
Abstract
Objective
The main purpose of skin cancer screening is melanoma mortality reduction. Before the implementation of nationwide German skin cancer screening, the pilot project SCREEN was conducted in Schleswig-Holstein in 2003–2004. We aimed to determine whether the pilot project had achieved a mortality reduction.
Methods
Using an incidence-based approach (patients with both melanoma diagnosis and death in 2003–2008), we compared the observed melanoma mortality of the SCREEN cohort to the melanoma mortality expected without screening in the general population of Saarland.
Results
The age- and sex-standardized melanoma mortality ratio (SMR) for 5.5 years of follow-up was 0.59 (95% confidence interval, 0.40–0.83).
Conclusion
Our results indicate reduced mortality in the SCREEN cohort. Several potential biases cannot be excluded, but most of them tend to inflate the SMR.
The introduction of nationwide skin cancer screening in 2008 in Germany was preceded by a pilot project, ‘SCREEN’, conducted in the federal state of Schleswig-Holstein. 1 The main objective of skin cancer screening is a reduction in melanoma mortality. A previous publication indicated a decrease in melanoma mortality in the general population during and after the implementation of the SCREEN project, while no similar reduction was observed in the surrounding regions without systematic screening activities.2,3 In addition to this evaluation approach, the effect of SCREEN on melanoma mortality can be estimated by comparing the observed mortality in the SCREEN cohort with the expected mortality, based on a reference population.
The SCREEN cohort included participants in the SCREEN project between July 2003 and June 2004. The SCREEN dataset was later linked to the data from the population-based cancer registry of Schleswig-Holstein. This linkage provided information for all SCREEN participants on melanoma diagnoses before or after SCREEN and on vital status (including cause of death) until the end of 2008. The general population of Saarland was chosen as an external comparison group (in Saarland, no screening was conducted until mid-2008). Data on melanoma incidence and death were provided by the Saarland Cancer Registry. The choice of method for calculating the observed and the expected number of melanoma deaths (ICD-10: C43) is crucial. 4 We applied an incidence-based approach. The mortality rates in the SCREEN cohort and in the Saarland comparison group were both based on deaths in the period July 2003 to December 2008 from tumours diagnosed in the same period. The observed mortality was calculated as melanoma deaths per 100,000 person years in the SCREEN cohort. The number of expected melanoma deaths was standardized by sex and 5-year age group to that of the SCREEN cohort, resulting in the age- and sex-standardized expected mortality. The 95% confidence interval of the standardized mortality rate (SMR) was calculated using the Byar approximation. 5
Observed and expected melanoma mortality.
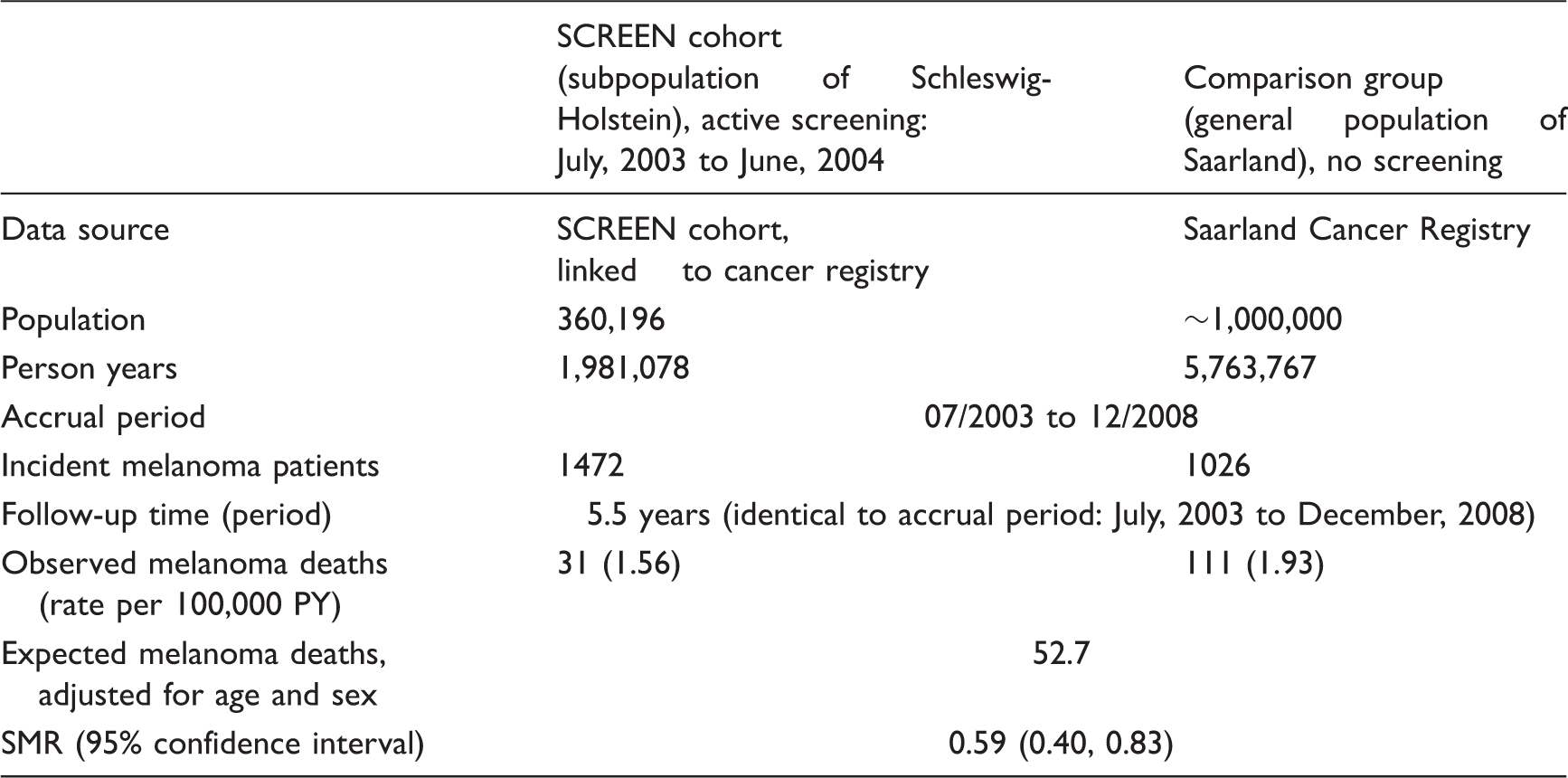
SMR: standardized melanoma mortality ratio.
For the first time, a large cohort of participants in whole-body examination for skin cancer screening, which conformed to the subsequently introduced nationwide guidelines on skin cancer screening, could be followed up for 5.5 years. The results from the SCREEN cohort indicate a significant reduction of melanoma mortality. The results are in good accordance with a previous population-based analysis of melanoma mortality in the whole screening region, 2 where within 10 years a reduction of nearly 50% after SCREEN compared with the pre-SCREEN period was reported. A recent systematic review on skin cancer screening also showed positive effects, but the evidence level was low. 3 The observed reduction in melanoma mortality in our cohort can probably be attributed to the screening intervention, but confounding factors and bias cannot be ruled out.
The main danger for finding an artificially low SMR is self-selection bias. SCREEN participants could have had a more favourable health behaviour and prevalence of risk factors (such as avoiding extreme sun exposure or visits to solariums) than the general population, and so the risk of dying from melanoma could be lower even without screening. While it was found that self-selection was probably present, it was also found that a large proportion of patients with risk factors for melanoma participated in the SCREEN project,1,6 so self-selection probably did not affect the SMR or may even have increased it.
There are several biases that potentially hamper the identification of a true reduced SMR. First, regional differences in the disease burden of melanoma may overestimate the SMR. Age-standardized melanoma mortality in the pre-SCREEN period (1998–1999) was previously higher in Schleswig-Holstein than in Saarland (2.35 versus 1.75 per 100,000), 7 so a true mortality reduction in the SCREEN cohort may be masked. Second, melanoma mortality in the SCREEN cohort may be overestimated because of insufficient exclusion of participants with a previous melanoma diagnosis. While Saarland has a long-standing cancer registry, the registry of Schleswig-Holstein did not start until 1998. Third, the longer the accrual period, the more the SMR can be biased to 1 because an increasing proportion of deaths are caused by melanomas that were diagnosed after SCREEN and were never able to benefit from the immediate screening. Despite these possible biases, we still found a significantly reduced mortality in the SCREEN cohort.
This study had several strengths, including the linkage of the SCREEN participants to the cancer registry of Schleswig-Holstein that provided the necessary follow-up information. In addition, the Saarland Cancer Registry made it possible to use the general population as an external comparison group, which contributed a large number of person years (more than 5 million). The follow-up time of 5.5 years was sufficient to suggest a mortality advantage in the SCREEN cohort. The effect might be even larger with a longer follow-up period because early detection may prevent deaths in the more distant future.
Although nationwide skin cancer screening was introduced based on findings of the SCREEN project, there are relevant differences in several aspects of their implementation, such as intensity of educational advertising, and special attention to persons with increased risk. 8 The results of the SCREEN project must therefore not entirely apply to the nationwide screening programme.
In our calculation of incidence-based melanoma mortality ratios for the SCREEN cohort compared with the general population of Saarland, there were several biases due to methodology and study design, but most of these tend to inflate the SMR. Despite this, our results indicate a significant 41% lower than the expected melanoma mortality in the SCREEN cohort.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.