
Abstract
Objective
To use results on recall rates from a regional non-population-based breast screening programme to inform practice in a planned national population-based programme.
Methods
We analysed data on rates of recall for further assessment in 27,327 mammographic screening episodes in 2015–2016 in the breast screening programme in the city of Tbilisi, Georgia. Screening was done by two-view digital mammography with double reading in women aged 40–70, and further assessment took place at the same clinic and during the same visit as the initial screening mammogram.
Results
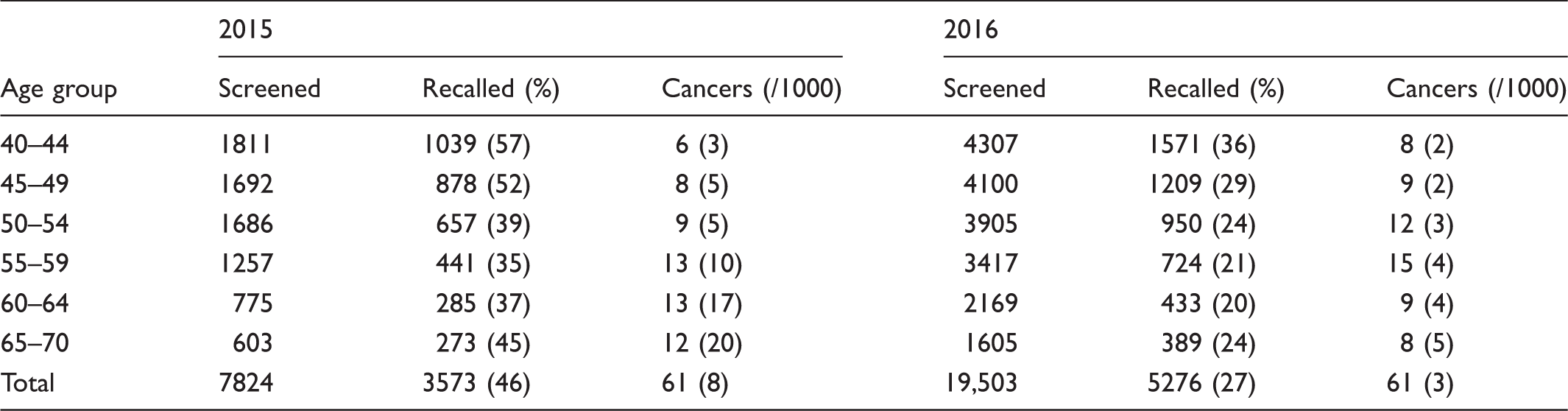
The recall rates were 46% (3573/7824) in 2015 and 27% (5276/19,503) in 2016. Cancer detection rates were 8 per 1000 in 2015 and 3 per 1000 in 2016. Rates of recall were higher in younger women than in older, whereas the rates of cancer detection were higher in older women.
Conclusions
The recall rates, while lower in 2016 than in 2015, are still too high to manage in a nationwide population programme. The use of same-visit assessment is likely to be contributing to this. The national programme should consider separate assessment clinics and carry out audit of recalls to date.
Since the results of the randomized trials of breast cancer screening showing a reduction in breast cancer mortality with mammography screening, many screening services have been established worldwide. 1 Such programmes require monitoring and quality assurance, to maximize the benefits of early detection and minimize risks of false-positive results and unnecessary investigative procedures.2,3 Typically, in Europe, the rates of recall for assessment range from 2 to 15% at first screen, with cancer detection rates of 3–10 per 1000. 2
It is planned to initiate a population-based national screening programme in Georgia, in the Caucasus. In recent years, there has been a regional programme in 18 centres in and around the capital city of Tbilisi. This programme has been advertised on mass media but has not used individual invitation. The programme uses two-view, full field digital mammography with double reading and offers screening every two years. After having their mammogram, the screened women are asked to wait while the mammogram is read. They are then either dismissed with a negative result or asked to undergo further investigation, including cytological sampling or biopsy, and so receive a diagnosis on the same visit as the initial screen.
Numbers screened, recalled and diagnosed with cancer, Tbilisi Breast Screening Programme 2015–2016.
The reason for the very high rates of recall is likely to be multifactorial and may include the relatively recent experience of asymptomatic mammography, professional attitudinal factors, and attributes of the population attending for screening, which may include a large proportion with symptoms. The latter is likely, in view of the very high cancer accrual rate at older ages in 2015. The high recall rates do not seem to be driven specifically by prevalent screens. In 2015, there were 4101 prevalent screens with 1792 (48%) recalls, and 3723 incident screens with 1601 (43%) recalls. The corresponding figures for 2016 were 9461 prevalent screens with 2619 (28%) recalls, and 10,042 incident screens with 2657 (26%) recalls.
It seems likely that a contributory factor is the practice of assessment at the same visit as the screen. Both in Europe and the USA, same-day assessment is associated with higher rates of recall for assessment.2,4 There was a considerable reduction in recall rates in 2016 compared with 2015, but the rates were still high, particularly in comparison with the cancer detection rates. To continue the trend of reducing recall rates, a number of actions should be taken. First, audit of the radiological features prompting recall, in conjunction with final diagnosis, may identify subgroups of radiological features which do not require further assessment. Second, it would be valuable to ascertain presence of symptoms or palpable signs in the recalled population, to determine to what extent the high recall rate is due to symptomatic benign disease. Finally, particularly in view of the greater volume implied by the move to a national population-based programme, the programme provider should consider changing to separate assessment clinics not on the same day as screening.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.