
Abstract
Objectives
To assess patterns and probabilities of participation in multiple rounds of colorectal cancer screening.
Methods
All individuals who were invited to participate in population-based colorectal cancer screening in the Stockholm-Gotland region in Sweden between 1 January 2008 and 30 September 2015 were included in the study. Guaiac-based faecal occult blood testing was used. All individuals invited to the three first consecutive screening rounds were included in the analysis.
Results
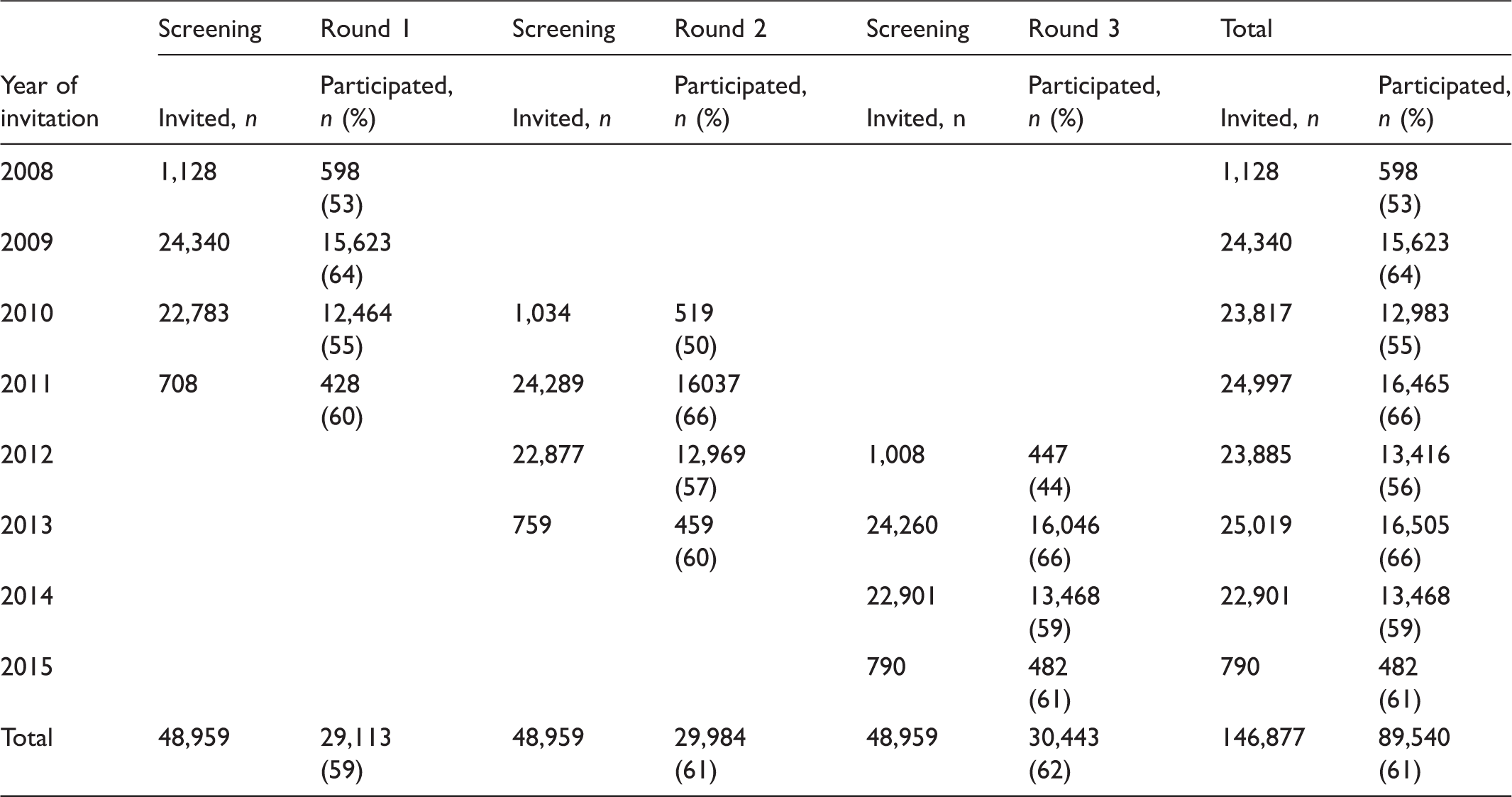
There were 346,168 individuals eligible for invitation to screening. The average participation rate during the follow-up period was 60%. Eligible individuals could be invited 1–4 times, depending on age at first invitation. Of 48,959 individuals invited to the three first consecutive rounds of screening, 71% participated at least once, and 50% participated in all three rounds. Participation at first invitation was a predictor for participation in subsequent rounds, and the likelihood of continuous participation following participation in the first round was 84%. Of those who attended the first and second rounds, 93% also participated in the third round. Similar patterns of consistency were seen among non-participants. For individuals not participating in the first screening round, the likelihood of consistent non-participation was 71.
Conclusions
Participation in the first round of screening is a strong predictor for participation in subsequent rounds. Therefore, reducing barriers for initial participation is a key for achieving consistent participation over several rounds in organized colorectal cancer screening programmes.
Introduction
To achieve the purpose of screening (to reduce disease-specific mortality), and to enhance screening efficacy, participation needs to be high. As this outcome measure requires long-term follow-up, participation is a valid surrogate measure for continuous evaluation of the efficacy of a screening programme. However, in population-based colorectal cancer (CRC) screening, participation rates in many programmes lie below 50% and rarely exceed 60%. 1
A number of studies assessing participation patterns in CRC screening programmes have shown similar demographic predictors for non-participation, that is low socio-economic status, male gender and younger age.2–4 Some recent qualitative studies have sought to more deeply understand individual reasons for non-participation, and have identified key issues for non-participation, such as fear of cancer/test result, disgust/shame by handling the test itself, inability to understand the testing procedure/aim of the test and procrastination in performing the test.5,6
The aim of this study was to assess, in detail, patterns and probabilities of participation in multiple screening rounds, in the population-based CRC screening in Stockholm/Gotland, the capital region of Sweden. During the study period, the guaiac-based faecal occult blood test (gFOBT) Hemoccult® was used.
Methods
In 2008, population-based CRC screening was introduced in the capital region of Stockholm, an area with approximately 2 million inhabitants. All individuals aged 60–69 are invited from a central screening centre to a biennial screening cycle. The programme was gradually expanded by successively inviting new birth cohorts, and was fully rolled-out in 2013. 7 The different age cohorts included varied in size due to natural variations in the population. From 2014, invitations to the first screening round have been sent only to individuals aged 60. Until September 2016 gFOBT was used, after which faecal immunochemical testing (FIT) was introduced.
Addresses of individuals invited to screening were obtained from The Swedish Tax Agency, a national agency that manages civil registration of private individuals. All those invited in the Stockholm/Gotland screening programme between 1 January 2008 and 30 September 2015 were included in the study. During this period the programme used gFOBT.
For analysis of participation patterns, we included all individuals with three complete screening rounds, defined as three consecutive invitations to the three first consecutive rounds of biennial screening, whether or not the invited individual chose to participate. Participation was defined as a returned gFOBT test from an individual invited to screening. Screening participants diagnosed with CRC or polyps requiring follow-up are included in separate follow-up programmes and not invited to any further screening rounds, so were not included in the analyses. Patterns of participation were analysed, and the probability of re-participation estimated. Eight possible patterns of participation were identified and merged into five groups: consistent participants, consistent non-participants, late entrants, drop-outs and intermittent participants.
The study was approved by the Regional Ethics Committee in Stockholm. Stata 14.0 (StataCorp, 4905 Lakeway Drive, College Station, TX, USA) was used for analyses of data.
Results
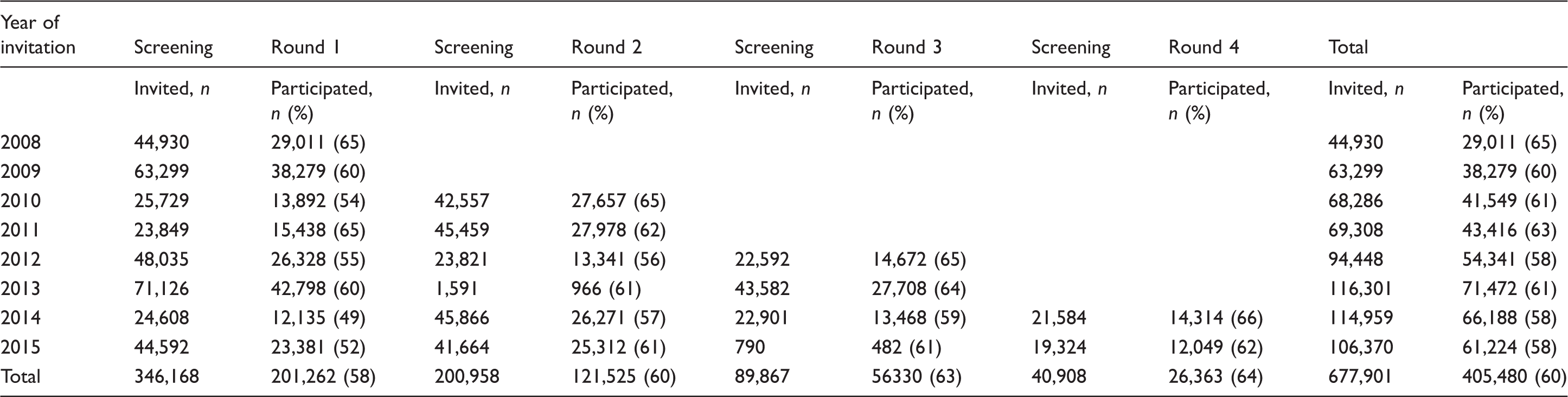
Participation in screening, all rounds 2008–2015.
Participation in screening, all rounds 2008-2015, men and women separately.
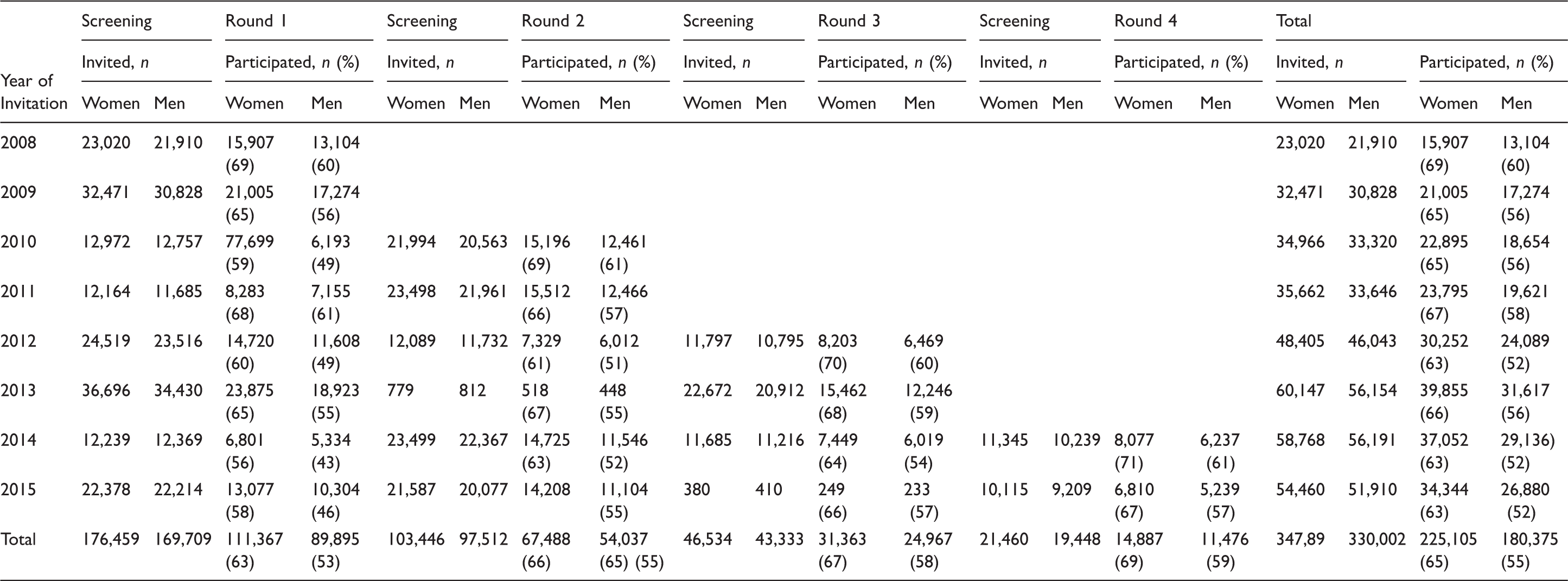
The variation in the number of participants in different years was due to the successive inclusion of different age cohorts during implementation and roll-out of the programme.
Participation in three complete screening rounds.
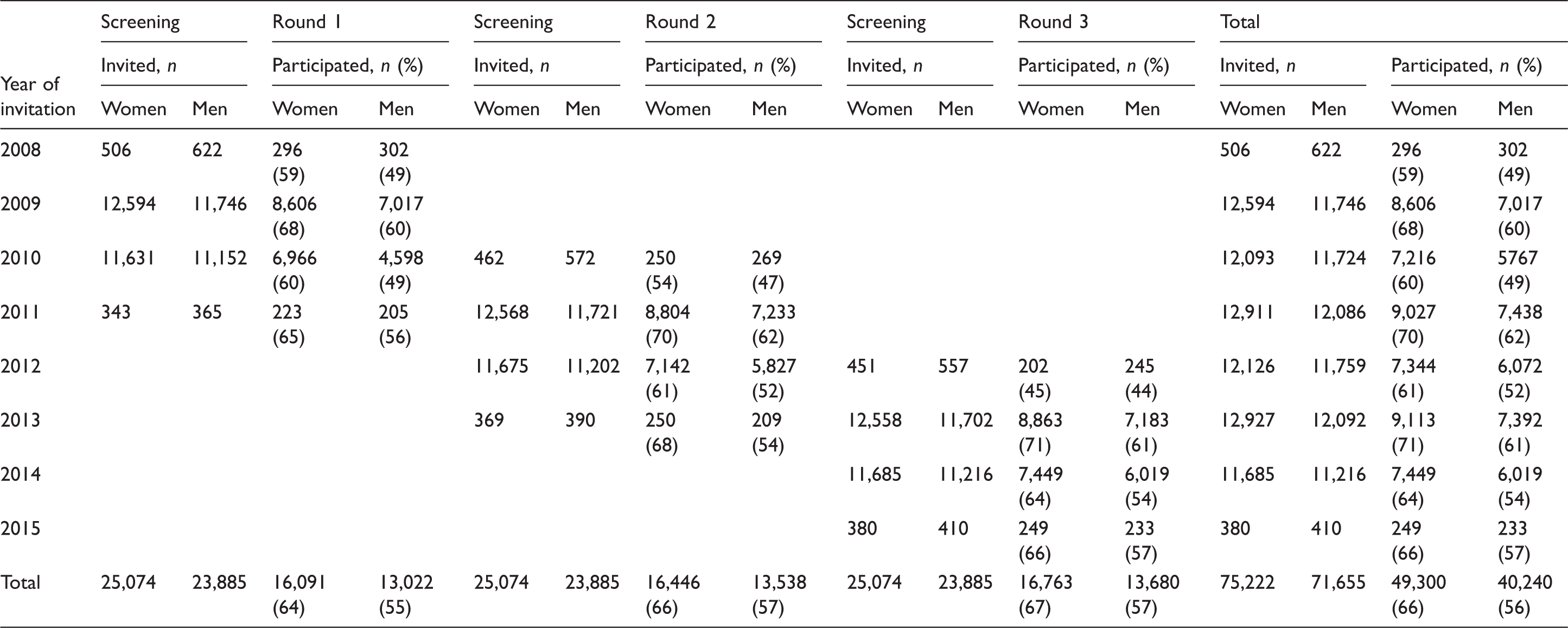
Participation in three complete screening rounds, women and men separately.
Patterns of participation in individuals with three complete screening rounds.
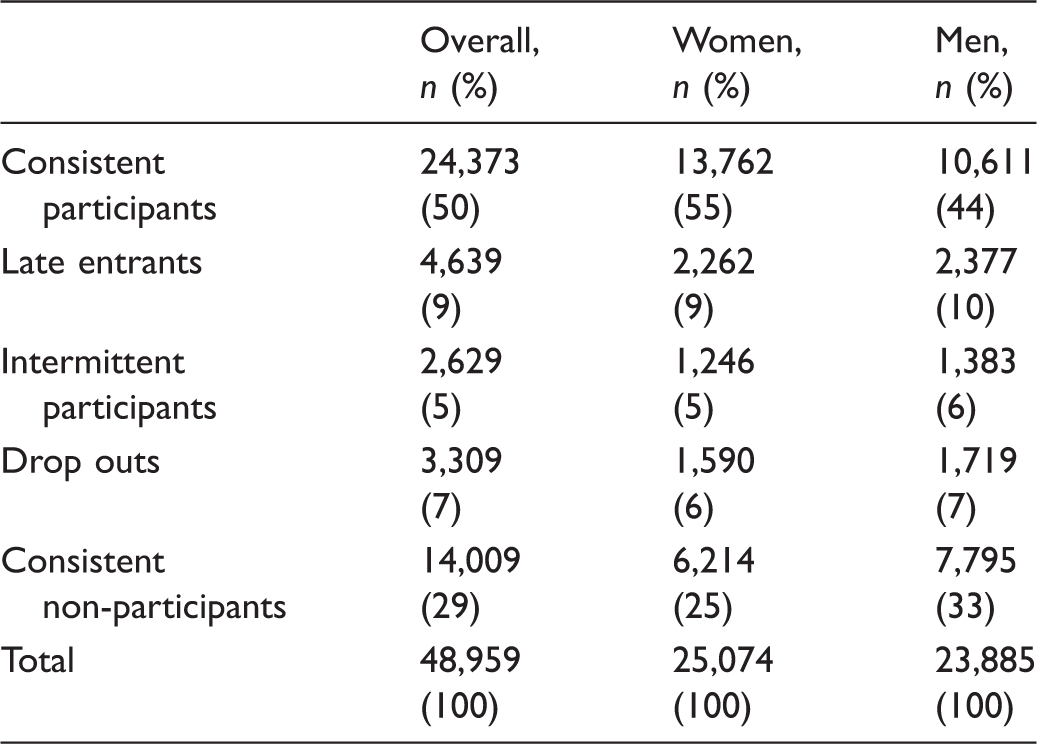
Patterns of participation in rounds 1–3.
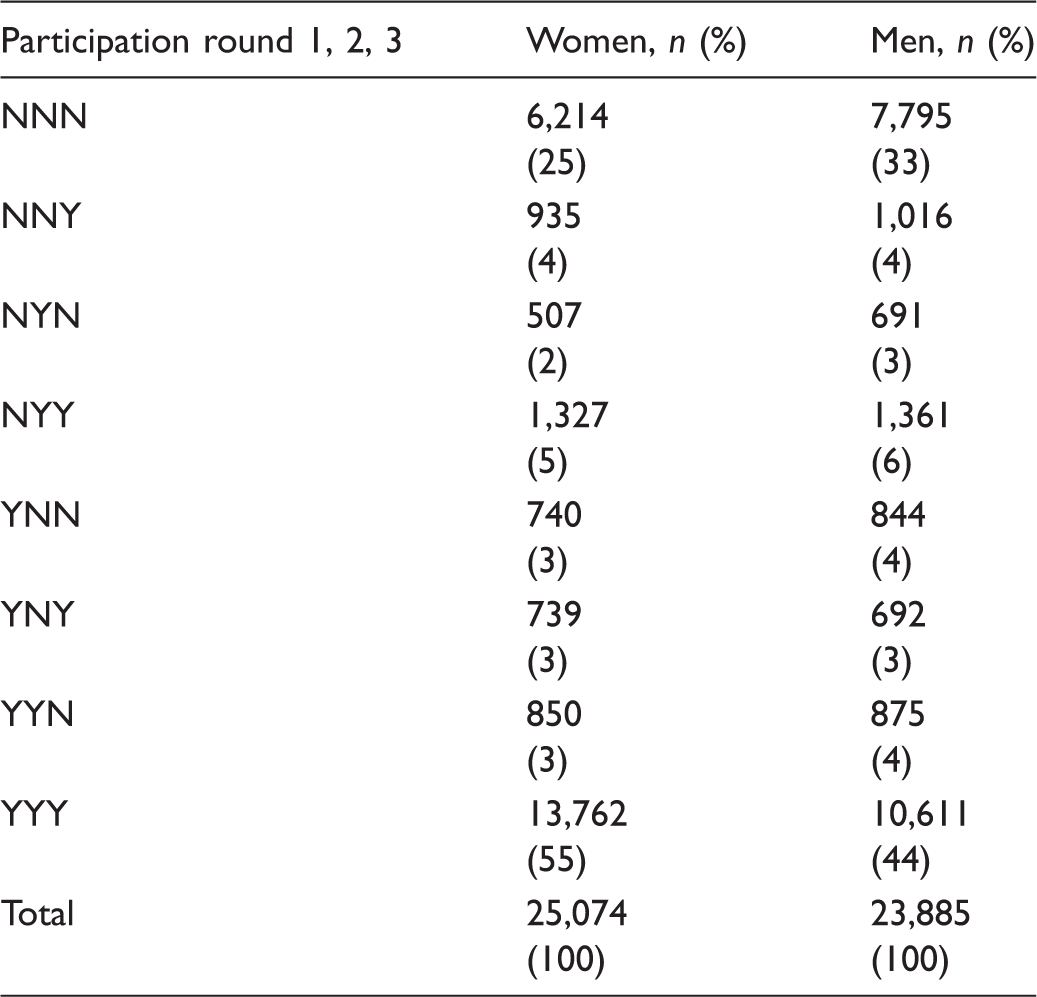
N: no participation; Y: participation.
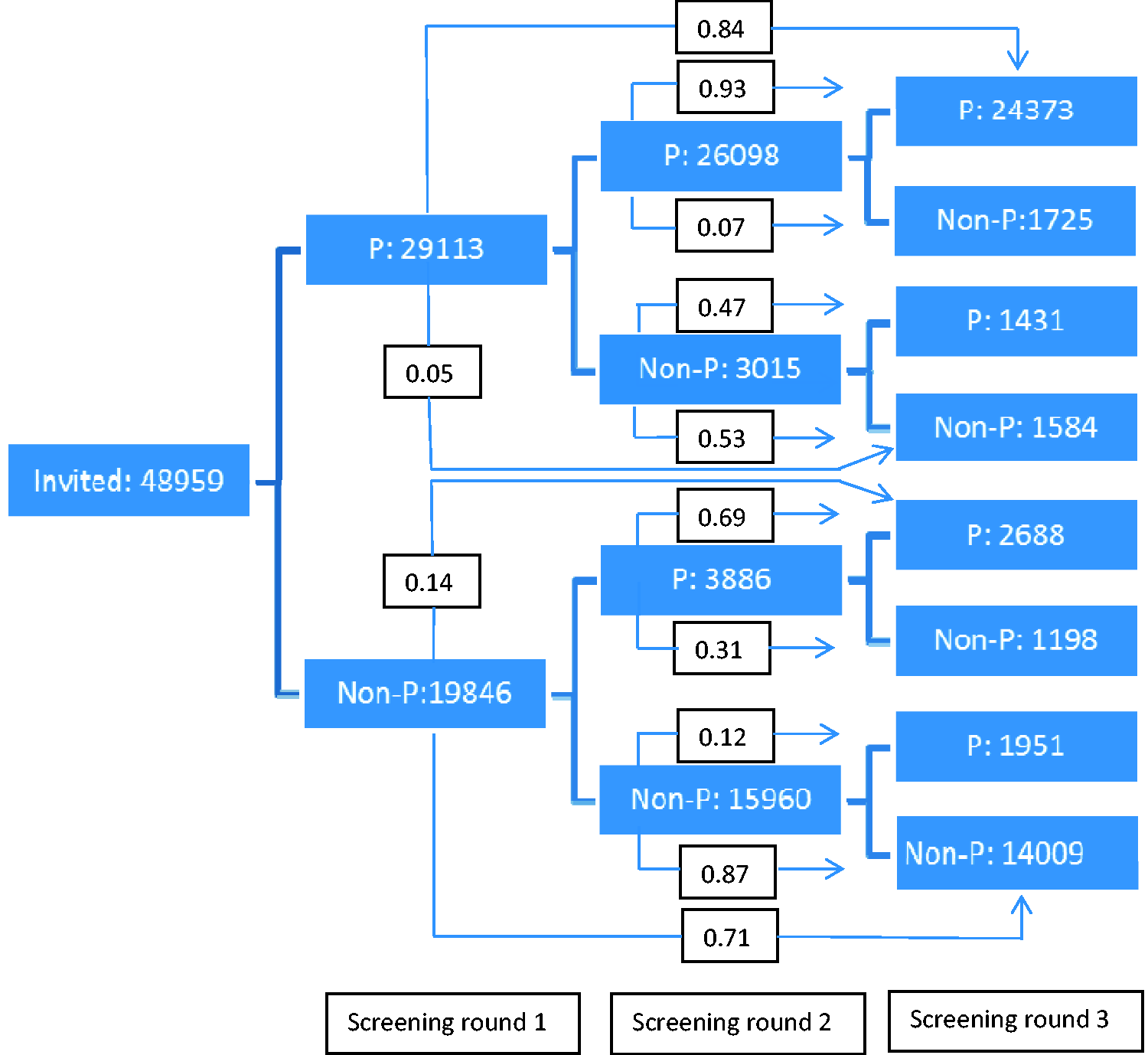
Likelihood of participation in following screening rounds, depending on participation in previous rounds. P: participant; Non-P: non-participant.
Discussion
Understanding factors affecting screening behaviour is important because participation ultimately determines the efficacy of a screening programme. Analysing the patterns of participation and non-participation among individuals invited to screening can help us better understand how to intervene and modify the programme to increase willingness to participate.
In this study, the overall average participation rate was 60%. Initial participation was a strong predictor for continuous participation, and the likelihood of consistent participation was 84% if the individual participated in the first screening round. Of those who attended the first and second rounds, 93% also participated in the third round. For non-participation, similar patterns of consistency were seen. For individuals not participating in the first screening round, the likelihood of constant non-participation was 71%.
The participation rate in this programme was higher than that in the biennial gFOBT Scottish programme, which reported a 39% rate of consistent participation, 65% participating at least once and a consistent participation rate of 60% among those who attended. 8 The English biennial gFOBT screening programme reported that similar to our findings, 70% of individuals invited to screening participated at least once, and that initial participation was correlated to continuous participation. 9 A similar distribution of participation patterns was seen, with consistent participants being the largest group, consistent non-participants the second largest, followed by late entrants. 9 The same distribution between groups was also reported from the population-based South Australian programme, reporting from two rounds with FIT. 2
Average participation rates in the Stockholm/Gotland study were higher among women than men (65% vs. 55%), which has been demonstrated in both trials and programme reports.1,10 Socio-economic background factors and deprivation are known to influence participation,4,11 but were not evaluated in this study. Age was also not evaluated, as the age span in this screening programme is small (60–69), and it is difficult to motivate any clinically relevant sub-categorization of age in this cohort.
This study illustrates that an individual who complies with a screening invitation is likely to continue participation, irrespective of invitation round. Individual background factors such as sex, age and socio-economic status are set, and will not be influenced by measures taken in a screening programme. However, participation follows a pattern, and screening participation behaviour seems determined by initial participation.
In population-based screening, it is questionable whether special adjustments should be made to reduce barriers for participation for different subgroups of individuals, as the screening opportunities offered should be equal and egalitarian. The remaining key option, therefore, is to eliminate, or at least reduce, barriers for initial participation for all, and thus promote socialization into a ‘screening participation behaviour’. The test procedure itself, which requires the repeated handling of stool at home, can be a reason for reluctance and a barrier for initial participation. Qualitative studies have demonstrated that perceived difficulties in accepting, handling or understanding the testing procedure can contribute to non-participation.5,6 The test and the screening procedure itself must therefore be smooth and easy, with as little inconvenience as possible for the invited individuals, in order to facilitate collecting and dispatching the sample. Replacing gFOBT with FIT, requiring only one collected stool sample per test, can be one of the measures taken in order to improve participation. 12
Efforts have been made in England and Scotland to increase uptake through intervention by ‘preformulated implementation intentions’ and questionnaires on ‘anticipated regret’ added to the standard information sent out with the test kits. However, in none of these trials have the interventions increased the overall uptake.13,14
How to intervene to enhance participation among low- and non-participants, and to improve participation overall, remains a central issue to explore. Measures taken in the Stockholm program to promote initial participation include a change from gFOBT to FIT in October 2015, development of a more easily understood and self-instructing icon-based information kit for the FIT-test, and having a central coordinating nurse available by telephone and email daily for questions from individuals invited to screening.
Conclusion
Participation in population-based CRC screening follows the same type of pattern for women and men, albeit with a higher proportion of women participating. Initial participation is a strong predictor of continuous participation and, likewise, initial non-participation is a strong predictor of continuous non-participation. Reducing the barriers for initial participation is a key issue to consider, regardless of individual background factors in the screening population.
Footnotes
Acknowledgements
We thank Jacob Järås of the Regional Cancer Centre, Stockholm-Gotland, for assistance with Stata.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support was provided by Regional Cancer Centre, Stockholm-Gotland, Sweden.