
Abstract
Objective
Breast and cervical cancers are screen-detectable; yet, challenges exist with ensuring uptake of mammography and Pap smear. Family, a central factor in developing knowledge to carry out health promotion behaviors, may be an asset to improving intention to screen among non-adherent women from underrepresented minority groups. We explored familial cancer; communication; and breast and cervical screening intention among non-adherent Black, Latina, and Arab women in the United States who participated in a randomized controlled trial of the Kin KeeperSM Cancer Prevention Intervention study. The intervention was a culturally-targeted breast and cervical cancer literacy tool for Black, Latina, and Arab women, consisting of two family-focused education sessions on the cancers, their screening guidelines, and risk-reducing health-related behaviors.
Methods
For this secondary analysis, we assessed family cancer history, family communication, and screening intention for breast and cervical cancer in age-eligible, non-adherent participants. Descriptive statistics examined sample characteristics of the intervention and control groups. Odds ratios were estimated from logistic regression modeling to assess the intervention and sample characteristic effects on screening intention.
Results
Of the 516 participants, 123 and 98 were non-adherent to breast and cervical cancer screening, respectively. The intervention (OR = 1.95 for mammography; OR = 1.62 for Pap smear) and highly communicative (OR = 2.57 for mammography; OR = 3.68 for Pap smear) families reported greater screening intention. Family history of cancer only increased screening intention for mammography (OR = 2.25).
Conclusion
Family-focused approaches supporting communication may increase breast and cervical cancer screening intention among non-adherent, underrepresented minority groups.
Introduction
In 2014, in the United States, Black and Latina women accounted for about 20% (46,625) of those diagnosed with breast cancer and 22% (9048) of those who died. 1 Black and Latina women accounted for about 30% (3848) of those diagnosed with cervical cancer and 32% (1330) of those who died. 1 Due to reporting procedures, there was no indication of the burden of disease among Arab women. Black women, unlike Latinas and Arabs, are slightly more adherent to breast (mammography) and cervical (Pap smear) cancer screening guidelines than Whites. 2 Rationale for adherence among Black women comes despite having lower health literacy than Whites. 3 Understanding perceptions that lead to screening uptake among underrepresented minority groups may explain this phenomenon and indicate areas to improve reach to women who are non-adherent to breast and cervical cancer screening.
Cancer screening is a health promotion behavior. Similar to the case with Black and Latina women, screening among Arab women is linked to perceptions of cancer, motivation, and barriers.4–6 The family is a central factor in developing knowledge to carry out health promotion behaviors.7–9 Families are sources of information, behavioral habits, and genetic predispositions. 10 In kind, the established trust among families serves as a resource to reinforce health-based education within the cultural context. Thus, including a family focus in intervention research may improve adherence to recommended breast and cervical screening guidelines. 11
Opportunity presents itself to study women and their female family members who have connections to the healthcare system but are non-adherent to breast and cervical screening guidelines. Intention to be screened is a known predictor of screen completion. 12 Here, we explore the family history of cancer; communication; and breast and cervical screening intention among non-adherent Black, Latina, and Arab women.
Methods
Data are derived from the Kin KeeperSM Cancer Prevention Intervention trial (described in detail elsewhere). 13 This randomized controlled trial tested the culturally targeted Kin KeeperSM intervention designed to improve breast and cervical cancer literacy as well as increase health-related behaviors among Black, Latina, and Arab women. Delivered by community health workers, the intervention utilized the network of primary participants (intervention group or control group) to educate women in at-home group settings in Michigan (N = 516). 13 Findings from the parent study indicate that the intervention improved cancer literacy across racial and ethnic groups. 14 Baseline data identified associations between family communication, literacy, and perceived health status; 15 however, associations with cancer history and such end-points have not been previously examined. Further, explaining associations in non-adherent women informs future research to increase adherence.
For the purpose of this study, we extracted study participants who reported being non-adherent (at baseline) to breast (N = 128) and cervical screening guidelines (N = 98). We examined associations of family communication and family cancer history with future screening intention among study participants. Non-adherence to breast cancer guidelines was defined as women aged 40–74, who had never had a mammogram, or had not had a mammogram within 12 months. Non-adherence to cervical cancer screening guidelines was defined as women aged 21–65, who had never had a Pap smear, or had not had a Pap smear within three years. Definitions for screening non-adherence were based on American Cancer Society and U.S. Preventive Services Task Force (USPSTF) recommendations of 2002, which were up-to-date at the time of study design.16–18 The following describes measures used in this analysis.
Sociodemographic questionnaire
A 56-item sociodemographic questionnaire allowed participants to self-report their descriptive information (e.g. age, race/ethnicity, health status, screening behavior, family history of cancer, and insurance).
Family Adaptability and Cohesion Scale
The FACES IV assessed six scales of family cohesion (disengaged to enmeshed with family involvement) and flexibility dimensions (rigid to chaotic in managing familial problems) which are central to family communication and satisfaction in the Circumplex Model of Marital and Family Systems.19,20 We calculated the total ratio score, then dichotomized the score into a high or low variable. High scores indicated a high level of self-reported communication between family members. FACES IV has high internal consistency (Cronbach α = .77–.89). 21
Screening intention
The Action Plan assessed participant’s self-reported goals or intent to access breast and cervical cancer screening. The intent to screen was indicated by answering “yes” to any of the following responses: (1) plan to find a healthcare provider to do first-ever screening; (2) schedule first-ever screening; or (3) continue getting yearly screening within twelve months. Screening refers to mammogram for breast cancer screening and Pap smear for cervical cancer screening.
Analysis
Descriptive statistics were used to summarize sample characteristics for non-adherent women, stratified by group (intervention vs. control). We calculated the proportion of women who had intent to screen in 12 months by intervention and sample characteristics. Unadjusted odds ratios and adjusted odds ratios were estimated from logistic regression modeling to examine the effect of intervention and sample characteristics on the future intent to screen. Each factor was entered into the model separately in unadjusted analyses. In adjusted analysis, all factors were included as predictors simultaneously in a multiple logistic regression model to examine the effects, adjusting for other factors in the model. We used effect sizes to guide the interpretation of odds ratios (ORs) from the logistic regression models, using OR = 1.68, 3.47, and 6.71 (or OR = 0.60, 0.28, and 0.15 for ORs less than one) as cutoffs for small, medium, and large effect sizes. 22 All tests were two-sided with a significance level of 0.05 and were conducted using SAS version 9.4. 23
Results
Of the 516 Kin KeeperSM trial participants, 123 (Black – 39.0%; Latina – 15.4%; Arab – 45.5%) reported non-adherence to the published guideline for mammography (yearly after age 40) and 98 (Black – 26.5%; Latina – 16.3%; Arab – 57.1%) reported non-adherence to the guideline for Pap smear (every three years) exams. Table 1 summarizes the sample characteristics. For mammography, we found that the intervention group was younger (p = 0.033) with a trend for higher likelihood of being un-partnered (p = 0.097), employed (p = 0.069), and insured (p = 0.083) than the control group. For Pap smear, the racial/ethnic make-up of the groups showed a marginally significant difference (p = 0.068). Compared to the control group, the intervention group had more African Americans (33.8% vs. 12.1%) and fewer Arab Americans (50.8% vs. 69.7%).
Sample characteristics: mammography group (N = 123); Pap smear group (N = 98).

aChi-square tests were used to test the difference between intervention and control in sample characteristics.Bolded p-values indicate a significant finding that is < 0.05.
A vast majority of the women had intent to receive the screening within 12 months (87.8% for mammography; 90.8% for Pap smear). Table 2 shows the unadjusted and adjusted effects of the Kin KeeperSM trial intervention and sample characteristics of having intent to receive mammography and Pap smear screening. After adjusting for potential confounders (age, race/ethnicity, marital status, education, employment, and insurance), multiple logistic regression analyses revealed that women who received the Kin KeeperSM intervention (OR = 1.95 for mammography; OR = 1.62 for Pap smear) and women in highly communicative families (OR = 2.57 for mammography; OR = 3.68 for Pap smear) reported greater screening intention. Lower education (OR = 1.86 for mammography; OR = 6.75 for Pap smear for ≤high school vs. higher education ≥ some college) and older age were associated with higher likelihood of having screening intention as well. Being employed and having insurance were associated with less likelihood of intent to screen for mammography (OR = 0.35 and 0.19, respectively) in 12 months, but were not associated with intent to screen for Pap smear in 12 months (OR = 1.27 and 0.89, respectively). Family history of cancer increased screening intention for mammography (OR = 2.25); however, family history was not associated with screening intention for Pap smear (OR = 0.92). Women who had a history of mammography or Pap smear screening had lower intent to screen (OR = 0.67 for mammography; OR = 0.20 for Pap smear) compared to those who had never received screening before.
Effects on screening intention: mammography within 12 months (N = 123); Pap smear within three years (N = 98).
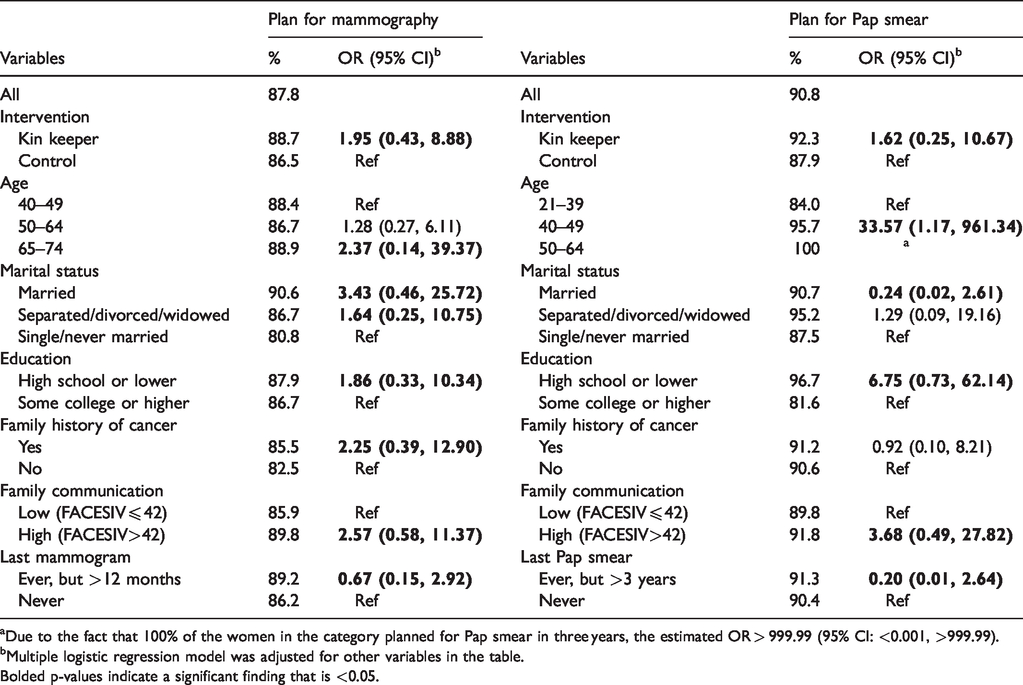
aDue to the fact that 100% of the women in the category planned for Pap smear in three years, the estimated OR > 999.99 (95% CI: <0.001, >999.99).bMultiple logistic regression model was adjusted for other variables in the table.Bolded p-values indicate a significant finding that is <0.05.
Discussion
The presentation of breast and cervical cancer continues to disproportionately affect women of color in the United States, despite their screening behaviors. Arab women, who are most often classified as White, have been medically underserved based on their socioeconomic and immigration status. They accounted for half of those who reported being non-adherent to breast or cervical cancer screening. Arab women remain a community that is under-represented in research and clinical care. Use of community health workers, and/or a member of the family, can encourage participation in research and create access to cancer education that may improve screening intention.15,24 Further, cultural barriers for timely initiation of cancer screening may be averted with increased education.
With the use of our extensive sociodemographic questionnaire, we captured data on family history of cancer and encouraged women to discuss this history among themselves. Family history of cancer was significant for intent for mammography screening in this study. This finding aligned with that from our previous study, 9 which demonstrated that having a family history of cancer was motivational for mammography screening in Black women. However, our study found no significance between family history of cancer and Pap screening intent, contrary to the results of our query of the 2000 National Health Interview. 25 This may be related to low health literacy on the intent for Pap smear screens to identify cervical cancer, which may be related to the lower incidence of cervical cancer in comparison to that of breast cancer. In a multiethnic study (including Blacks and Latinas), familial cancer history increased the odds of getting screened. 26 This study offers a plausible argument that family communication is associated with screening intention, which may also be true of other women outside of the United States who share heritage and culture with women from these racial and ethnic groups.
As illustrated here, facilitating family communication can improve screening intention. While mass multimedia messaging is an effective and easily disseminated way to promote healthful behaviors like cancer screening, this raises questions about who is receiving the messaging as intended and do they have trouble understanding guidelines or risk.27,28 Capitalizing on family communication of normative cancer screening behaviors has been associated with follow-through in Black and Latina women.5,29,30 This communication offers opportunities to clarify facts related to screening and serves as a reminder to get screened. 31
Quality communication of family health information is critical to leverage healthy behaviors within the home. Communication may be affected by any number of factors. Notably, the more extensive study of these diverse women identified marital status, family composition, and status of health as predictors of communication. 15 One must also consider how families establish routines for healthful behaviors. Many studies have pointed to education as being directly related to establishing healthy behaviors like having cancer prevention screening.26,32–34 However, we found that those with lower educational attainment had higher intention for breast and cervical cancer screening. This chance finding warrants further investigation.
Limitations
This study was a secondary analysis of previously collected data. As such, the self-reported data on intention do not indicate whether or not participants followed through with either screening modality. We also acknowledge that the relatively small sample size of the study resulted in less precise estimates as indicated by the wide confidence intervals and higher likelihood of Type-II error (or, failure to detect true significant findings).
Conclusion
Regardless of the racial or ethnic group, family serves as a positive vehicle to deliver health promotion messages. It presents a trusted environment to communicate complicated topics. Family-focused approaches supporting communication may increase breast and cervical cancer screening intention among non-adherent, underrepresented minority groups. Further work is needed to understand how bolstering family communication can be used to increase cancer prevention screening, particularly among those who have elevated risk of developing cancer due to familial history. Research is also needed to understand the role of general education in cancer prevention screening intention.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded in part by the National Institutes of Health National Institute of Nursing Research 5R01NR011323-05.