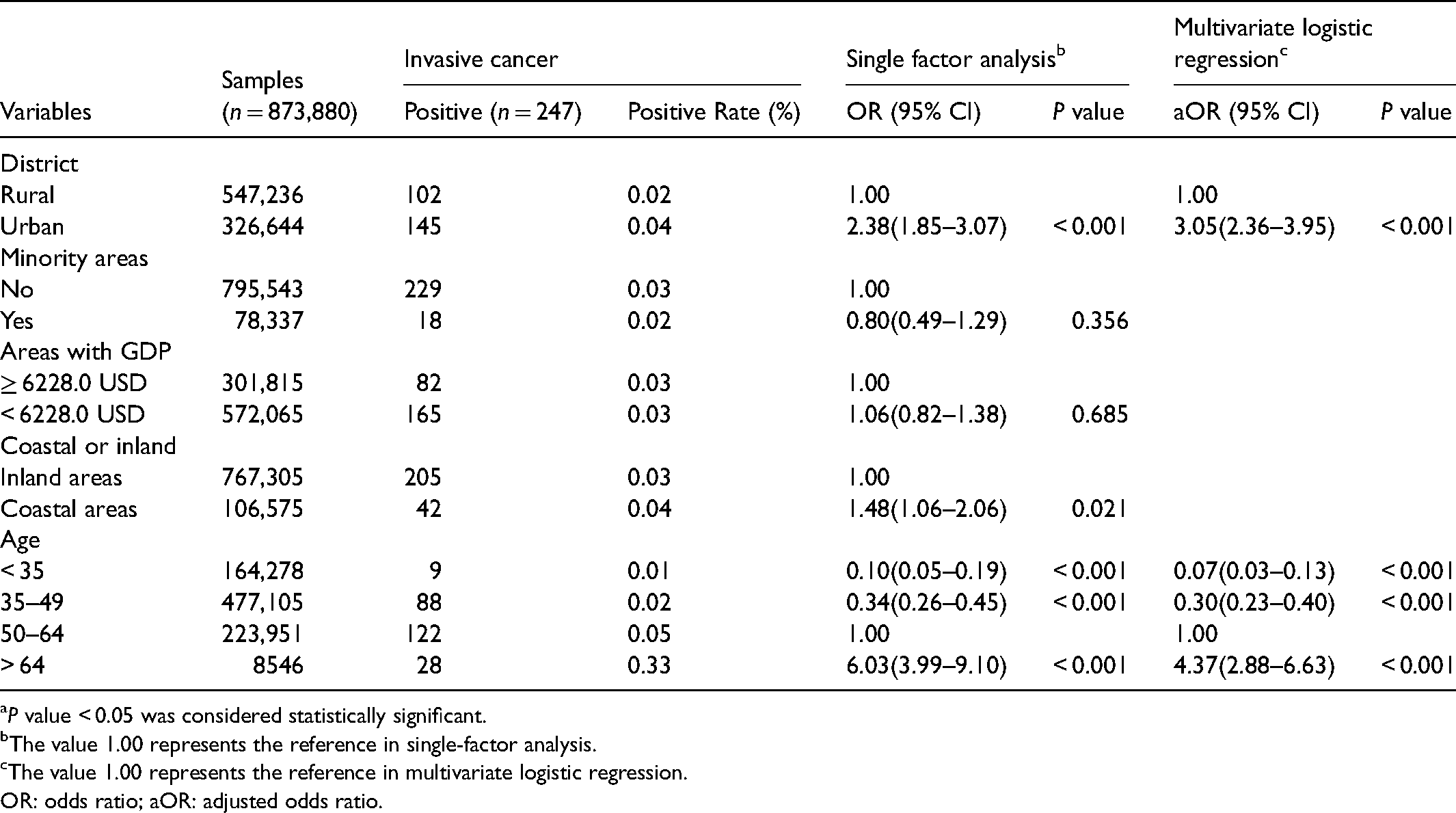
P value < 0.05 was considered statistically significant.
The value 1.00 represents the reference in single-factor analysis.
The value 1.00 represents the reference in multivariate logistic regression.
OR: odds ratio; aOR: adjusted odds ratio.
Discussion
Guangxi is the only ethnic minority coastal province in South China; it has a relatively weak economy and borders northern Vietnam. The ethnic structure of Guangxi is relatively complex, with Han, Zhuang and Yao accounting for 62%, 31% and 3%, respectively. The remaining ethnic minorities account for approximately 4% of the population. Guangxi is home to the largest Zhuang and Yao populations. Similar to other developing areas,13,14 the trend of increasing mortality from CC puts an increasingly heavy burden on individuals, families, and the country.7,15 This study found that the positive rate of CC in Guangxi was 28.26/100,000, which was higher than that reported in previous studies in China (13.30/100,000) 16 but lower than that reported in Guangdong (45.03/100,000), a developed province located in southeastern Guangxi. 17
Females aged 35–64 were the main target population of the NCCSP, and this population was associated with a higher risk of CC than younger females in this study. Similar results were noted in a previous study in China. 18 We found that females over 64 were associated with a significantly higher risk of CC than females aged 50–64 (the main target population of the NCCSP). The Chinese National Cancer Center also estimated a high incidence rate in elderly females in China 19 and suggested that CC screening should include those aged 65 and older. 20
We found that urban females in Guangxi were associated with a high risk of CC, similar to previous studies describing the incidence of CC in urban and rural areas.21–23 Previous studies suggested that urban females have more sex partners and first intercourse at a younger age than rural females. 24 These sexual behaviours are risk factors for CC. 25 Some studies conducted in developed countries suggested a high incidence of CC in rural females and ethnic minority populations. 26 In this paper, ethnic disparities in HSIL were observed. In contrast, spatial and economic condition disparities of CC have been reported worldwide.27,28 We found that low economic conditions were not a risk factor in this study. We hypothesize that although Guangxi is a developing region with low economic conditions, the regional economic differences among counties in Guangxi are not as large as those reported in previous studies between developed and developing countries.
The positive rate of HSIL (0.60%) in Guangxi was higher than that reported in recent studies (0.48%–0.56%) in China29–31 but lower than that reported in other developing counties or areas.31,32 Notably, this study was based on cervical cytological results rather than histological results, which is similar to some population-based studies on CC screening. In this study, we found that being female over 64 and being from an urban area were common risk factors for CC and HSIL. We also discovered that the 35–49 and 50–64 age groups had similar HSIL risks. CC screening showed high value in the early detection of HSIL in the target population. Previous studies have reported a strong relationship between HSIL and cancers,33–35 particularly CC and anal cancer.36–38 We should focus on these populations at high risk for CC and HSIL in Guangxi.
Notably, the urban female population is not yet covered by the NCCSP in Guangxi, but the NCCSP allows these females to self-pay for CC testing. However, compared with the periodic check-up for rural females in the NCCSP, PE appears to be an ideal screening method for most urban females. In addition, some urban female workers can have regular check-ups paid for by employers. Regular check-ups may help with the early detection of HSIL, and potentially give more opportunities to control or interrupt its progression through appropriate treatments.39,40 The main purpose of this screening is to identify CC patients early, to save lives, and to improve quality of life.41,42 This paper identified populations in Guangxi at high risk for CC. This finding suggests that if we pay more attention to the high-risk population, then clinicians have more opportunities to identify potential patients and treat them at early stages.43,44
In minority areas, the natural environment may be harsh and the economic level can be low because of traditional customs, lifestyle, and culture. The low coverage rate of CC screening, high prevalence of STIs and tuberculosis,and late detection of HIV/AIDS in Guangxi may indicate certain obstacles to the implementation of public health services, especially in undeveloped minority areas, despite the similar expected standards of medical care and services at the county level.45–47 Our results suggest that health departments should actively mobilize urban women to participate in CC screening in their early 60 s to identify HSIL and cancer patients at an early stage. Surveys of target populations in low coverage areas are conducive to exploring possible barriers to CC screening.48,49 Targeted campaigns in the local language can promote awareness of women's health, which has a positive effect on CC screening. 50
This paper has the following limitations. 1) Given differences in the serial numbers of HPV and liquid-based cytological samples, we did not incorporate the HPV results into this study. 2) Given the significantly different features between PE and NCCSP, the sample source was included in the multivariate regression model as a covariate. Therefore, the source could not be considered a potential variable in risk analysis. 3) Both NCCSP and PE samples may contain a small number of patients with HSIL who require regular follow-up examination. Approximately 1.7% of HSIL patients are estimated to undergo repeat CC screening in follow-up visits, and the positive rate of HSIL may be overestimated.
Despite these limitations, there are also some strengths. Many studies have focused on CC screening in China. However, the majority were based on the NCCSP, and our study is based on data from a large sample of the NCCSP and PE. This paper expounds on the positive rates of LSIL, HSIL and CC in Guangxi, thereby identifying high-risk populations and providing evidence for public health strategy developers.
Conclusion
Our study revealed that females from urban areas are at high risk for CC and HSIL in Guangxi. We suggest that public health strategies must focus on these high-risk populations.
Footnotes
Acknowledgments
We thank Dr Fengting Huang, Liying Ou, Jianyun Lan, Xiaoxia Li and colleagues at cytopathology diagnosis department of Guangxi Kingmed diagnostics group for supporting our study. All authors in the study provided important contribution and revision of the manuscript.
Ethics approval
This study protocol was approved by the Ethics and Human Subject Committee of Guangxi Medical University and Guilin Medical University (No.20180702-3).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by the National Natural Science Foundation of China [grant No.81560523 and 81760577], the Guangxi Science and Technology Development Project [grant No.AD17129003, No.14124005-2-11], the Fundamental Research Funds for Young and Middle-aged Teachers by the Education Department of Guangxi government [grant No.KY2016YB076], the Innovation Project of Guangxi Graduate Education (grant No. YCBZ2020052), Guangxi Scholarship Fund of Guangxi Education Department of China. Young Researchers Science Foundation Program of Guangxi Medical University (grant No. GXMUYSF201814).