
Abstract
Objective
To provide evidence about the performance characteristics and consequences of bimanual ovarian palpation.
Setting and methods
The Prostate, Lung, Colorectal and Ovarian cancer screening trial randomized 154,900 individuals to either an intervention or control arm. Enrolled eligible participants were aged 55–74, had no history of trial cancers, and no current treatment for cancer. Intervention arm women received CA-125 tests and transvaginal ultrasound. Bimanual ovarian palpation was offered annually during the first four years of the trial. Bimanual ovarian palpation-specific sensitivity and specificity were calculated, as were rates of diagnostic procedures and resulting complications following positive bimanual ovarian palpation screens.
Results
A total of 20,872 women received at least one bimanual ovarian palpation, with 50,498 total bimanual ovarian palpation examinations performed. The sensitivity and specificity of bimanual ovarian palpation were 5.1% (2/39) and 99.0% (49,957/50,459), respectively; no cases were detected by bimanual ovarian palpation alone. Rates for most follow-up procedures for abnormal results in women without ovarian cancer were higher among the group with another screening test positive, except for pelvic exam, where rates were similar. No complications were reported in the bimanual ovarian palpation-only positive group.
Conclusion
Low sensitivity of bimanual ovarian palpation alone and in combination with other tests argue against using bimanual ovarian palpation as a screening test for ovarian cancer in asymptomatic women.
Keywords
Bimanual ovarian palpation (BOP) is frequently conducted in asymptomatic women as a component of their pelvic examination to screen for anomalies, including those suggestive for ovarian cancer. This examination involves palpation of ovaries to feel for unusual growths, masses, or nodules. The United States Preventive Services Task Force (USPSTF) is currently reviewing its recommendations for pelvic exams. 1 Their final research plan includes as key questions the performance characteristics (e.g. sensitivity and specificity) of the pelvic exam and its components in predicting the presence of ovarian and other gynecologic cancers, as well as the adverse effects of screening with the pelvic exam. At present, relatively few studies have assessed these questions.
The Prostate, Lung, Colorectal and Ovarian (PLCO) cancer screening trial 2 was a large randomized trial designed to test whether screening for these cancers reduced cancer-specific mortality. The ovarian component of PLCO included screening with CA-125, transvaginal ultrasound (TVU) and, initially, BOP. BOP screening was discontinued during the trial because no cancers were detected with that modality alone. Nonetheless, a large number of women received one or more BOP exams in PLCO.
In this study, we describe the demographics of these women, the performance characteristics of BOP in PLCO, diagnostic procedures following positive BOP screens, and complications thereof. The goal of this report is to provide further evidence about the performance characteristics of this screening method and potential direct and indirect harms that can inform evidence-based prevention guidelines for pelvic exams.
The PLCO study design has been described in detail previously. 3 Briefly, PLCO was a large-scale, multi-center, randomized controlled trial designed to evaluate the effect of cancer screening for four types of cancer (ClinicalTrials.gov number NCT00002540). 3 Between 1993 and 2001, 154,900 participants were randomized into an intervention or control arm at 10 screening centres. 3 Intervention arm women with at least one ovary received CA-125 blood tests annually for six years and TVU annually for four years. 2 BOP was originally offered annually for four years, but in 1998, it was discontinued because no ovarian cancer was detected solely by BOP. 2 As a result, the number of palpation examinations women received ranged from 0 to 4. Control arm women received usual care according to their health providers’ recommendation. 2 Participant demographics, screening history, and medical history were collected using a self-administered baseline questionnaire at randomization. 2
Positive CA-125 and TVU test results have been described previously. 2 For BOP, a palpable adnexal mass (may include a palpable ovary) or a cul-de-sac nodularity was considered positive. 2 TVU and BOP exams were performed independently, with each examiner blinded to the other’s results. BOP examiners were generally nurses or physician assistants; examiners were required to undergo training with at least 40 exams performed. 4 Diagnostic procedures and medical complications following positive screens were documented from medical records. All subjects were tracked for ovarian and other cancer incidence.
For the purposes of defining test sensitivity and specificity, ovarian cancer was considered present at a screen if it was diagnosed within one year (and prior to any subsequent screen); otherwise, cancer was presumed absent. Sensitivity of BOP was defined as the proportion of screens with ovarian cancer present that were positive on BOP, and specificity as the proportion with ovarian cancer absent that were negative on BOP. Positive predictive value (PPV) was calculated as the proportion of positive screens that had ovarian cancer present, and negative predictive value (NPV) as the proportion of negative screens that had ovarian cancer absent.
Across all positive BOP screens where cancer was absent (i.e. false-positive screens), rates of various diagnostic procedures performed within a year of the screen (including repeat CA-125 or TVU, pelvic exams, and surgical procedures) and rates of resulting complications were computed, overall and by whether the other screening tests (TVU and/or CA-125) were positive.
Of 78,216 women enrolled in PLCO, 39,105 were randomized to the intervention arm and 34,253 were eligible for ovarian cancer screening based on having at least one ovary. Of the 34,253 women, 20,872 received at least one BOP, with 50,498 total BOP examinations performed (mean 2.4 per women). The mean age of these women was 62.9, and 89.1% were non-Hispanic white. Thirty-nine women were diagnosed with ovarian cancer within one year of a BOP screen (and prior to any subsequent screen). The sensitivity and specificity of BOP were 5.1% (2/39) and 99.0% (49,957/50,459), respectively. Of the two true positives with BOP, one was positive for both TVU and CA-125, and the other positive for only CA-125. Both cases were diagnosed at stage IIIC. PPV and NPV were 0.40% and 99.9%, respectively.
Diagnostic procedures and complications within one year of a false-positive palpation screen.
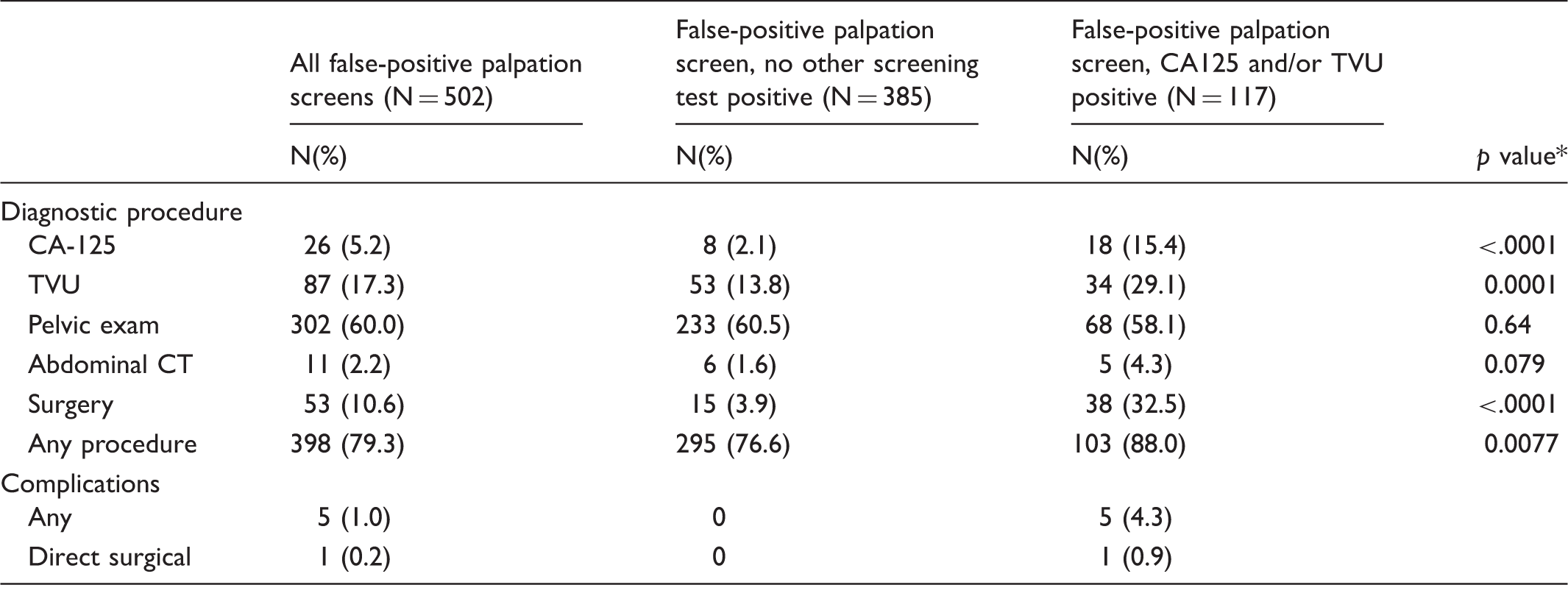
Analyses are on a per-screen basis.
For comparison of procedure rates in false-positive BOP screens with versus without another screening test positive; based on Chi-square test.
In this study of screening with BOP in PLCO, its sensitivity for ovarian cancer detection was very low (5.1%). There is little other evidence on BOP sensitivity; three other studies included a total of five ovarian cancer cases.5–7 Therefore, the current estimate, based on 39 cases, represents the best evidence to date about BOP’s ability to detect ovarian cancer, and this evidence demonstrates that there is little potential for any important benefit of BOP with respect to ovarian cancer.
Nevertheless, BOP, even when CA-125 and TVU were both negative, triggered diagnostic workups for eventual false-positive exams, primarily with repeat palpation or bimanual pelvic examination, but also to some extent with TVU. About 4% (n = 15) of this group (BOP-only positives) received surgery, 11 women received only oophorectomy, and four received both oophorectomy and hysterectomy, highlighting the potential harms of BOP, even though no complications were reported.
In the broader picture of ovarian cancer, as it is the most common fatal gynecological malignancy in the U.S. (about 14,240 deaths annually), 8 screening has been actively investigated as a preventive strategy. PLCO did not find any ovarian cancer mortality benefit of screening with any of the tests, with a mortality relative risk of 1.18 (95% confidence interval: 0.82–1.71). 2 The UK Collaborative Trial of Ovarian Cancer Screening (UKCTOCS), which also utilized CA-125 and TVU, also did not show a significant mortality reduction for its primary endpoint, although mortality reductions were observed in some secondary analyses. 9 Continued follow-up of UKCTOCS is ongoing to examine longer term trends in ovarian cancer mortality across arms.
In conclusion, BOP has very low sensitivity for ovarian cancer and as such its usefulness for ovarian cancer detection in asymptomatic women is doubtful.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Cancer Prevention Fellowship Program (CPFP) at the National Cancer Institute.