
Abstract

In their recent publication on feedback of mammogram-reading performance to screening radiologists, Hofvind et al. 1 list the most typically reported performance measures as reading volume, recall rate, and rate of screen-detected cancers. If the survey question on which performance measures were included in the audit feedback was of the structured or fixed-response type, and if the survey is repeated in the future, we suggest the addition of early rescreen rate to the possible response options.
Early rescreen, the non-standard practice of inviting women for rescreen mammography at shorter than nominal time intervals, is due to mammographic and patient-reported conditions which are associated with increased breast cancer risk or an increased risk of false-negative mammography result (or both). Early rescreen is a psychological burden with no demonstrated benefit. European breast screening guidelines recommend that it be avoided or restricted to <1% of screened women. 2 Whether screening radiologists comply with this recommendation is unknown. To our knowledge, the early rescreen rate is not included in the published data from any screening program, and only two ad-hoc investigations have been reported (from the United Kingdom 3 and Italy 4 ).
In an update of the Italian study, we evaluated the time trend in the early rescreen rate in the Emilia-Romagna two-yearly, two-view, double-reading mammography screening program. The program was implemented between 1996 and 1998. The study period was 1997–2008. We used data collected in 2012 for a study on the proportional incidence of interval breast cancer, processed, and analysed as described previously. 5 Early rescreen rate was defined as the rate of negative mammography records containing the radiologist’s indication that the woman should be re-invited to screening before two years.
Of 549,018 women undergoing one or more mammography screens, there were 1,548,169 eligible negative mammography records. Over the study period, the early rescreen rate was 1.3%, with a range between health district screening units of 0–6.0%. The indicated time interval was 12 months in 93.0% of instances. The rate decreased with increasing woman’s age (50–54, 1.9%; 55–59, 1.2%; 60–64, 1.1%; 65–69, 0.9%; χ2 test for trend, P = 0.000), and was lower at second and subsequent screens (Mantel-Haenszel odds ratio stratified by age, 0.75; 95% confidence interval, 0.73–0.77). As shown in Figure 1, jointpoint regression analysis of the annual district- and age-adjusted early rescreen rate identified a significant constant trend over time, with an average annual increase of about 10% and an estimated rate of 2% in the most recent year of observation – a figure that cannot be ignored.
Number of women with negative screening mammography result by calendar year, time trend in early rescreen rate adjusted for district screening unit and woman’s age, and time trend in jointpoint-estimated early rescreen rate.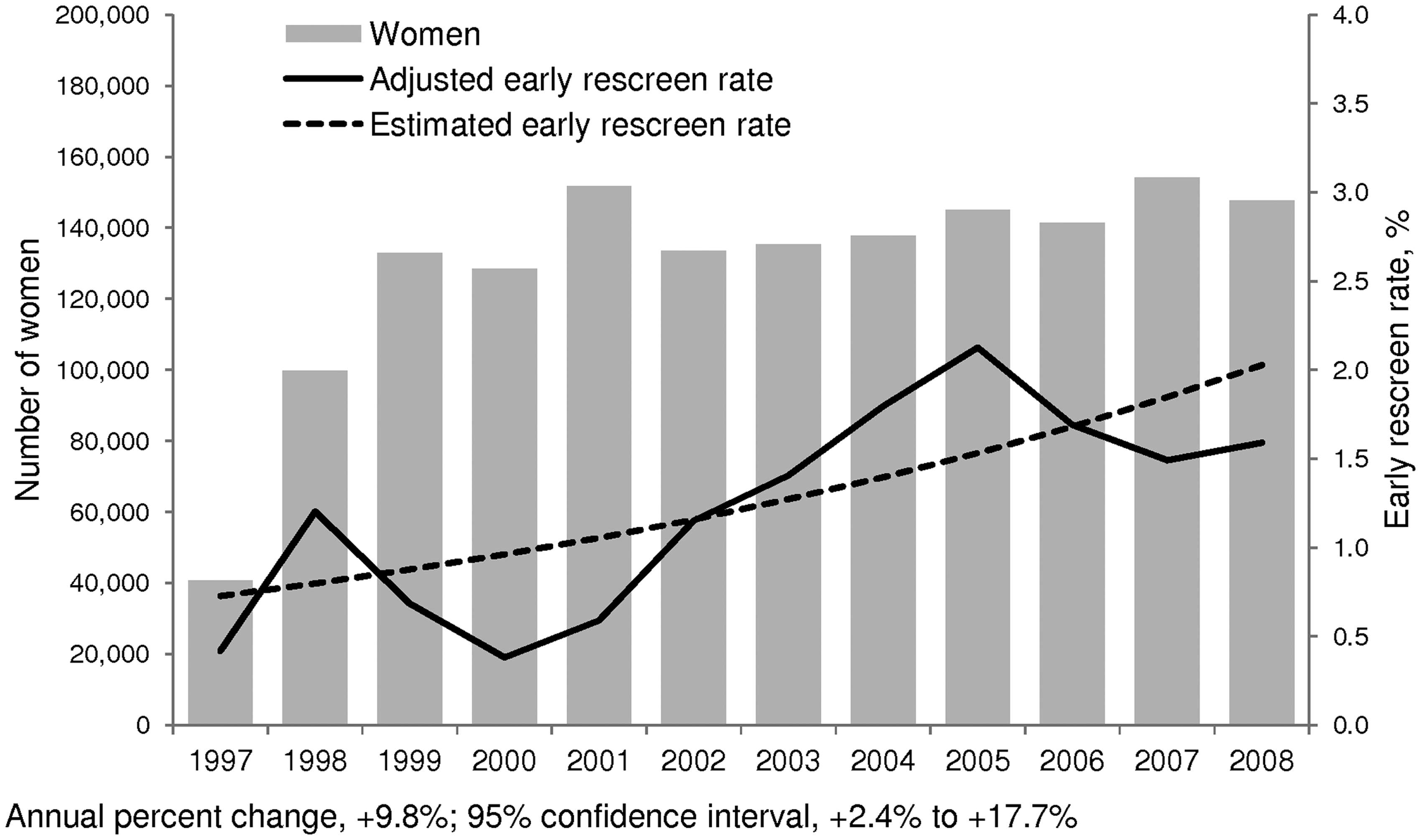
We hypothesize that this trend reflects interaction between a progressive decrease in the level of experience of screening radiologists (due to retirement of experienced personnel and utilization of non-dedicated radiologists – a common situation in Europe), and the gradual introduction of digital mammography (with improved detectability of microcalcifications and increased prevalence of breast abnormalities). The early rescreen rate probably reflects an attempt to increase or maintain the sensitivity of mammogram reading, while simultaneously limiting the recall rate, which has been stable over many years. Other factors, including hormone replacement therapy use, which increases both mammographic breast density and breast cancer risk, but which declined among Italian women during the study period, are unlikely to have played a role.
Early rescreening deserves greater consideration by the mammography screening community, and providing feedback on this to radiologists would improve their awareness of the problem.