
Abstract
Objective
To investigate pregnancy outcome for fetuses with nuchal translucency (NT) ≥3.5 mm but normal karyotype in the Stockholm (Sweden) area.
Methods
A retrospective population-based cohort study. From 2006 to 2012, fetal NT was measured in 55123 singleton pregnancies. There were 341 pregnancies with NT thickness ≥3.5 mm; 139 had a normal karyotype, 164 had an abnormal karyotype and 38 were removed from the study. Pregnancy outcome was defined as adverse (termination of pregnancy [TOP], miscarriage [MC], intrauterine fetal death [IUFD], or delivery of a child with structural defects or genetic disorders), or favourable (delivery of a child without any structural defects or genetic disorders diagnosed before discharge).
Results
Of the 139 high NT pregnancies with normal karyotype, 110 (79.2%) resulted in live births, one (0.7%) IUFD, 23 (16.5%) TOP and five (3.6%) MC. The risk of an adverse pregnancy outcome increased with increasing NT. Structural fetal defects were found in 28 (19.5%) of pregnancies undergoing second trimester ultrasound screening, of which seven resulted in live births and 21 were terminated. The most common structural defect was cardiac defects.
Conclusions
Adverse pregnancy outcome increased with increasing NT, even with normal karyotype, however, the prognosis is good if the second trimester ultrasound screening is normal.
Introduction
Ultrasound measurement of nuchal translucency (NT) thickness is part of first trimester screening for trisomies 13, 18, and 21.1,2 Increased NT thickness is associated with several other conditions and structural defects, including cardiac defects and a range of genetic disorders and syndromes.3–10 Where karyotype is normal, the likelihood of adverse pregnancy outcome is greater with increasing NT.11,12 While large studies have shown these effects, we sought to repeat the method in a local setting, to determine specific risks and to provide more accurate parental counselling.
Methods
Between 2006 and 2012, 55123 women in the Stockholm area with a singleton pregnancy received an NT measurement as part of first trimester screening for trisomies 21, 13, and 18, at one of seven centres (Center for Fetal Medicine at Karolinska University Hospital in Huddinge, Center for Fetal Medicine at Karolinska University Hospital in Solna, Södersjukhuset, Södertälje Hospital, UltraGyn, UltraBM and Mama Mia Söder). Screening is offered to all women in this region. All certified sonographers are audited annually, and the distribution of their NT measurements must fall within the 40–60 limit compared with the distribution in a larger population. Each NT is measured in triplicate and the median value is used. In our study, none of the sonographers had particularly high or low rates of elevated NT.
Women with a risk ≥1:200 for Trisomy 13, 18 or 21 were offered invasive testing, either by chorionic villus sampling (CVS) or amniocentesis (AC). This was followed by QF-PCR. All pregnancies with an NT thickness ≥3.5 mm (which is above the 99th centile)
13
were offered a complete karyotyping. Of 341 pregnancies with NT measurement ≥3.5 mm, 164 had an abnormal karyotype. Most of these were aneuploidies (Trisomy 21, 13, and 18), but some had structural chromosomal defects such as deletions, and were subsequently excluded from this study. In addition, 38 (11.1%) were later removed from the study (for details, see below). The remaining 139 included in this study had a normal karyotype (determined by either AC or CVS). A flowchart of the study methods is presented in Figure 1.
Flowchart of the pregnancies included in the study.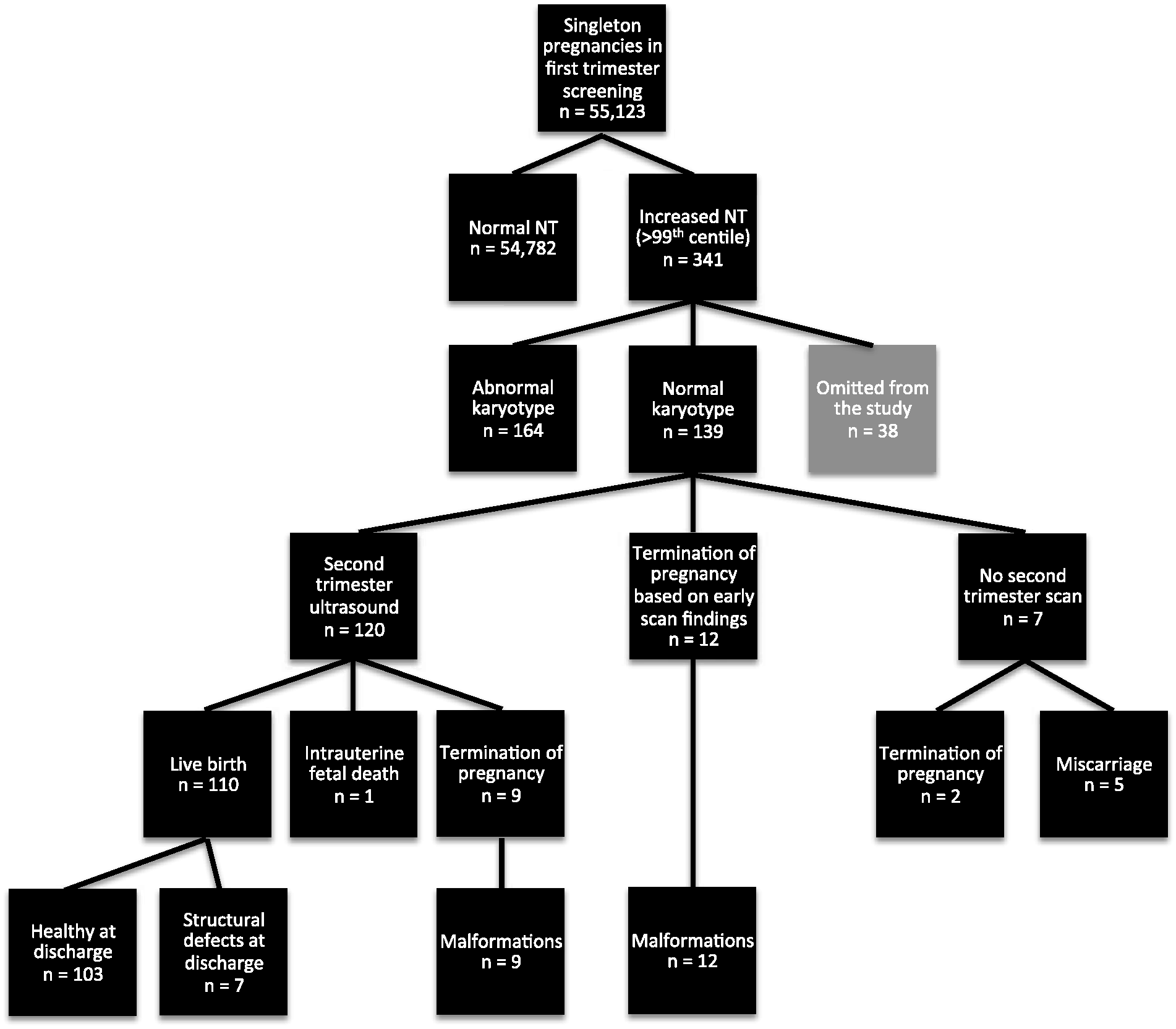
A second detailed ultrasound scan, including fetal echocardiography, to investigate structural anomalies, was offered at 18–20 weeks of gestation. Before discharge after birth, a pediatrician examined the infants.
Pregnancy data were collected retrospectively from our database registry (Obstetrix®). NT thickness, maternal age, prenatal karyotyping, pregnancy outcome, and the condition of live born children until discharge were recorded. The pregnancy outcome was described as live birth (LB), termination of pregnancy (TOP), miscarriages (MC) or intrauterine fetal death (IUFD). Adverse pregnancy outcome was defined as TOP, MC, IUFD or LB with structural defects or genetic disorders, as in the study by Äyräs et al. 14 MC was defined as a fetal loss <22 + 0 gestational weeks and IUFD ≥22 + 0 gestational weeks (the World Health Organization definition). Favorable pregnancy outcome was defined as LB without any structural defects or genetic disorders diagnosed before discharge.
The Central Ethical Review Board in Stockholm, Sweden (Dnr 2011/2007-31/1) approved the study.
Results
NT was increased in 341 (0.6%) pregnancies. In 164 (48.1%) of these, the fetus had an abnormal karyotype; 139 (40.8%) had a normal karyotype. There were 38 cases (11.1%) removed from the study, 34 due to an unknown karyotype and four with normal karyotype who were lost at follow-up. The outcome of the 139 pregnancies studied was 110 (79.2%) LB, one (0.7%) IUFD, 23 (16.5%) TOP and five (3.6%) MC.
Pregnancy outcomes related to NT thickness (mm) in 139 fetuses.
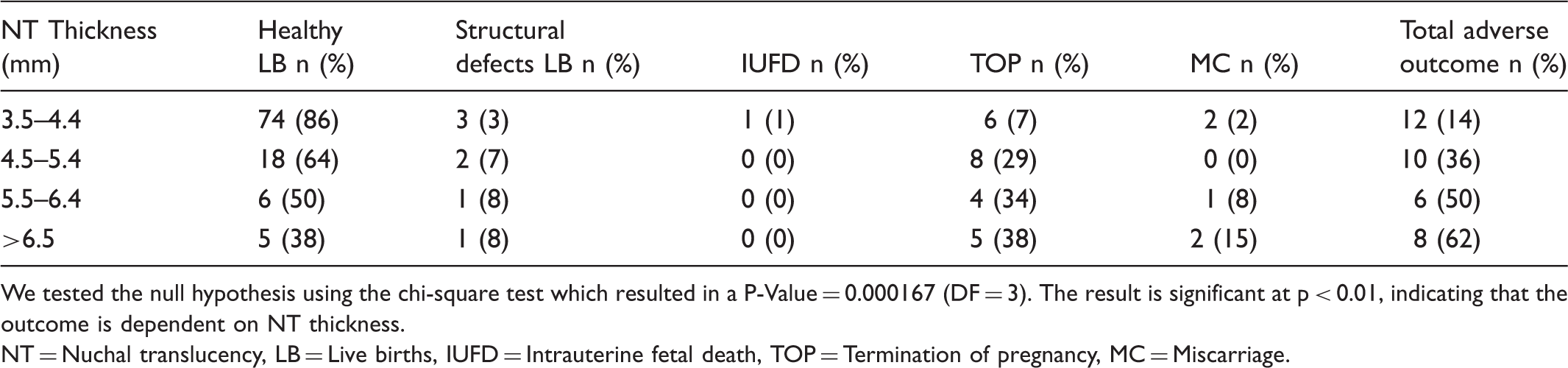
We tested the null hypothesis using the chi-square test which resulted in a P-Value = 0.000167 (DF = 3). The result is significant at p < 0.01, indicating that the outcome is dependent on NT thickness.
NT = Nuchal translucency, LB = Live births, IUFD = Intrauterine fetal death, TOP = Termination of pregnancy, MC = Miscarriage.
Antenatal diagnosis in euploid fetuses with structural defects at birth or TOP.
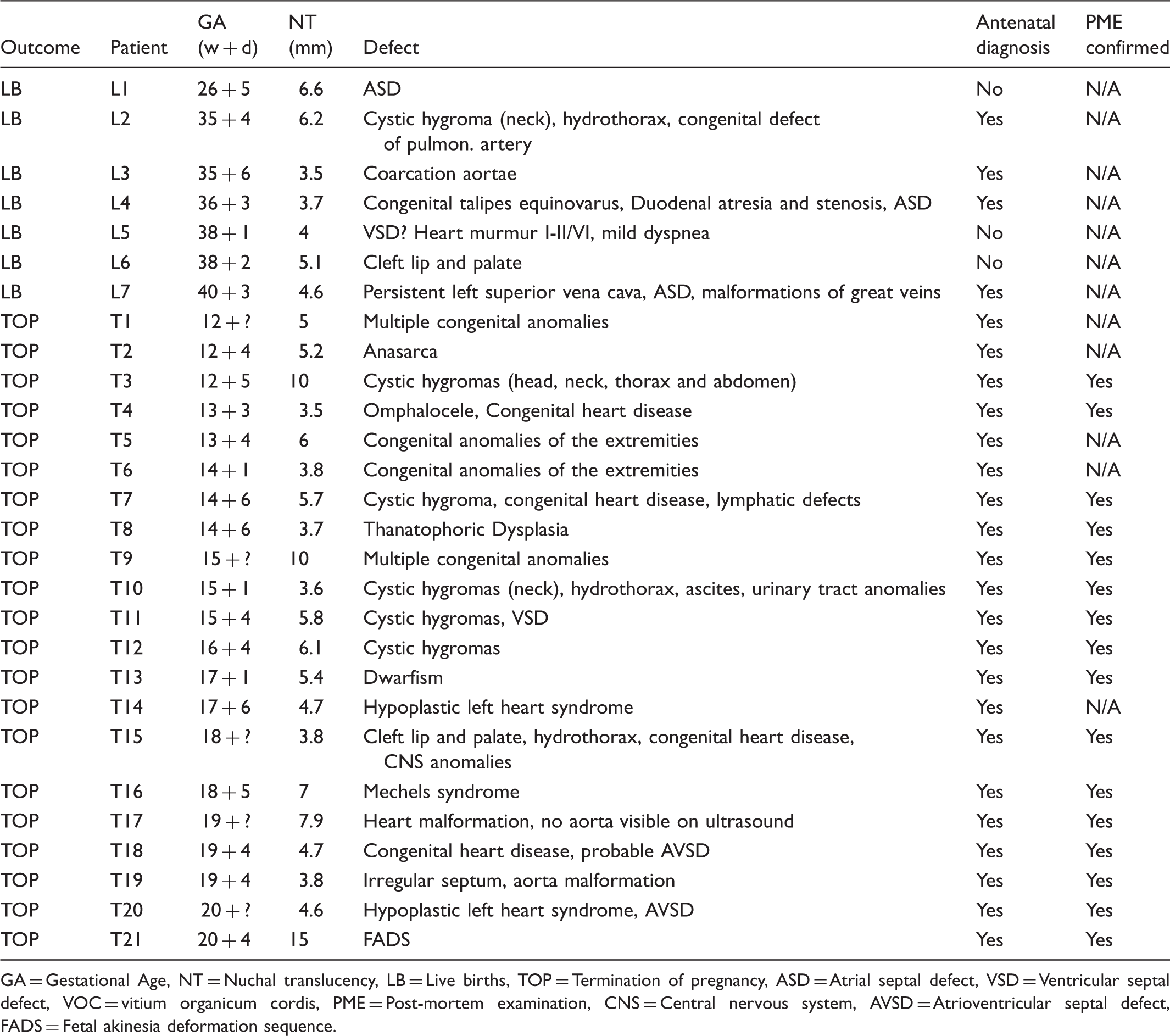
GA = Gestational Age, NT = Nuchal translucency, LB = Live births, TOP = Termination of pregnancy, ASD = Atrial septal defect, VSD = Ventricular septal defect, VOC = vitium organicum cordis, PME = Post-mortem examination, CNS = Central nervous system, AVSD = Atrioventricular septal defect, FADS = Fetal akinesia deformation sequence.
The diagnosis of a fetus with structural anomaly was obtained prenatally in 25 (89%) of the cases (four LB and 21 TOPs). Three (11%) LB were diagnosed after birth (Table 2). Two of the missed cases were heart defects and one cleft lip and palate (Table 2).
In the LB group, 97 (88.2%) babies were born at term, and 13 (11.8%) were premature, seven (6.4% of total LB) born between 32–36 weeks, two (1.8% of total LB) between 28–31 weeks, and three (2.7% of total LB) between 23–27 weeks. Fourteen infants were admitted to the neonatal ward after birth, ten of whom were preterm.
The most common structural defect (55.6%) was of the heart (5/7 LB and 10/20 TOPs). Other common malformations were of the limbs, face, and central nervous system (see Table 2).
Discussion
Several studies5,12,14,15 have shown that adverse pregnancy outcome becomes more likely with increasing NT, and our findings support these results. The overall adverse pregnancy outcome was 25.9% but becomes more likely with increasing NT. We also found, as did earlier studies, that prognosis is good if the second trimester ultrasound screening is normal. The overall adverse outcome risk in our study was increased compared with Ayräs et al and Bilardo et al, where adverse outcome for all fetuses with increased NT was 11% and 19%,14,16 respectively, but our risk was similar to the 23% reported by Souka et al. 17 The less favourable prognosis in our study may be related to the higher NT cut-off level compared with previous studies.
A normal karyotype does not rule out fetal malformations. Increased NT in a euploid fetus is associated with an increased risk of structural anomalies.4,12,16 Of the 23 TOPs, 21 had fetal malformations confirmed by second trimester ultrasound, and the other two terminated before organ screening was performed so it is unknown whether structural defects were present. All women told that the karyotype and second trimester ultrasound was normal continued their pregnancies. While some of the cystic hygroma cases might have been healthy, cystic hygroma is highly correlated with adverse perinatal outcome 18 and this is covered in the parental counselling.
The most common structural defects are cardiac, the prevalence of major cardiac defects increasing with increasing NTs.4,8,12 In our study, the prevalence of major cardiac defects was 11%, similar to that found by Mavrides et al. 19 and Muller et al. 20 but much lower than found by Hyett et al. 21 Like earlier studies,4,14 we found no difference in the NT distributions among different types of cardiac defects.
We observed structural malformations in 28 cases (20.1%), 25 diagnosed antenatally, and five after birth. Seven were LB and had minor structural malformations. The structural malformations found during second trimester ultrasound screening were confirmed by post-mortem examination in 16 of the 21 TOP cases, the remaining five cases diagnosed by ultrasound only. As found in a previous study, 22 we observed a close correlation between ultrasound and autopsy findings, although the previous study also revealed that in almost 40% of cases, post-mortem examination gives additional clinically important information not provided by ultrasound. 22
The main limitation of this study was that newborn follow-up lasted only until discharge, and many structural and genetic disorders are diagnosed in early infancy. We hope to perform a long-term follow-up to investigate whether more LB children have since been diagnosed with conditions or malformations. In addition, ours was a comparatively small cohort, and because 38 pregnancies (11.1%) were omitted, our results must be interpreted cautiously. Of these 38 omitted pregnancies, 34 (10.0%) did not undergo AC or CVS, so karyotype was unknown, and four (1.1%) had normal karyotype but were lost to follow-up due to relocation during pregnancy, as the 21 counties in Sweden do not share the same medical record computer systems. Some details of the 34 that did not undergo AC or CVS are available; 19 resulted in TOP, there were nine MC, five LB (one diagnosed with Down’s syndrome, four considered healthy at discharge), and one relocated during pregnancy. Of the nineteen terminations, seven had post-mortem examinations. In six of these malformations of the fetus were confirmed, and in the other the post-mortem was inconclusive. Karyotyping of the fetus was not performed in any of the seven post-mortems, and none of the MC underwent post-mortem examinations.
A strength of our study is detailed information about pregnancy outcome and the health condition of newborns, confirmed by a paediatrician’s before discharge.
The NT cut-off of ≥3.5 mm (>99th centile; 0.6% of pregnancies in our study) was based on in-house advice from the Department of Clinical Genetics. Our observation of 0.6% of pregnancies having a NT thickness >3.5 mm correlates well with other studies reporting about 1%. In this group the risk of major chromosomal abnormalities is very high, 12 and offering fetal karyotyping by AC or CVS is the first line of management of such pregnancies. If the karyotype is normal, a detailed scan at 19 weeks for the exclusion or diagnosis of both major abnormalities and more subtle defects associated with a known genetic syndrome should be performed. If there are no adverse findings, parents may be counselled that the risk of an adverse pregnancy outcome is not increased. However, almost 12% of these pregnancies in our study resulted in premature delivery, which is two times higher than the Swedish average national rate (6% in 2005). 23 This could be an extra adverse pregnancy outcome, and should be included in the counselling.
From 2015 comparative genomic hybridization (CGH)-array is replacing karyotyping for these patients in our clinics. This array guarantees a much higher resolution (100–1000 times) compared with the karyotype analysis, and can detect copy number variations of small size (even a few hundred base pairs) as well as microdeletion and microduplication syndromes. Understanding the spectrum of array-CGH anomalies detected in the prenatal setting will help to more accurately predict the pregnancy outcome. Future studies will reveal to what extent this new strategy will improve the parental counselling for these patients.
Conclusions
Chromosomal abnormalities and a wide range of fetal malformations and genetic syndromes are associated with increased fetal NT at 11 + 0–13 + 6 weeks of gestation. Our study shows that an increase in the NT thickness in first trimester ultrasound screening is associated with an adverse pregnancy outcome, even when the karyotype is normal. However, in euploid pregnancies with normal second trimester ultrasound findings, a favourable outcome occurs in 74.1% of the cases.
Footnotes
Acknowledgements
The authors acknowledge Dr. Nikos Papadogiannakis, Karolinska University Hospital, Huddinge, for invaluable help with the pathology reports.
Declaration of conflicting interests
None.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.