
Abstract
Objectives
Body mass index is a strong predictor of post-menopausal breast cancer risk and (negatively) confounds the association between mammographic breast density and breast cancer risk; however, height and weight are not typically measured as part of routine mammographic screening. This study piloted voluntary height and weight measurement within the BreastScreen Western Australia (WA) programme, and assessed trial participation.
Methods
From February 2016 to January 2018, 204,429 women attending BreastScreen WA were invited to have their height and weight measured and recorded as part of their routine screening mammogram. Descriptive data analysis was used to assess pilot participation rates by available screening data.
Results
Of the 204,429 patients who attended BreastScreen WA during the pilot, 76.35% (156,072) agreed to have their height and weight measured. Pilot participation rates were significantly lower in those patients with disabilities (RR: 0.626; 95% CI: 0.600, 0.653), those who spoke a language other than English at home (RR: 0.876; 95% CI: 0.867, 0.885), and those who identified as Aboriginal and Torres Strait Islander (RR: 0.829; 95% CI: 0.807, 0.852). Pilot participation decreased over time from 88.9% in the first three months to 55.5% in the last month, due to lessening of support from BreastScreen staff.
Conclusion
Measuring height and weight at the time of routine mammographic screening is feasible, although logistical issues, particularly the added time/effort required of support staff, should be considered. BreastScreen WA has since decided to collect voluntary self-reported height and weight data as routine screening policy.
Introduction
Most mammographic screening programmes in Australia collect information regarding some known breast cancer risk factors, such as age, family history and hormone therapy use, but not body mass index (BMI). This is despite climbing obesity rates in developed countries, and the known association of increased BMI as a preventable predictor of breast cancer risk, particularly in post-menopausal women. 1 There is also increasing evidence supporting the use of individual breast cancer risk assessment to tailor screening recommendations for groups of women at different levels of risk, 2 and that breast cancer risk prediction models require height and weight information. Also, BMI negatively confounds the strong association between mammographic breast density and breast cancer risk, particularly when using measures of percent density (which is inversely correlated with BMI). 3 Without adjustment for BMI, the association between percent density and breast cancer risk is underestimated, 4 and advocacy for accurate breast density reporting is increasing.5,6 A prospective database of height and weight measures within a breast cancer screening programme could facilitate large scale investigations of the role of BMI and screening outcomes, which would be of both clinical and research value. This study assessed the feasibility of prospectively measuring height and weight as part of routine screening mammography within the BreastScreen Western Australia (WA) programme.
Methods
Equipment and participants
BreastScreen WA is a state-run, publicly funded breast cancer screening programme that provides free screening mammograms to asymptomatic women aged 40 and older, and specifically targets women aged 50 to 74. The programme screens around 120,000 women each year across eleven permanent screening clinics, and four mobile services that visit over 100 outer metropolitan and rural towns every two years. An electronic measuring station that carries out weight and height measurements in a single step was tested in one of the city-based permanent screening clinics. The testing protocol required women to measure themselves at the station and send their results to a printer to attach to their medical record. The test was deemed unsuccessful due to regular technical issues, and additional staff time required to complete the measurements. Digital flat scales and portable wall stadiometers were subsequently installed in each of the mammography rooms/mobile units. Both devices were compact and portable, given space constraints.
All women attending any of the 15 BreastScreen WA services between 25 February 2016 and 31 January 2018 were eligible to have their height and weight measured as part of their routine screening mammogram, and 204,429 women attended the screening programme during this time. There were no exclusion criteria, however, the invitation to have height and weight measured was dependent on a request from the attending BreastScreen reception and radiography staff. BreastScreen staff were also required to assist participants in measuring their height, and to record the measurements manually on the patient medical record.
Study design
For the first five months of the pilot, women were provided with a hard copy information sheet about the pilot ‘trial’ upon arrival for their screening mammogram. The information sheet explained that BreastScreen WA was trialling whether it is possible and appropriate to ask women to measure their height and weight at the time of mammography. Women were told that this information may be useful in the future to improve the effectiveness of breast cancer screening, and were then asked if they would consider having their height and weight measured/recorded. It was explained to the women that participation in the trial was completely voluntary, and that not participating in the trial would not affect their care in any way. Women were instructed to let the staff assisting them know if they would like to participate in the trial. A copy of the information sheet is provided in the online Supplemental Material. All women who attend BreastScreen WA provide written consent, at every screen, to the collection and use of data relating to the screen, subsequent investigations, and treatment, for monitoring, evaluation and research purposes, provided names are not used in any reports or published statistics. During the measuring procedure, women could keep their shoes on and were dressed from the waist down (in their own clothes) in addition to wearing a hospital gown. There was also the opportunity for women to comment on the trial on the reverse side of the information sheet. After five months, a laminated copy of the information sheet was provided to women, to read and return prior to having their mammogram (instead of a hard copy). If women had any comments or feedback about the measurement they were provided with a phone number or instructed to comment on the BreastScreen WA feedback brochure.
A random sample of full-field digital mammograms from 410 women who did not participate in the pilot and 410 age-matched women who had their height and weight measured was extracted from BreastScreen WA’s Picture Archiving and Communication System. Participants were sorted by a random number variable (generated in STATA) and the first 410 participants were selected. An age-matched non-participant was then selected for each participant. The list of IDs for 820 women was provided to BreastScreen WA, where identifying information was reassigned to facilitate total volume measurement by co-author RA. The nipple to chest wall diameter was electronically measured from the cranio-caudal view, to estimate a validated measure of total breast volume. 7 This was to ascertain if overweight women were less likely to participate in having their height and weight measured.
Available data extracted from the BreastScreen WA database included height, weight, age, postcode, family history, screening location (clinic or mobile), country of birth, Aboriginal and Torres Strait Islander status, disability and language interpreter flags, and whether a longer appointment was required. Postcode was used to apply the Australian Bureau of Statistic’s Accessibility/Remoteness Index for Areas and Socio-Economic Indexes for Areas (SEIFA). 8 Remoteness was categorized into five groups: Major city, Inner regional, Outer regional, Remote and Very remote. We used quintiles of SEIFA’s Index of Disadvantage based on relative socio-economic advantage and disadvantage, where the first quintile has the least advantage and most disadvantage.
Statistical analysis
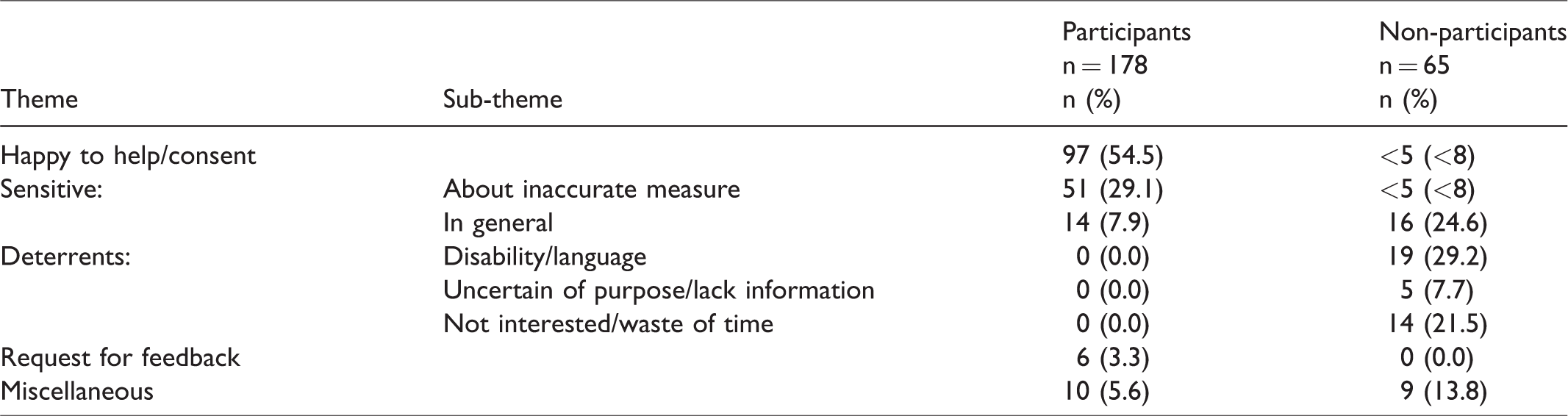
The characteristics of participants and non-participants were described using descriptive statistics. Poisson regression with robust error variance was used to estimate relative risks to investigate the predictors of participation.9,10 Subjects with missing data were excluded from the regression analyses. Results were considered significant at p < 0.05. The reliability of the measurements was investigated using Pearson’s correlation coefficient in those who had had multiple height and weight measurements during the study period. The distribution of height and weight measurements were compared with those from women aged over 35 from the Australian Bureau of Statistics’ National Health Survey, which measured height and weight from a sample of 21,000 people across the Australian population. Of the women who received the hard copy version of the information sheet (approximately 50,000), 243 provided comment on the reverse side. Their responses were analysed thematically through an inductive approach to categorize these into a meaningful framework. 11 Responses were coded to the framework and counted. Illustrative quotes were selected to present each code.
All data management and analyses were completed using Stata v14. All patient data was de-identified before analysis. This study was registered with Royal Perth Hospital Clinical Quality and Safety Unit (no: 13585).
Results
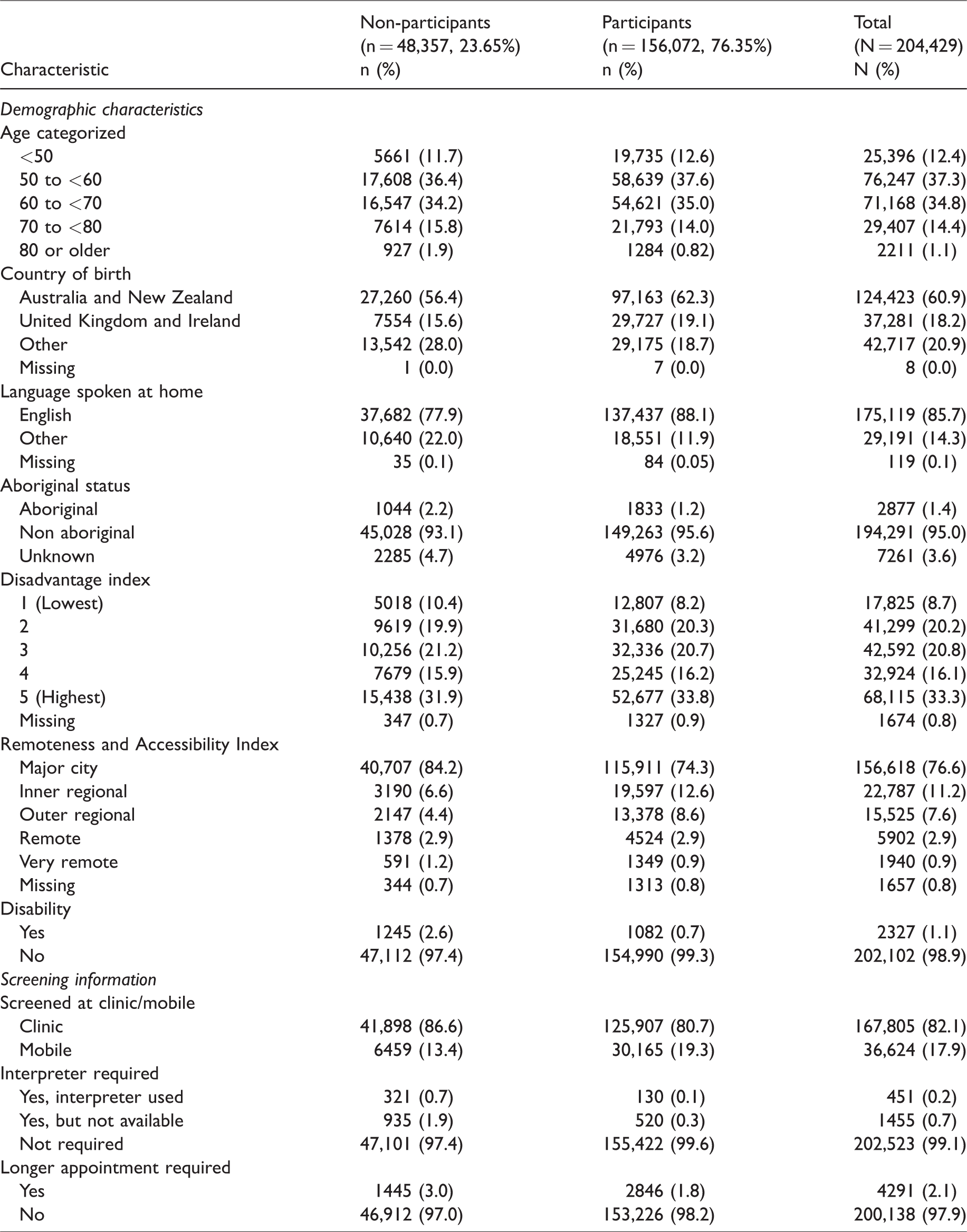
The characteristics of pilot participants and non-participants are shown in Table 1. Of the 204,429 individuals screened during the pilot period, 76% participated in the height and weight measurement collection. Overall, the mean age was 59.8 years, the majority of women were born in Australia or New Zealand (61%), and spoke English (86%) at home. Most women lived in major cities (77%) and had their mammogram at a fixed clinic (82%). Based on postcode, 33% of women lived in higher socioeconomic areas. Pilot participation rates were lower for women who were born outside Australia, United Kingdom and Ireland (68%), spoke a language other than English at home (64%), were Aboriginal and Torres Strait Islander (64%), were in the lowest SEIFA quintile (72%), lived in very remote areas (70%), or had a disability (46%). Pilot participation rates over time are shown in Figure 1. At the beginning of the study period the participation rate was 88.9%, and gradually fell over time to 55.5% at the end of the study period.
Characteristics of screened women (N = 204,429) by height and weight trial participation status.
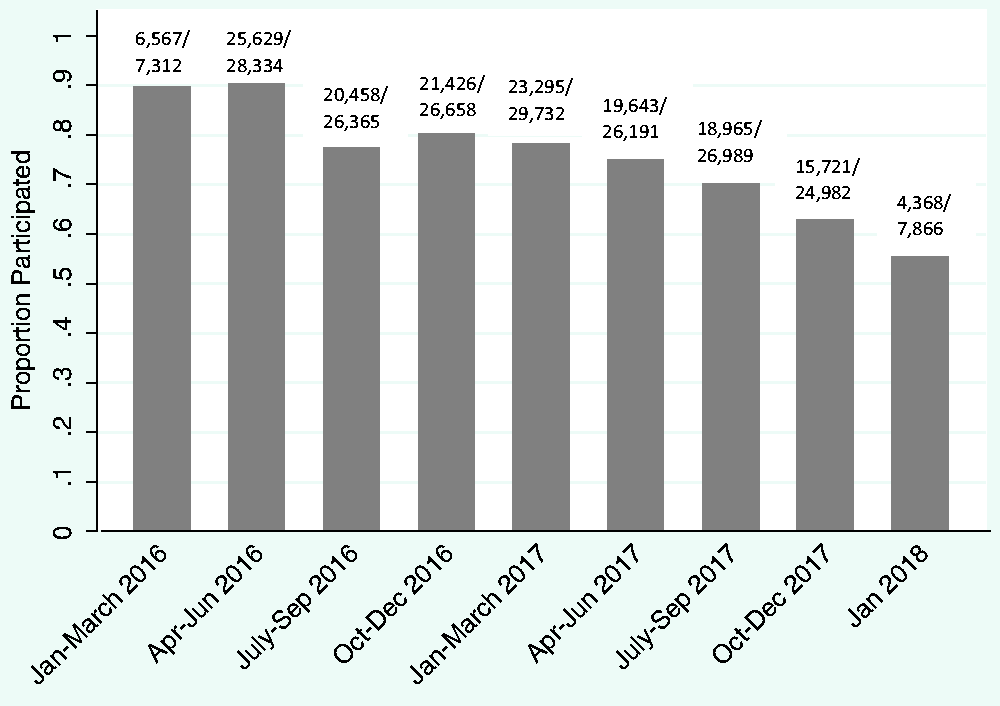
Proportion of trial participants by date screened at BreastScreen WA.
The results of the modified Poisson regression comparing demographic and screening characteristics of pilot participants and non-participants are shown in Table 2. All characteristics were significantly associated with pilot participation and were included in the multivariable model. As age increased, participation decreased, with women aged 80 or older 25% less likely to participate than those aged younger than 50 (RR: 0.746; 95% CI: 0.721, 0.772). Women who spoke a language other than English at home were 12% less likely (RR: 0.876; 95% CI: 0.867, 0.885), while those who used an interpreter were 55% less likely to participate in the pilot (RR: 0.449; 95% CI: 0.389, 0.519). Women who identified as Aboriginal and Torres Strait Islander were 17% less likely to participate in the pilot than those who did not (RR: 0.829; 95% CI: 0.807, 0.852). As socio-economic status increased, pilot participation rates increased, with those in the highest quintile 9% more likely to participate than those in the lowest (RR: 1.089; 95% CI: 1.078, 1.100). Compared with women living in major cities, women living in more remote areas were more likely to participate, however, this relationship was not linear. Women who had a disability were 37% less likely to participate (RR: 0.626; 95% CI: 0.600, 0.653).
Relative risks comparing characteristics of height and weight trial participants (n = 156,072) and non-participants (n = 48,357).
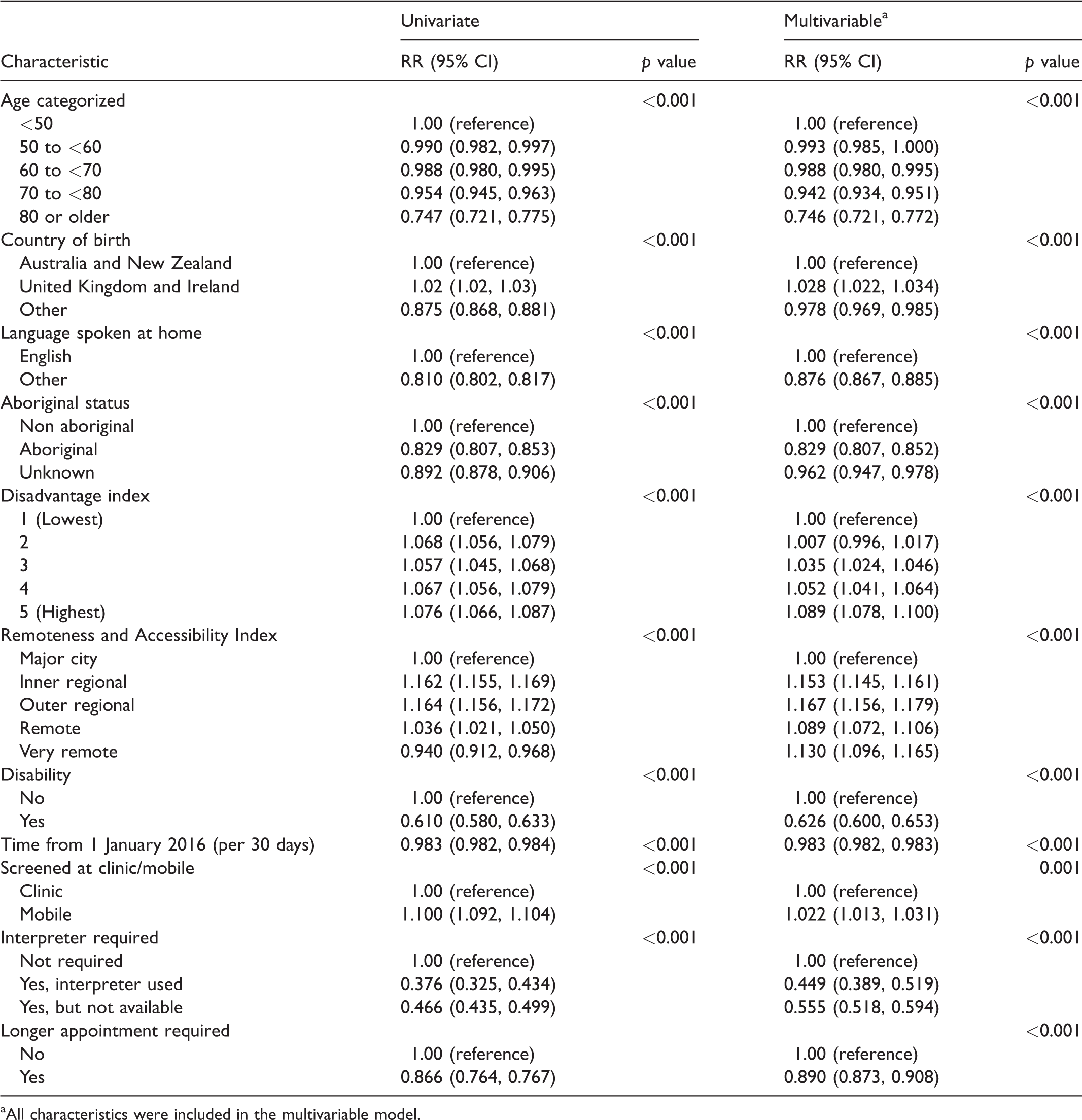
aAll characteristics were included in the multivariable model.
Figure 2 is a flow chart showing the number of measurements and the measurement errors identified. During the course of the pilot, four sets of scales malfunctioned and took up to a week to replace, depending on location. Of the 162,995 height and weight measurements taken, 10% were excluded due to defective scales (identified by date and location), and another 0.5% of measurements fell outside a pre-determined feasible range (see Figure 1). Figure 3 summarizes the repeated measurements collected for 6005 individuals who screened annually. The correlations between the first and second measurement for height and weight were above 0.9. There was less than 5 cm difference between heights for 95% of participants with repeated measures (Figure 3(a)), and less than 10 kg difference between weight measurements for 97% of participants with repeated measures (Figure 3(b)). The comparison of the heights and weights of the study population and the Australian population aged older than 35 from the Australian Bureau of Statistics’ National Health Survey are shown in Figure 4. The distributions were similar between the study participants and the Australian population for both height (Figure 4(a)) and weight (Figure 4(b)), with the study population seemingly slightly taller and heavier than the Australian population.
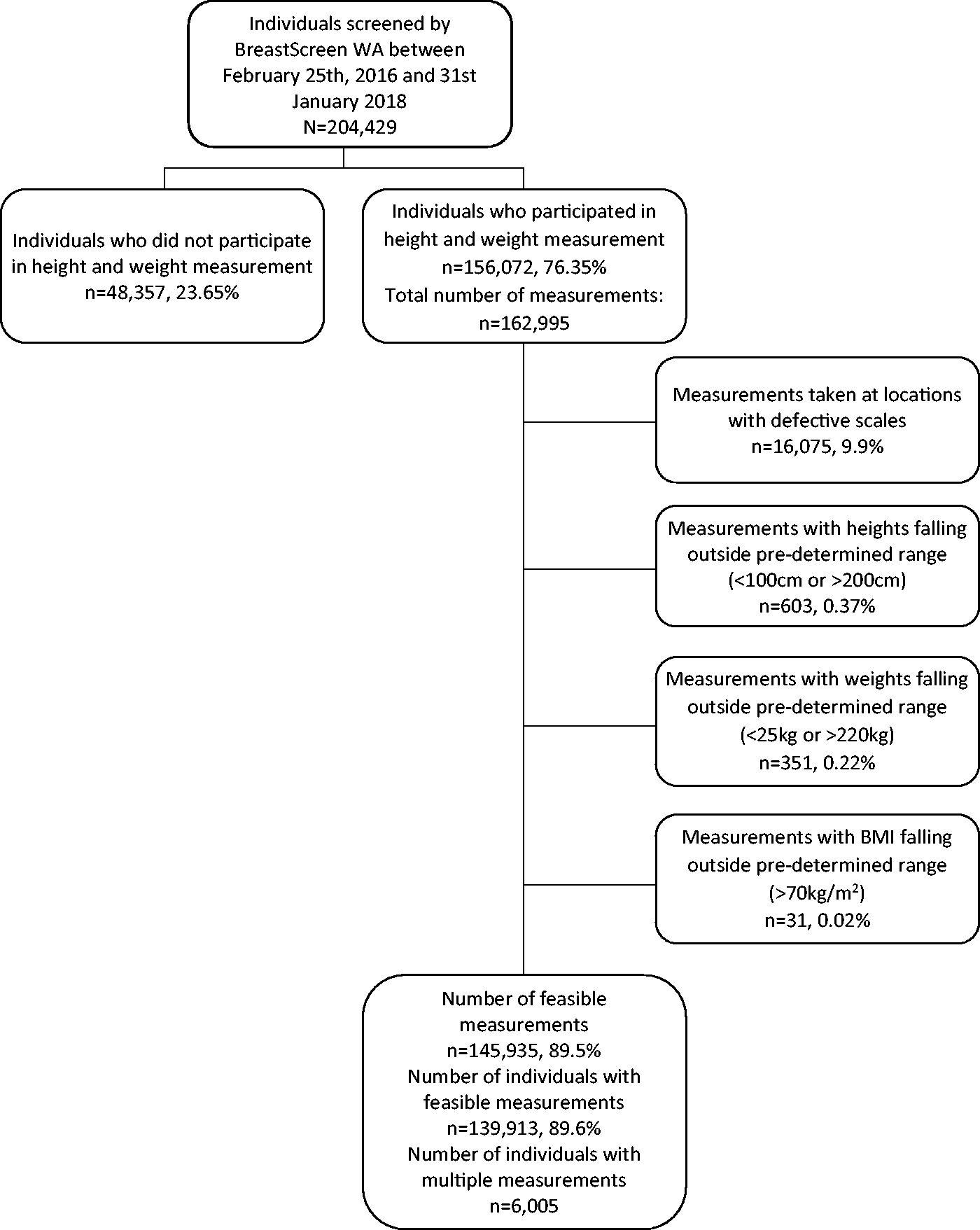
Flowchart outlining source of trial subjects and exclusion criteria.
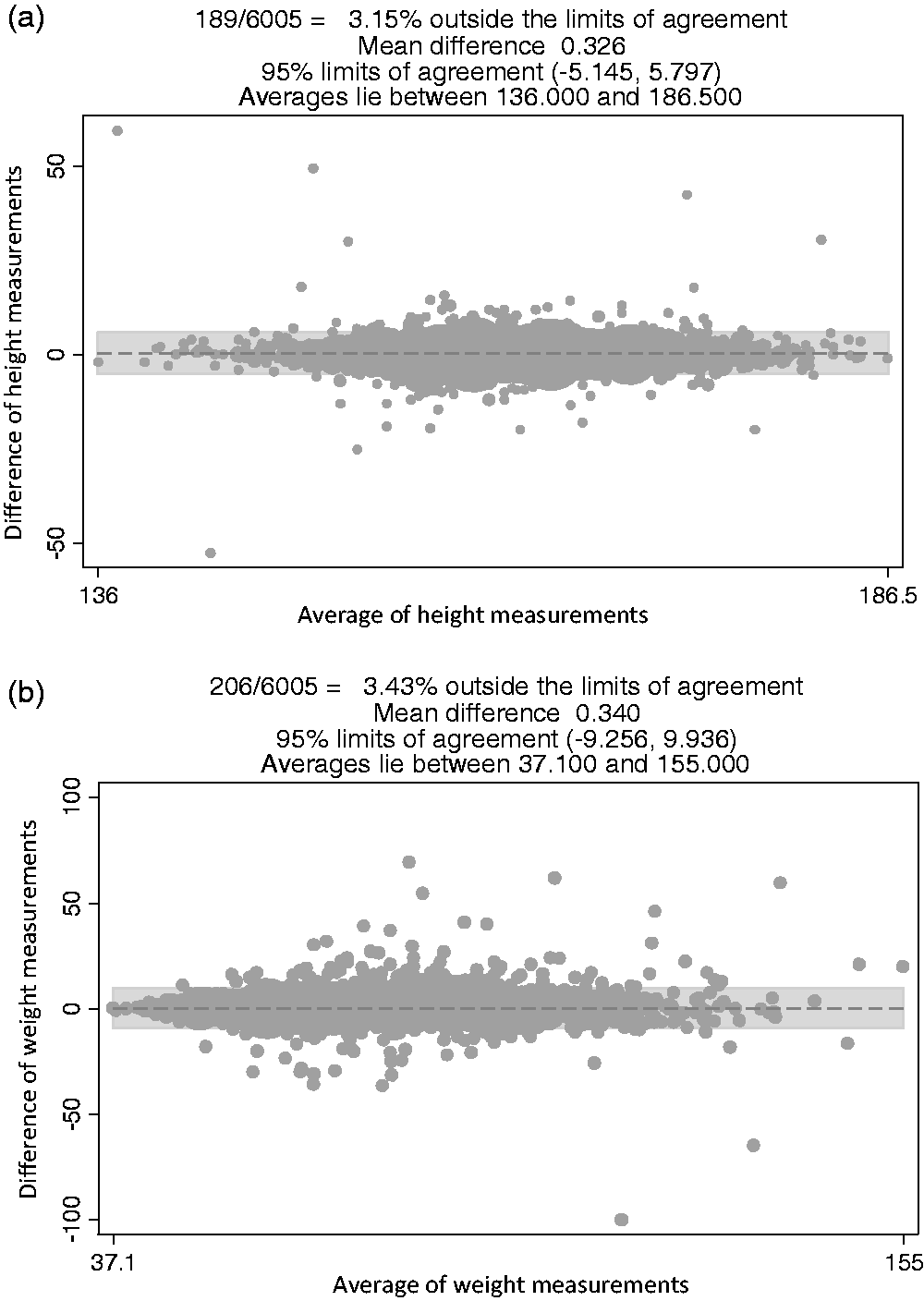
(a) Agreement between two measurements of height taken approximately one year apart from 6005 participants. (b) Agreement between two measurements of weight taken approximately one year apart from 6005 participants.
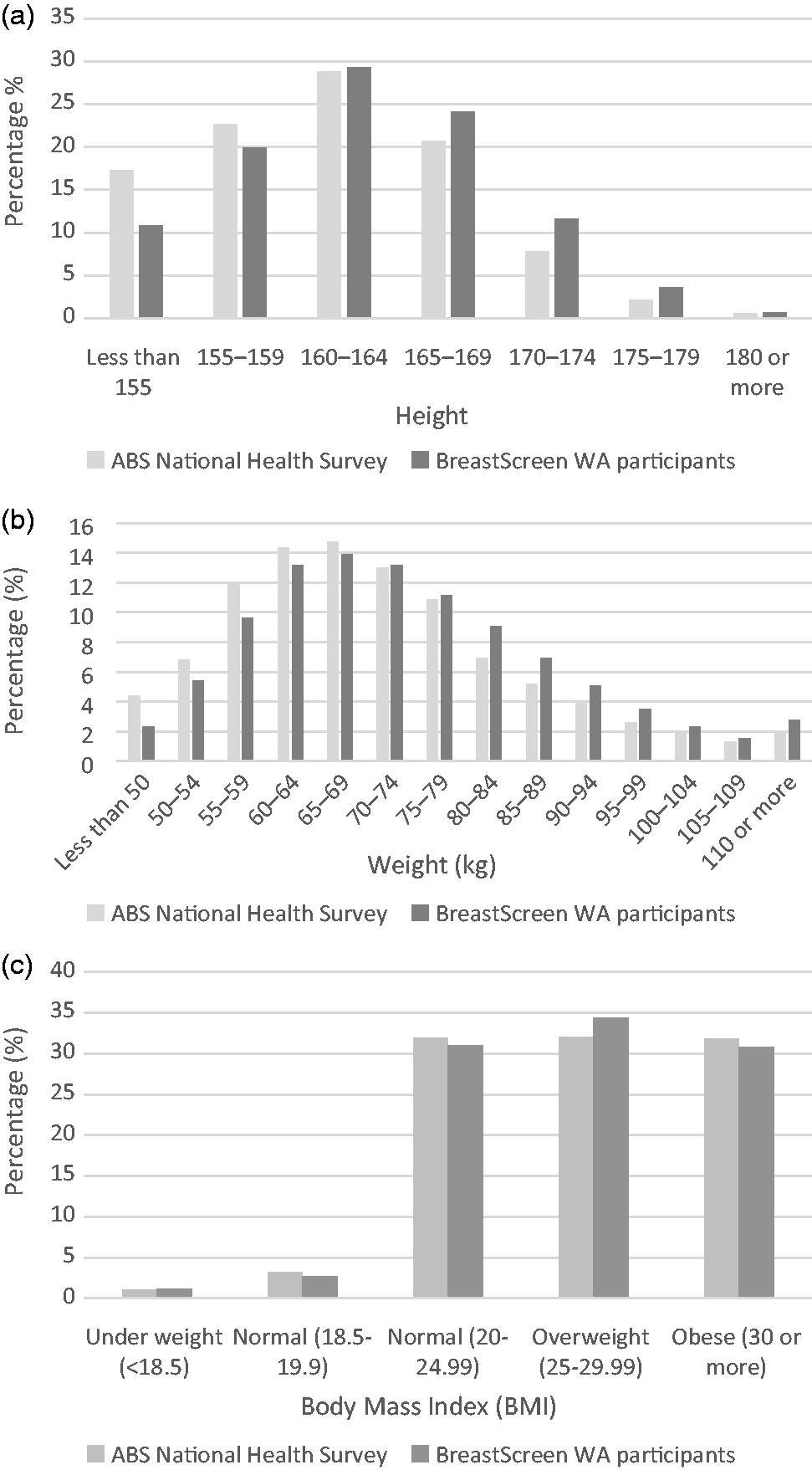
(a) Distribution of BreastScreen WA participants’ height measurements compared with Australian Bureau of Statistics National Health Study for ages 35 and older. (b) Distribution of BreastScreen WA participants’ weight measurements compared with Australian Bureau of Statistics National Health Study for ages 35 and older. (c) Distribution of BreastScreen WA participants’ body mass index measurements compared with Australian Bureau of Statistics National Health Study for ages 35 and older.
A comparison of the total volume of the breast between a random age-matched sample of participants and non-participants found non-participants to have larger breasts than participants (mean total breast volume; participants: 306.5 cm3, non-participants: 341.3 cm3).
Qualitative data analysis of open-ended comments from 243 women.
Discussion
This study demonstrates that voluntary measurement of height and weight at the time of routine mammography is feasible within a breast cancer-screening programme, with an overall pilot participation rate of 76%. Factors associated with reduced participation included increasing age, disabilities, language barriers and Aboriginal and Torres Strait Islander status, factors that have also been important in other population-based recruitment. 12 The largest impediment to participation was declining motivation of BreastScreen staff to invite women to have their height and weight measured. Open-ended comments provided by a subset of women suggest that most women are happy to have their height and weight measured, but some were concerned about the accuracy of the measures with clothes and shoes on. High correlation between height and weight measures taken approximately one year apart within a subset of women suggests reliability of the measures to be reasonable.
To our knowledge, this is the first study to evaluate the feasibility and appropriateness of routinely measuring and recording patient height and weight at the time of mammography. Implementation of the height and weight measurement devices occurred at minimal cost, albeit with additional costs related to replacement of defective scales. It relied upon the commitment of additional time by BreastScreen staff to invite women to participate and facilitate the measurement, and that commitment clearly diminished over time. Feedback from staff provided through the Chief Radiographer suggests that staff commitment declined over time and due to time constraints and concerns from participants regarding the accuracy of the measurements with shoes/clothes on. There were no formal opportunities for staff to receive information concerning the pilot or provide feedback, which could have had an impact on the declining pilot participation rate over time. Given that BreastScreen is risk averse to any additional process that might deter women from screening re-attendance, BreastScreen WA has subsequently implemented a policy of asking patients to voluntarily self-report their height and weight measurements.
Cross-sectional exclusions of measurement data due to defective scales were around 10%, with less than 1% of measurement data outside pre-determined ranges, probably due to data entry errors. Replacement scales were provided as promptly as possible, however a new instrument could take up to a week to arrive, depending on the service location, resulting in thousands of potentially inaccurate measurements. These measures were excluded based on date of malfunction and location. No routine calibration protocol was in place, an error that we highlight so that others collecting multisite population data of this nature can consider this in study planning. Despite efforts to remove potentially inaccurate measurements, there were still some large differences in height and weight in some who were re-screened, presumably due to data entry errors that were not picked up by our cross-sectional exclusion criteria.
Women who did not participate had significantly larger breast size compared with those who did participate. Total breast size has been shown to be positively correlated with BMI,13,14 suggesting that heavier women are less likely to volunteer to have their height and weight measured as part of routine screening mammography. Feedback from the small proportion of women who provided comment was largely positive, with over 40% of those 242 who commented being happy to have their height and weight measured. There were concerns expressed from around 20% of women who commented about the inaccuracy of measurements taken due to wearing shoes and partial clothing, a problem which is avoided by the decision to collect self-reported height and weight.
With over 156,000 prospectively collected height and weight measurements from a population-based screening programme, this study provides an extraordinary resource from which to investigate further research questions. BreastScreen WA is currently the only state programme in Australia that notifies women if they have dense breasts, one of the strongest predictors of breast cancer risk, and one that also significantly reduces the sensitivity of mammography to detect abnormalities. The association between breast density and breast cancer risk is highly (and negatively) confounded with age and BMI, associations that are clinically hard to translate. However, combined with other existing data regarding family history and personal history of premalignant lesions, there is potential to inform breast density notification protocol and/or assess individual risk.
Conclusion
This study found that routine measurement of patient height and weight at the time of mammography was feasible and acceptable to most women. However, logistical issues, particularly added time/effort/education required of screening clinic staff, and calibration and checking of functioning of scales, need to be considered. Due to these issues, BreastScreen WA is now collecting voluntary self-reported height and weight data as routine screening policy.
Supplemental Material
Supplemental material for Measuring height and weight as part of routine mammographic screening for breast cancer
Supplemental Material for Measuring height and weight as part of routine mammographic screening for breast cancer by Ellie Darcey, Ravi Ambati, Helen Lund, Andrew Redfern, Christobel Saunders, Sandra Thompson, Elizabeth Wylie and Jennifer Stone in Journal of Medical Screening
Footnotes
Acknowledgements
The authors acknowledge the BreastScreen Western Australia staff for their involvement in the collection of the data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study is funded by Cancer Council Western Australia and Cancer Australia (APP1085750).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.