
Abstract
Objective
To compare characteristics and survival of New Zealand European, Māori, and Pacific women with screen-detected vs. non-screen-detected breast cancer.
Methods
Women aged 45–69 diagnosed with invasive breast cancer between January 2005 and May 2013 were identified from the Waikato and Auckland Breast Cancer Registries. Patient demographics and tumour characteristics were described by detection mode and ethnicity. Kaplan–Meier method was used to estimate the five-year breast cancer-specific survival of women with stage I–III breast cancer by ethnicity and detection mode.
Results
Women with screen-detected cancers were older, had smaller tumours, fewer stage IV (0.8% vs. 7.6%), fewer high grade (16.8% vs. 39.0%), and fewer lymph node positive diseases (26.3% vs. 51.5%) than women with non-screen-detected cancers. There were more Luminal A (70.0% vs. 54.0%), fewer human epidermal growth factor receptor 2 positive non-Luminal (4.4% vs. 8.8%), and fewer triple negative cases (7.0% vs. 13.8%) in screen-detected than non-screen-detected cancers. If not screen detected, 22.7% of breast cancers in Pacific women were stage IV compared with 2.4% if screen detected. If not screen detected, the five-year breast cancer-specific survival was 91.1% for New Zealand European women, 84.2% for Māori women, and 80.2% for Pacific women (p-value <0.001). For screen-detected breast cancer, survival between different ethnic groups was similar.
Conclusions
Breast cancers detected through screening are diagnosed at an earlier stage and have a greater proportion of subtypes, with better outcome. Variations in survival for Māori and Pacific women are only found in women with non-screen-detected breast cancer.
Introduction
One of the main reasons that outcomes of breast cancer in Māori and Pacific women are poor compared with New Zealand (NZ) European women1–4 is the late stage at diagnosis in Māori and Pacific women. 4 Māori and Pacific women are less likely to have screen-detected breast cancer.4,5 Patients identified through breast screening have better outcomes, mainly because of diagnosis at an earlier stage, 6 and screen-detected breast cancers may be less aggressive than those diagnosed symptomatically. Māori and Pacific women are less likely to have triple negative disease compared with NZ European women, while Pacific women are more likely to have human epidermal growth factor receptor 2 positive (HER2+) non-Luminal disease than others.2,7 We wanted to know what influence breast screening has on outcomes for Māori and Pacific women compared with NZ European women, and how this is influenced by cancer stage at diagnosis and biomarker subtype.
Breast screening became universally available in NZ in 1998 for women aged 50 to 64. In 2004, the age range was extended to 45 to 69. Screening has been reasonably well accepted by NZ European women. Uptake in Māori women has been slower,8,9 although the gap is narrowing. 10 This study is based on data from two large population-based registers of newly diagnosed breast cancer in the Auckland and Waikato regions. These registers are derived from a baseline population from approximately 1.7 million residents and include about 1000 new breast cancer cases per year. This study aims to compare the characteristics and survival of NZ European, Māori, and Pacific women with screen-detected breast cancer with women of similar age with non-screen-detected breast cancer.
Methods
Data were obtained from the Waikato (WBCR) and Auckland (ABCR) Breast Cancer Registries. The WBCR is a prospectively maintained regional cancer registry that includes all in situ and invasive breast cancers diagnosed in the Waikato District Health Board area since 1999. The ABCR was established in 2000 by the Auckland Breast Cancer Study Group, and includes all breast cancers diagnosed within the Auckland, Waitemata, and Counties Manukau District Health Boards (DHBs), including those from private Breast Centres within the region. The WBCR and ABCR data covers a population of approximately 1.7 million, of which 29% of women are in the targeted screening age groups (45–69). Waikato DHB area has a larger proportion of Māori (23%) than Auckland DHB (8%), Waitemata DHB (10%), and Counties Manukau DHB (16%), but have a smaller proportion of Pacific (3%) than the other three DHBs (11%, 7%, and 21%, respectively).
This study included women aged 45 to 69 diagnosed with invasive breast cancer between January 2005 and May 2013. Data extracted for the study include: age, stage at diagnosis, tumour size, lymph nodes, year of diagnosis, method of diagnosis (screen detected, not screen detected), biomarker type (Luminal A, Luminal B1, Luminal B2, HER2+ non-Luminal, triple negative disease),2,7 and mortality data (date of death and cause of death). The Mortality Collection was also linked to the Combined Register through the National Health Index number to ensure the accuracy and completeness of these mortality data.
Patient demographics and tumour characteristics were described by mode of detection and by ethnic group. Survival analyses were performed in women with stage I–III breast cancer only. Patients were considered to be censored on the date of death or the last updated date of Mortality Collection, which was 31 December 2014. Kaplan–Meier method was used to estimate the five-year breast cancer-specific survival by ethnicity and by mode of detection. All data analyses were performed in IBM SPSS statistics 25 (New York, United States).
The study is covered under ethics approval from the Health and Disability Ethics Committee – Approval Number: 12/NTA/42/AM01.
Results
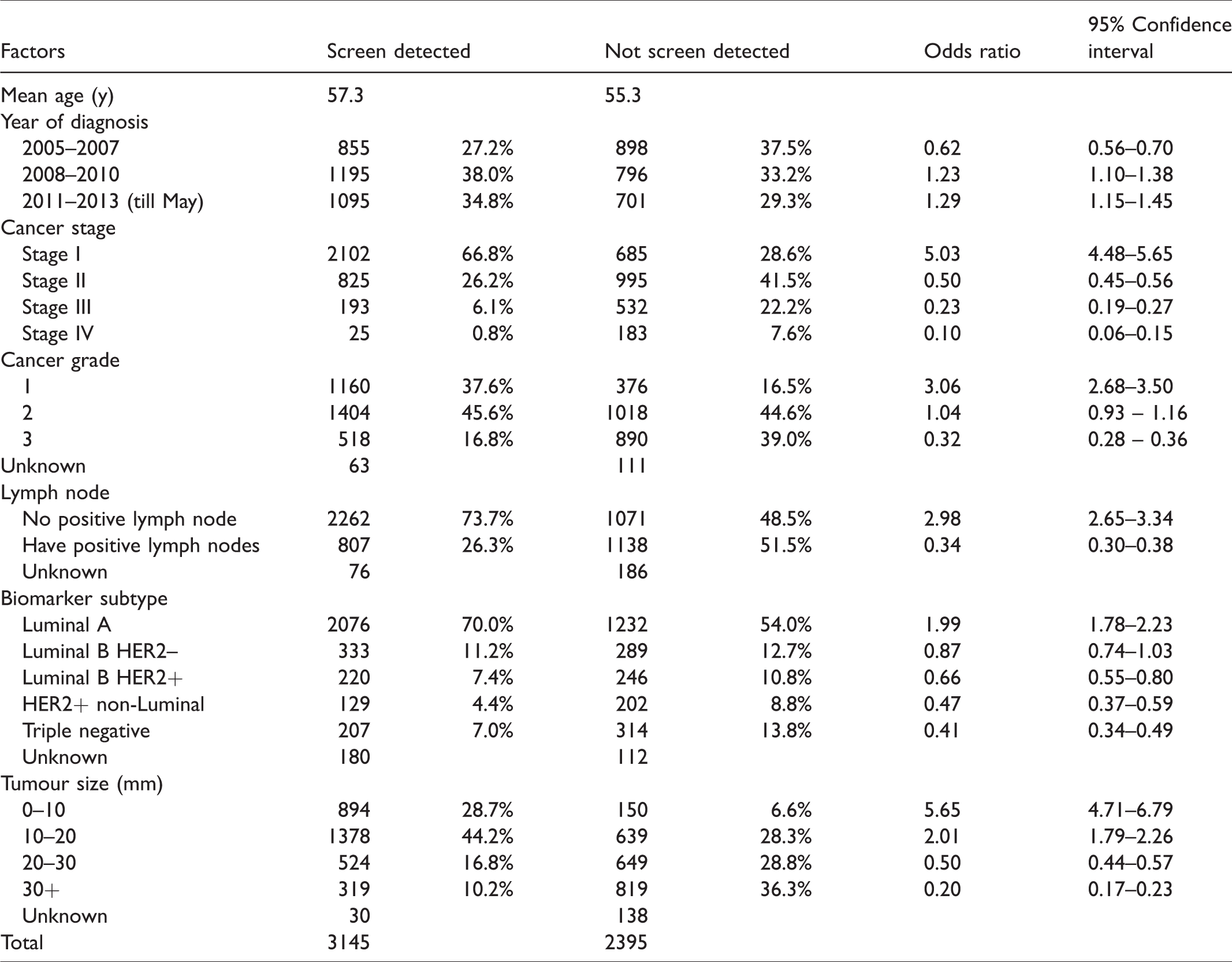
The number of breast cancer cases detected by screening increased per year over the study period, and the number of non-screen-detected cases decreased (Table 1). Women with screen-detected cancers were slightly older (mean age 57.3 compared with 55.3 for non-screen-detected women), had smaller tumours, were less likely to have stage IV (0.8% vs. 7.6%) and high-grade diseases (16.8% vs. 39.0%), and were less likely to be lymph node positive (26.3% vs. 51.5%) compared with women with non-screen-detected breast cancers. There were more Luminal A (70.0% vs. 54.0%), fewer HER2+ non-Luminal (4.4% vs. 8.8%), and fewer triple negative disease (7.0% vs. 13.8%) cases in the screen-detected cancers than non-screen-detected cancers.
Characteristics of breast cancer patients by mode of detection.
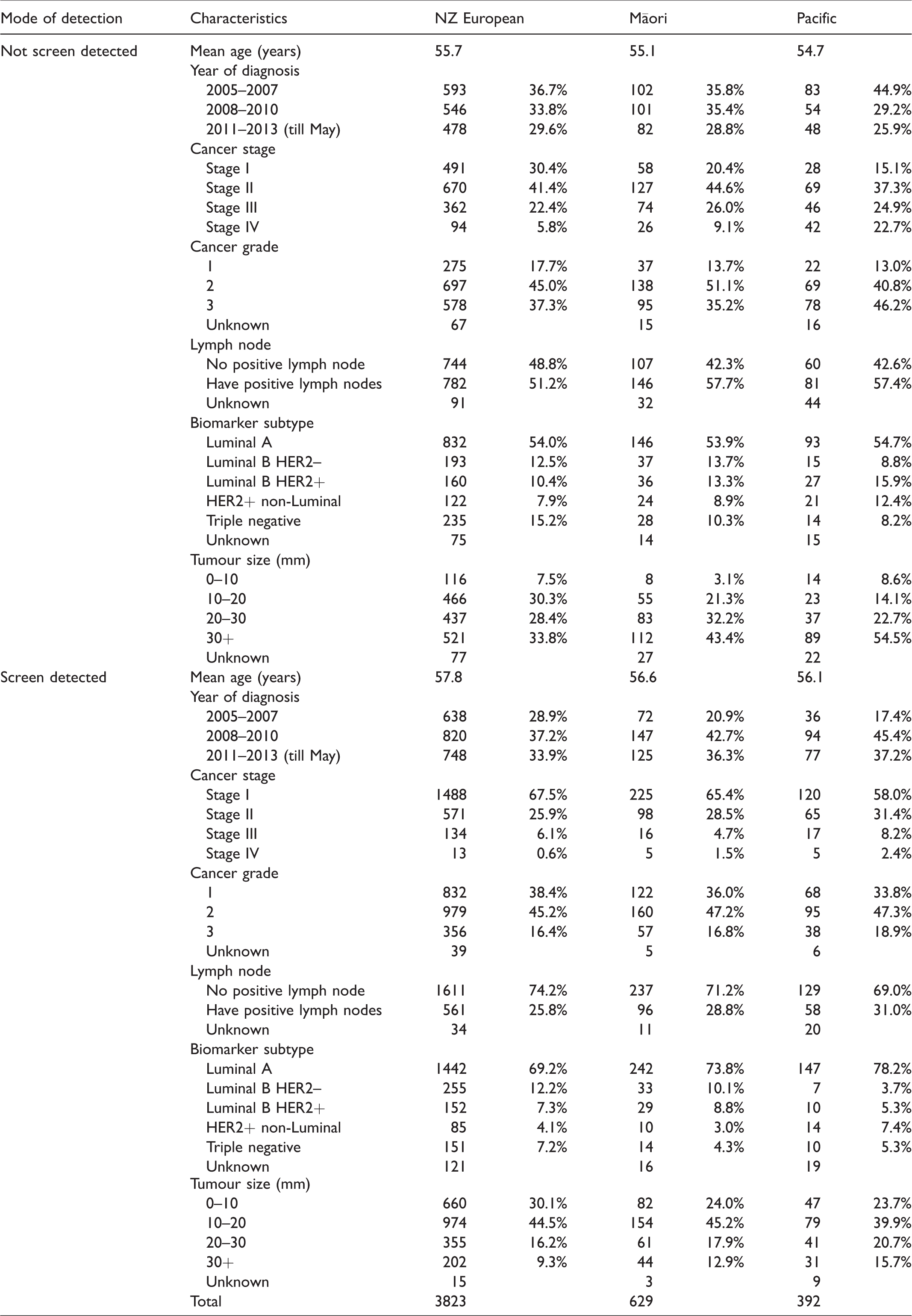
Māori and Pacific women were more likely to have advanced breast cancer stage, positive lymph node, bigger tumour size, and HER2+ disease, but less likely to have triple negative disease than NZ European women (Table 2). These differences were identified in both the non-screen-detected group and in the screen-detected group. If not screen detected, 22.7% of Pacific women were diagnosed with stage IV breast cancer, compared with 2.4% if they were screen detected.
Characteristics of breast cancer patients by ethnicity.
Overall, survival was better in women with screen-detected than non-screen-detected cancer (Figures 1 and 2, Table 3). The five-year breast cancer-specific survival was 89.8% for non-screen-detected patients and 97.2% for screen-detected patients. If the cancer was not screen detected, the five-year breast cancer-specific survival was 91.1% for NZ European women, 84.2% for Māori women, and 80.2% for Pacific women (log-rank test p-value <0.001). If cancer was screen detected, the breast cancer-specific survival between different ethnic groups became similar (log-rank test p-value =0.075).
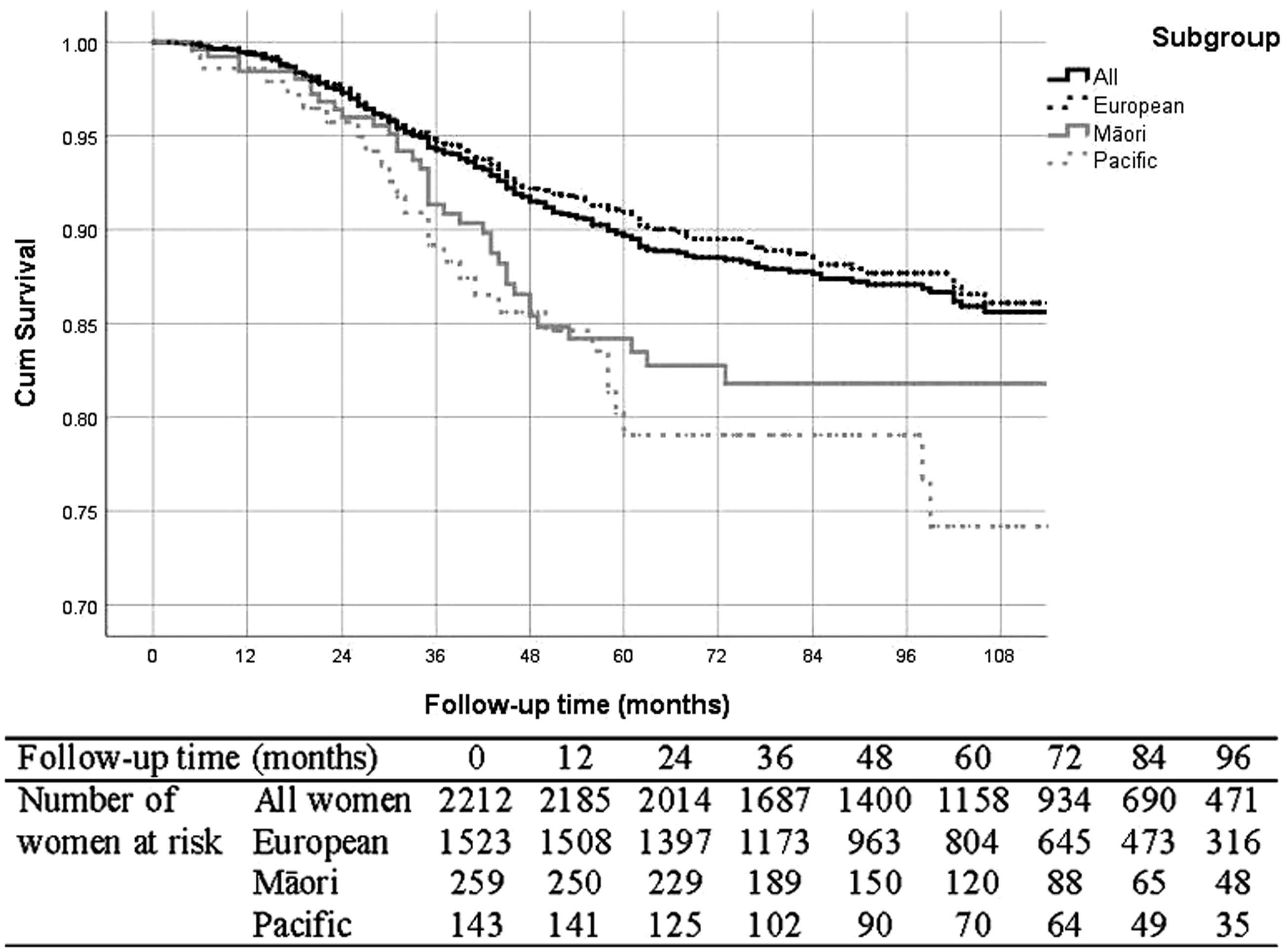
Kaplan–Meier breast cancer-specific survival curve for not screen-detected women.
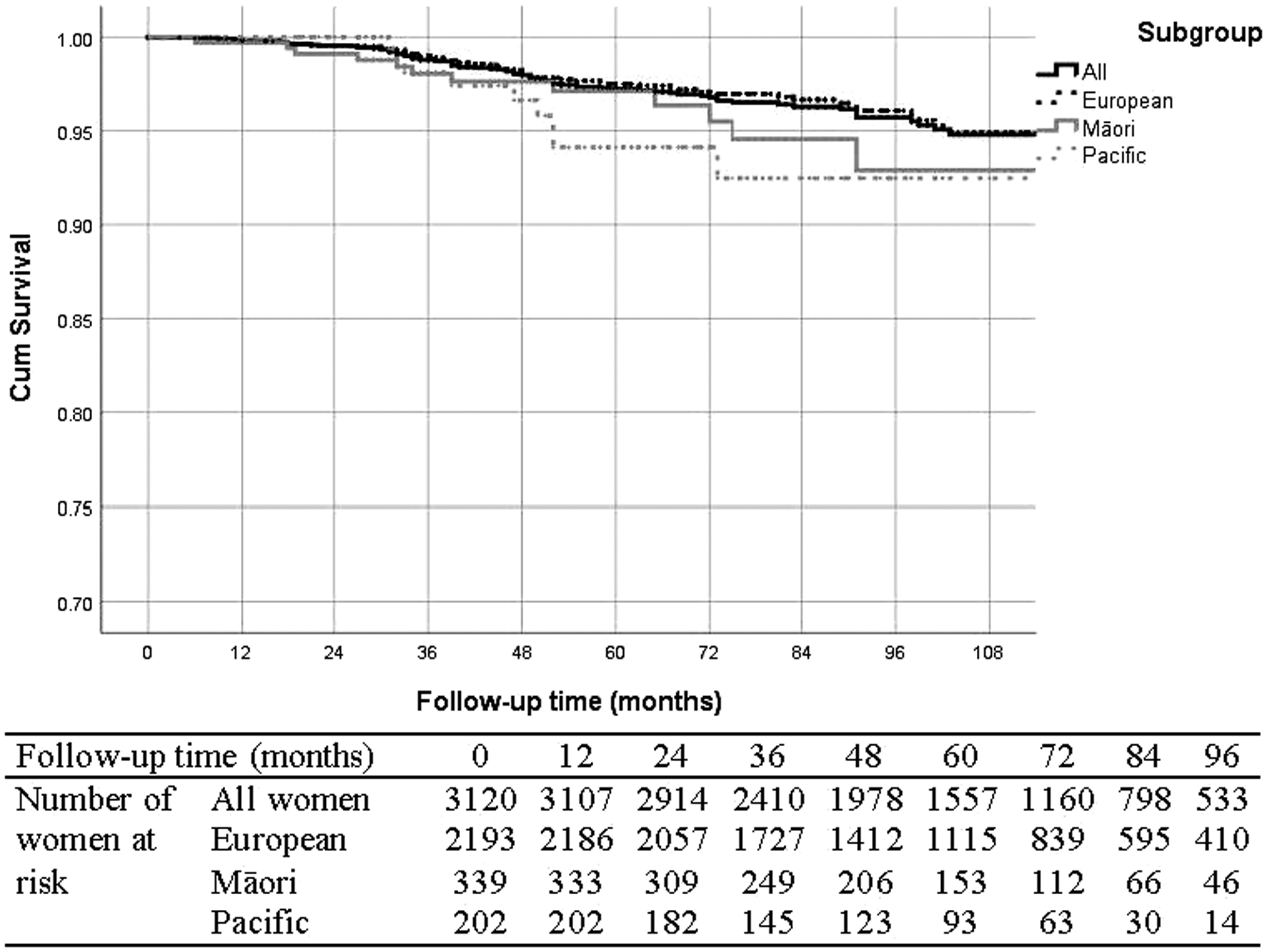
Kaplan–Meier breast cancer-specific survival curve for screen-detected women.
Five-year breast cancer-specific survival of women with stage I–III breast cancer.

Including New Zealand (NZ) European, Māori, Pacific, and others.
Discussion
Previous studies have demonstrated that some screen-detected breast cancers have a unique natural history and biology compared with symptomatic breast cancers.11,12 Our results show, as expected, that screen-detected breast cancers were less aggressive than non-screen-detected cancers: 70% Luminal A compared with 54%. Screen-detected cancers were diagnosed at an earlier stage (66.8% stage I disease and 26.3% lymph node positive). This is consistent with other studies,13–17 showing that in patients with screen-detected cancer, most had Luminal A cancer and stage I disease, and only 1% of patients had stage IV cancer.
There were also differences comparing Māori, Pacific, and NZ European women, with the greatest difference found in Pacific patients. The greatest difference was the five-year survival difference (13.9%) in Pacific patients with screen-detected (94.1%) compared with non-screen-detected (80.2%) cancer. Adherence to the screening programme and improvements in access to earlier diagnosis for Pacific women have the potential to make a substantial difference in breast cancer outcomes. 3
Five-year survival outcomes are short term for breast cancer, yet even at this early stage, there are major differences in survival by ethnicity for women with cancer diagnosed through a non-screen pathway. These differences are expected to grow in magnitude with longer follow-up. We have previously published on some of the reasons behind this. 18 When women are diagnosed through a screen-detected pathway, these differences almost disappear, and the five-year survival outcomes for all ethnic groups are very high. In part, these higher survival rates are explained by lead-time bias and length-time bias.13–17,19 Screening advances the date of diagnosis, with a longer survival time expected even without treatment, and identifies more slow growing tumours (e.g. more Luminal A diseases) in the screen-detected group.
There are real survival benefits for women as a result of breast cancer screening. Multiple previous studies have demonstrated a 20–30% reduction in breast cancer mortality as a result of population-based screening.20–22 This is the kind of benefit seen when screening is applied to an average population. When screening is made available to populations that have much higher than average death rates for breast cancer, there is the potential for a much greater mortality benefit, if high population coverage can be achieved. In NZ, a major effort has been made to improve the initially poor coverage amongst Māori and Pacific women. Coverage for these ethnic groups is now approaching 70% of eligible women. 23 Our study strongly supports this initiative, and the message that Māori and Pacific women diagnosed through breast cancer screening do just as well as any ethnic group is an important one to promulgate. Not only may this result in further improvements in screening coverage, but it enhances breast awareness, and the need for early diagnosis – later stage at diagnosis having previously been demonstrated to be the single most important reason for worse outcomes in NZ Māori and Pacific populations. This study suggests that when population-based screening is applied successfully to disadvantaged ethnic groups, mortality benefits may be significantly better than for more advantaged populations.
On the other hand, the Breast Screen Aotearoa Programme has a strict protocol for the management of women post diagnosis, while there is more variation in the management of women with non-screen-detected breast cancer. This also suggests that standard management can reduce the inequity in outcomes in Māori and Pacific women.
A strength of this study is the data sources. The Waikato and Auckland population-based Breast Cancer Registers collect good-quality data on all breast cancer patients, 24 with large numbers of patients in different ethnic groups for comparison analyses, and have comprehensive data on patient characteristics, mode of diagnosis, and outcomes. Our study was not designed to prove the benefit of breast screening. The inclusion of interval cancers with cancers in patients who have never attended breast screening will mean that the survival benefit seen in the screened population will be greater than if an intention to screen analysis had been undertaken. Another weakness is that the follow-up time for some patients (701, 29.3% of patients diagnosed in 2011–13) was short and may not be enough to identify ethnic differences in survival in screen-detected breast cancers.
Conclusion
This study shows that in our population in NZ an increasing proportion of breast cancers are being diagnosed through breast screening. Women with screen-detected breast cancer are diagnosed at an earlier stage of disease and have a greater proportion of subtypes that have a more favourable outcome. The study also shows that there are differences in the characteristics of Māori and Pacific women, especially those with non-screen-detected cancer. It appears that the variations in survival for Māori and Pacific women are only found in those with non-screen-detected breast cancer.
Footnotes
Acknowledgements
The authors acknowledge the Auckland and Waikato Breast Cancer Registers for providing the detailed data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the New Zealand Health Research Council (grant number 14/484). The authors acknowledge the Health Research Council of New Zealand for providing financial support and the New Zealand Breast Cancer Foundation and the Waikato Bay of Plenty Division of the Cancer Society for funding the Registers.