
Abstract
Objective
To evaluate the repercussions of recent changes to the cut-offs used in the first screening step of the pre-marital screening programme for thalassaemia prevention in Iran.
Methods
The profiles of 984 subjects referred to a genetic laboratory, and the tests of 242 parents of children with thalassaemia major were assessed for red blood cell (RBC) indices, haemoglobin (Hb) A2 levels and results of Hb electrophoresis.
Results
Of 407 suspected thalassaemia minor (STM) cases, 18 proved positive for thalassaemia minor on molecular analysis (18/407, confidence interval 2.6–6.9%). If the revised screening cut-offs had been used to determine who would undergo molecular analysis, two of these cases would not have been identified. Only 4.4% of suspected cases with lower than normal RBC indices (mean corpuscular volume <80 fl and mean corpuscular Hb <27 pg) and HbA2 (<3.5%) were diagnosed with thalassaemia minor.
Conclusion
The thalassaemia major prevention programme is performed in two separate steps. One step involves the screening of subjects and identification of β-thalassaemia minor, suspected cases for thalassaemia minor (STM), and normal subject groups. The other step concerns the identification of thalassaemia minor in the STM group. Changing the cut-offs at the first screening step does not result in significant improvement from an economic view, and is associated with significant risk at the second screening step.
Introduction
Cut-off details of the thalassaemia prevention programme in Iran (fourth edition).
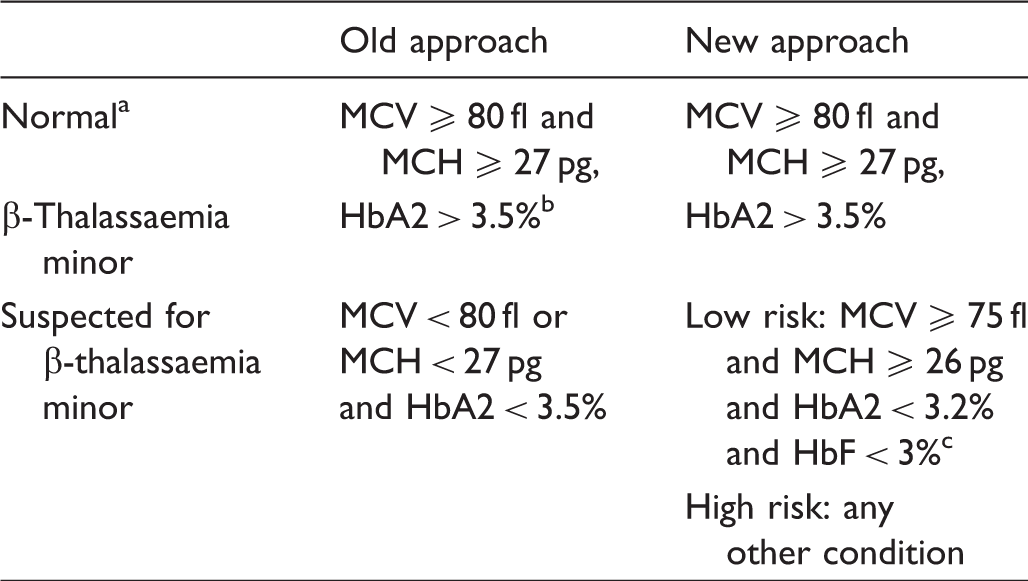
If MCV ≥ 80 fl and MCH ≥ 27 pg, there is no need to check HbA2.
HbA2 must be checked by column chromatography and should only be checked if MCV and MCH are lower than 80 fl and 27 pg, respectively.
HbF must be checked by capillary electrophoresis.
To address these problems, a fourth revision of the thalassaemia screening programme was issued in September 2014 (Table 1; Figure 1), with changes intended to expedite the determination of the state of subjects, and reduce the number of cases referred for molecular examinations. Under the fourth revision, people with RBC indices close to normal are classified as having “low risk for thalassaemia minor” (LRTM) (see Table 1). If one subject (regardless of the condition of their partner) is identified as LRTM, the couple is not required to undergo molecular evaluation. The cut-off levels of MCV and MCH for the LRTM group are reduced to 75 fl and 26 pg, respectively (subjects in the LRTM group must have MCV ≥75 fl and MCH ≥26 pg). However, there is no scientific consensus on the appropriate cut-off points of RBC indices when performing thalassaemia screening, and lower cut-off points have been suggested.7–10 Although selecting lower cut-offs for screening reduces administrative problems, it has been unclear whether it leads to missed cases of thalassaemia. We therefore aimed to evaluate the risks of missed cases along with the reduction of cut-offs in RBC indices, as outlined by the fourth revision of the β-thalassaemia prevention programme.
Flow chart for thalassaemia screening (fourth revision). Low risk for thalassaemia minor (LRTM) (MCV ≥ 75 pg and MCH ≥ 27 pg and HbA2 < 3.2% and HbF < 3%), STM: suspected for thalassaemia minor (MCV < 75 fl, or MCH < 27 pg, or 3.5% > HbA2 ≥ 3.2%, or HbF < 3%), subjects with HbA2 ≥ 7% should be referred to haematologist for further evaluation.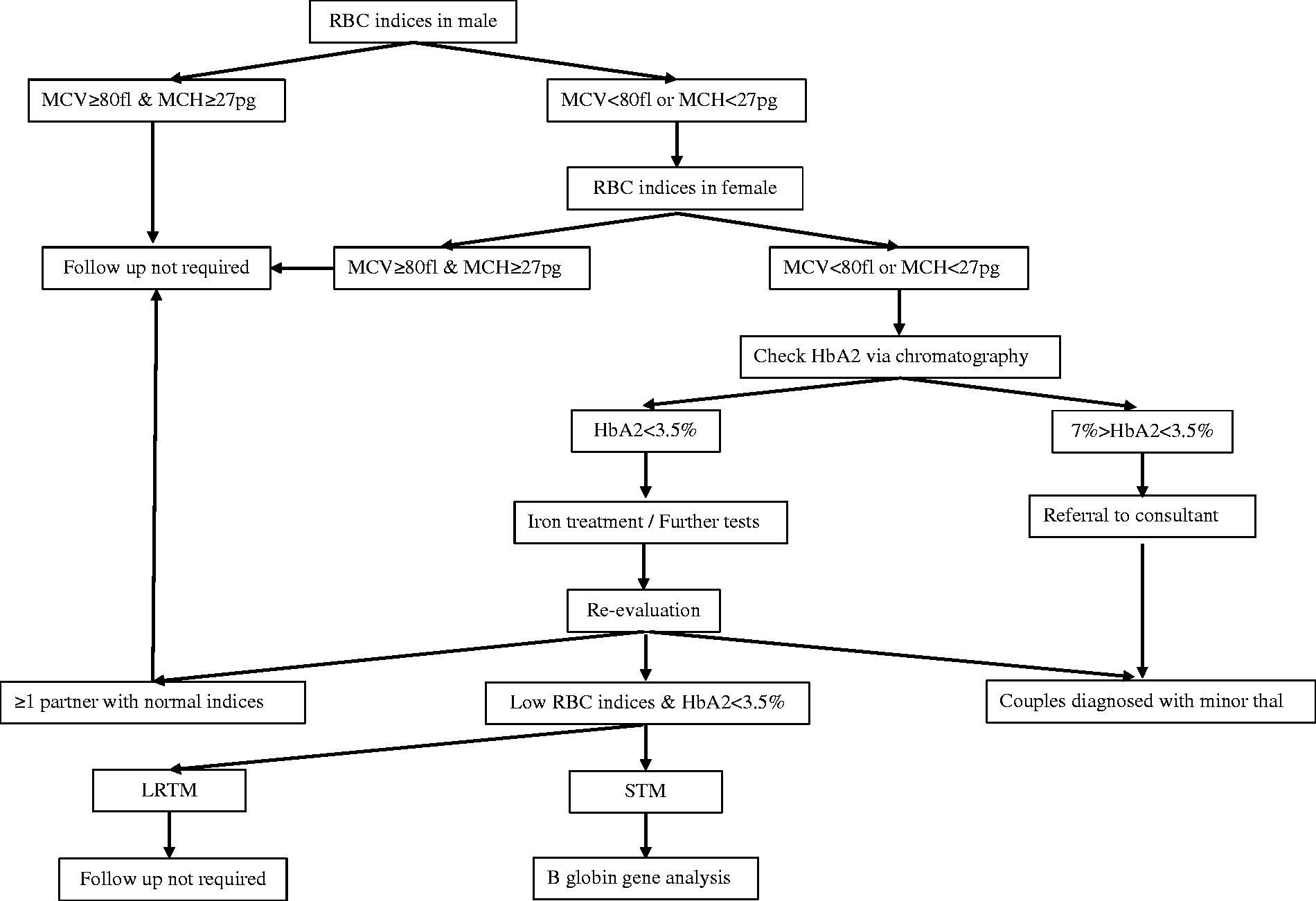
Methods
We carried out a retrospective analysis of 984 subjects from Isfahan province, Iran, referred to the genetic laboratory for detection of any β-globin gene mutations. These included 271 couples referred from a thalassaemia prevention centre for pre-marital screening because of low RBC indices (STM group), 54 subjects by personal request and 194 couples with a known case of thalassaemia and haemoglobinopathies referred for the first step of prenatal diagnosis. We also added the haematologic data of 142 thalassaemia major parents as a random thalassaemia minor group that was not included in any screening programme (married before starting pre-marital thalassaemia screening programme).
STM group (n = 407)
All the subjects in this group were referred to the reference genetic laboratory in Isfahan city during 2011–2013 due to having lower than normal RBC indices and normal HbA2 levels (according to the third revision of the thalassaemia prevention programme), in order to determine the presence or absence of β-thalassaemia using molecular evaluation. RBC indices and HbA2 levels were extracted from files. Although not included in the screening programme, the genetic laboratory routinely performed Hb electrophoresis assay for STM subjects before gene analysis. Therefore, Hb electrophoresis data have been included in this study. This group covers 271 couples. In 135 couples, one of the partners had thalassaemia minor and the other one was STM. Both partners in each of the remaining 136 couples were STM.
Personal request group (n = 54)
These subjects were referred to the reference laboratory in Isfahan city during 2011–2013 due to personal requests (not from a prevention programme).
Thalassaemia minor and haemoglobinopathies group (n = 388)
The subjects in this group were found to have thalassaemia minor or haemoglobinopathies (according to HbA2 levels and Hb electrophoresis), and were referred for beta globin gene analysis at the reference laboratory in Isfahan city as the first step for prenatal diagnosis. These included 191 couples (382 subjects) previously diagnosed with thalassaemia minor, and three couples (six subjects) with specified haemoglobinopathy (confirmed genetically).
Parents of patients with thalassaemia major (n = 218)
This category consisted of the parents of 141 thalassaemia major and thalassaemia intermedia patients in one of the thalassaemia treatment centres in Lordegan, a city west of Isfahan provenance (data from some parents were not available). RBC indices, HbA2 levels and Hb electrophoresis of parents were extracted from their files. Information about the subjects, such as age, sex, RBC indices, Hb electrophoresis, HbA2 levels and data of the molecular tests were also examined.
We analyzed the STM group to assess how the changes in threshold RBC indices for the implementation of the molecular tests between the third (MCV >80 fl and MCH >27 pg) and fourth (MCV >75 fl and MCH >26 pg) revisions of the β-thalassaemia prevention programme would affect the probability of missing a β-thalassaemia diagnosis. We analyzed the other groups to assess the distribution of RBC indices associated with β-thalassaemia minor. Differences between groups were evaluated by using independent sample t tests, Pearson chi-square tests and 95% confidence interval (CI) for proportion.
Results
STM group
Variations of Hb disorders and RBC indices in 46 subjects of the “suspected for thalassaemia” (STM) group.
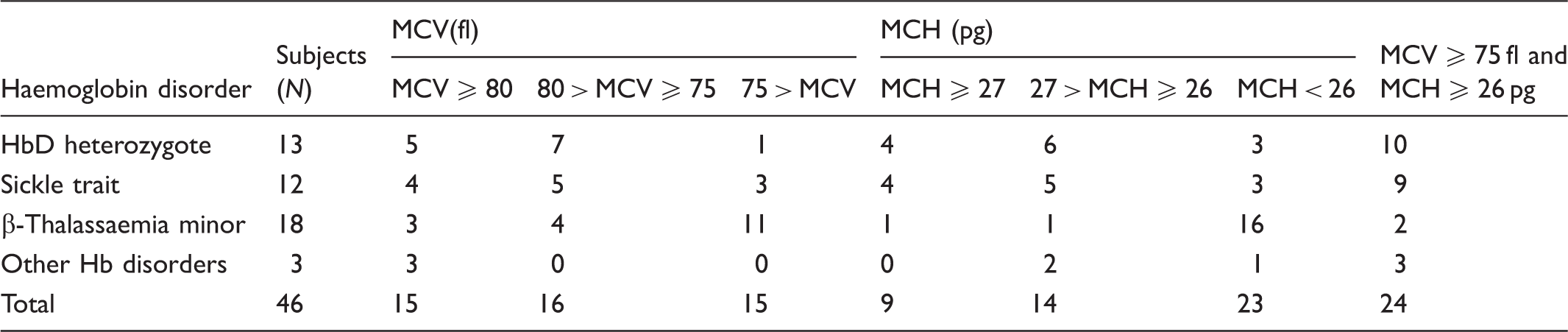
When we applied the threshold RBC indices from the fourth revision of the screening programme, a subset of 187 of the 407 STM subjects (46%) were classified as LRTM (MCV >75 fl, MCH >26 pg, HbA2 <3.2%, and Hb F <3%). This LRTM group included two cases of β-thalassaemia minor, which would have gone undetected by the fourth revision of the screening programme. Haematologic indices for the first case were MCV = 79.6 fl, MCH = 27 pg, HbA2 = 2.4%, and Hb F = 1.1%, and for the second case MCV = 81.6 fl, MCH = 26.9 pg, HbA2 = 2.4% and HbF = 0.5%, with β-thalassaemia mutations IVS110 and -110, respectively.
Predicted haemoglobinopathies in children of couples selected from the STM group according to the RBC indices and Hb electrophoresis.
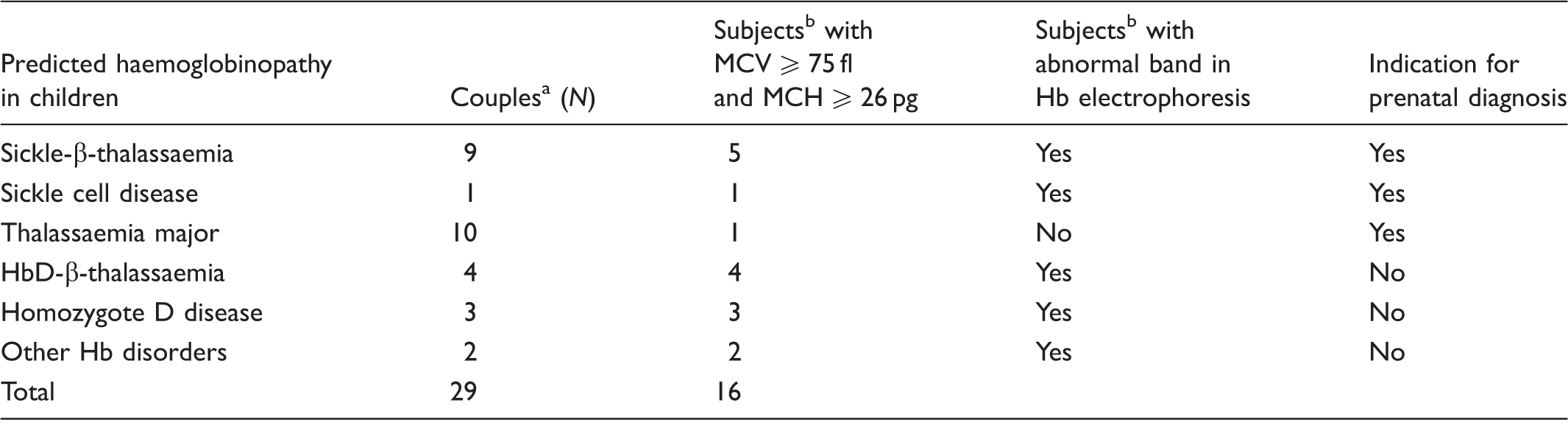
Each couple consists of two partners who both carry β gene mutations.
At least in one partner.
In the STM group, 187 individuals would have been classified as LRTM under the fourth revision of the screening programme. Two of these were confirmed to have thalassaemia minor (1.1% of LRTM versus 4.4% of total STM group; p > 0.05, 95% CI [−0.004,0.026] in the STM group), meaning that 2/18 (11%) of β-thalassaemic individuals in the STM group that would have been detected under the third revision of the screening programme would no longer be detected using the new cut-off values.
Subjects with thalassaemia minor
Among the 984 evaluated subjects, 574 were confirmed to have β-thalassaemia minor; these included 382 subjects in thalassaemia minor group, 135 subjects with a high HbA2 level, and 18 subjects with normal HbA2 level in the STM group, as well as 36 subjects from the personal request group. In six subjects, MCH was greater than 26 pg (with two subjects above 27 pg), and in seven subjects MCV was above 80 fl. One subject, who was known to have family with thalassaemia minor, had MCH and MCV of over 27 pg and 80 fl, respectively (with increased HbA2 levels). Overall, 4.2% of the cases with thalassaemia minor had HbA2 levels lower than 3.5%, and 95.6% of β-thalassaemia minor cases had MCVs lower than 75 fl.
Parents of patients with thalassaemia major
From 218 available cases, there was one subject (mother) with normal RBC indices (silent carrier), and one parent with an MCH of 26.1 pg and MCV of 79.8 fl. Both of these cases had normal HbA2 and Hb F levels, and would not have been detected by the fourth revision of the screening programme; one would be detected by the third revision of the programme. Electrophoresis results from 218 cases showed 14 subjects (6.4%) with normal Hb A2 levels below 3.5%. Two of these 14 parents had MCVs of greater than 70 fl.
Discussion
β-Thalassaemia major is a preventable non-communicable hereditary disease, and given the high prevalence of thalassaemia in certain areas, and the lack of a certain cure (excepting bone marrow transplant), screening has been implemented in many countries.12–14
Most thalassaemia minor cases have HbA2 levels higher than 3.5%. In the Isfahan thalassaemia screening programme, only 3.3% of thalassaemia minor cases had HbA2 lower than 3.5%. 2 In our study the prevalence of thalassaemia minor with low HbA2 levels was 4.2% in thalassaemia minor subjects referred to genetic laboratory, and 6.4% in parents of children with thalassaemia major or intermedia. Other studies support these findings, reporting normal HBA2 levels in only 1–10% of thalassaemia minor subjects. 15 This suggests that the majority of children with thalassaemia major could be detected without expensive molecular tests. Some previous studies confirm the use of RBC indices and HbA2 levels for the first step of thalassaemia screening.7–9 Nevertheless, when molecular examinations were implemented to detect the small percentage of thalassaemia minor people in the STM group in this study (people with low RBC indices but normal HbA2 levels), β-thalassaemia was detected in 4.4% of cases.
The changes to the threshold RBC indices used to determine which individuals should undergo molecular investigation in the fourth revision of the thalassaemia screening programme would result in a seemingly small reduction in diagnosis of thalassaemia for the STM group studied here, from 18 to 16 detections in 407 subjects. Under the fourth revision, 11% of cases with thalassaemia minor in the STM group we studied would not have been detected. Based on previous studies in this province among people referred to counselling centres, 1 of 159 marriages (4412 from 703,082 couples) were referred to the genetic diagnosis laboratory because of suspected thalassaemia. 2 In the population studied here prenatal diagnosis was suggested after molecular tests for 20 of 271 (1/14) couples in the STM group. Potentially, therefore, if molecular tests were not performed at all, 1 in 2154 marriages would have undiagnosed thalassaemia. If, as recommended under the fourth revision, molecular tests are performed for only those in the STM group not deemed LRTM, we would predict that one out of every 21,545 marriages would have undiagnosed thalassaemia. If the goal is to identify all couples at risk of having a child with thalassaemia major, this rate of failure to detect is of concern.
The thalassaemia prevention programme is performed through two separate steps. The first involves an initial diagnosis of, as well as the identification of STM couples. The second step involves the detection of thalassaemia minor in the STM group. When choosing the optimal RBC cut-offs for screening, the steps of the programme being targeted and how these steps are affected must be specified. If there are no facilities for molecular diagnosis, screening for β-thalassaemia trait can be achieved using MCV, MCH, HbA2 levels and Hb electrophoresis. Based on the results from our group of parents of patients with thalassaemia major, this type of screening would lead to a minimum 93.6% reduction of thalassaemia major in our study. In this step, appropriate cut-off points for RBC indices are only essential for deciding whether to perform HbA2 analysis and Hb electrophoresis. HbA2 analysis is simple and low-cost, so reducing the cut-off points does not meet the economic goals of the revised thalassaemia screening programme. The use of these assays as the first step of the thalassaemia screening programme has been reported elsewhere. 16 The other step is to identify subjects with β-thalassaemia minor among the STM group that constitute about 4.4% of this population. To address the high cost and time-consuming nature of molecular tests, changing the cut-offs can reduce the number of people referred to the laboratory, but 11% of thalassaemia minor subjects in the STM group cannot be identified.
Conclusion
The thalassaemia prevention programme comprises two separate steps. The first step involves the screening of couples to detect (i) carriers and (ii) couples in the STM group. The second step is screening for β-thalassaemia minor in the STM group. Our results show that changing the previously established cut-off points for identifying STM individuals is not justified financially or socially, as it increases the risk of thalassaemia incidence in the second step of the thalassaemia screening programme (screening for thalassaemia in the final suspected subjects).
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.