
Abstract

Two important tumor suppressor genes, BRCA1 and BRCA2, have been identified through family history studies (BRCA1 in 1994 1 and BRCA2 in 1995 2 ). A deleterious mutation in one of these genes confers substantial additional risk for breast (and ovarian) cancer that varies by gene. Between 45% and 65% of women who carry such a mutation will develop breast cancer by age 70. 3 These women could then choose risk-reducing bilateral reconstructive mastectomy and oophorectomy as soon as they have completed their family. Of immediate interest in considering the question posed in this editorial is the finding that deleterious BRCA mutations occur at a much higher rate in Ashkenazi Jewish women (about 1 in 40) than in most other populations (about 1 in 400). In addition, three founder mutations account for nearly all deleterious mutations in this population. 4
In 2014, the United States Preventive Services Task Force (USPSTF) found strong evidence that Ashkenazi Jewish heritage conferred sufficient risk of breast / ovarian cancer to warrant consideration of BRCA testing, even in the absence of a positive family history. The USPSTF recommended against offering BRCA mutation testing generally, not only because of the lower mutation prevalence, but also because of the need for full sequencing of the BRCA1 and BRCA2 genes that would identify many variants. Some of these would be known deleterious mutations (like the three founder mutations) but others would be of unknown clinical significance. These latter findings would leave some women with uncertainty as to both course of action and future risk.
Testing that is limited to the three founder mutations avoids variants of unknown significance and significantly reduces assay costs. If testing for the three founder mutations were to cost $200, the cost per case detected (BRCA mutation carrier developing cancer by age 70) would be about $19,000. 5 This can be contrasted with a hypothetical effort to offer general population testing for BRCA mutations to women in other ethnic groups. 6 In such a circumstance, there would be additional assay costs due to full sequencing and a much lower carrier rate. Together, these factors would increase projected testing costs to $760,000 per case detected.
Reliability of penetrance estimates is an important consideration when determining the extent of added risk conferred by a BRCA mutation and in deciding under which conditions to offer testing. Historically, penetrance has been estimated from women within families with strong family histories (index cases) and this may be biased towards overestimating penetrance. This issue can be addressed by using four specified interdependent epidemiological parameters to evaluate internal consistency of publications reporting results of BRCA testing and breast cancer.4,7 Knowing three of these parameters allows the fourth to be computed. The parameters include: 1) percentage of deleterious BRCA mutations in the population (carrier rate), 2) percentage of mutations among women with breast cancer (clinical sensitivity or detection rate), 3) percentage of women with a mutation who develop breast cancer (penetrance), and 4) overall percentage of women developing breast cancer by a given age (population cumulative incidence). In the Ashkenazi Jewish population, the carrier rate is about 1 in 40 (2.5%), the proportion of breast cancer cases caused by these mutations (clinical sensitivity) is about 10% by age 70, and the population cumulative incidence of breast cancer is also about 10% by age 70. The expected penetrance of 40% can be computed by using the other three parameters, [((clinical sensitivity x cumulative incidence) / carrier rate) = penetrance or ((10 x 10) / 2.5) = 40]. This is consistent with the estimate of 49% from a recent study in Israel that used an innovative study design aimed at avoiding bias of ascertainment. 8
Impact of grandparent ethnicity on the probability of carrying one of three BRCA founder mutations and the associated detection rate.
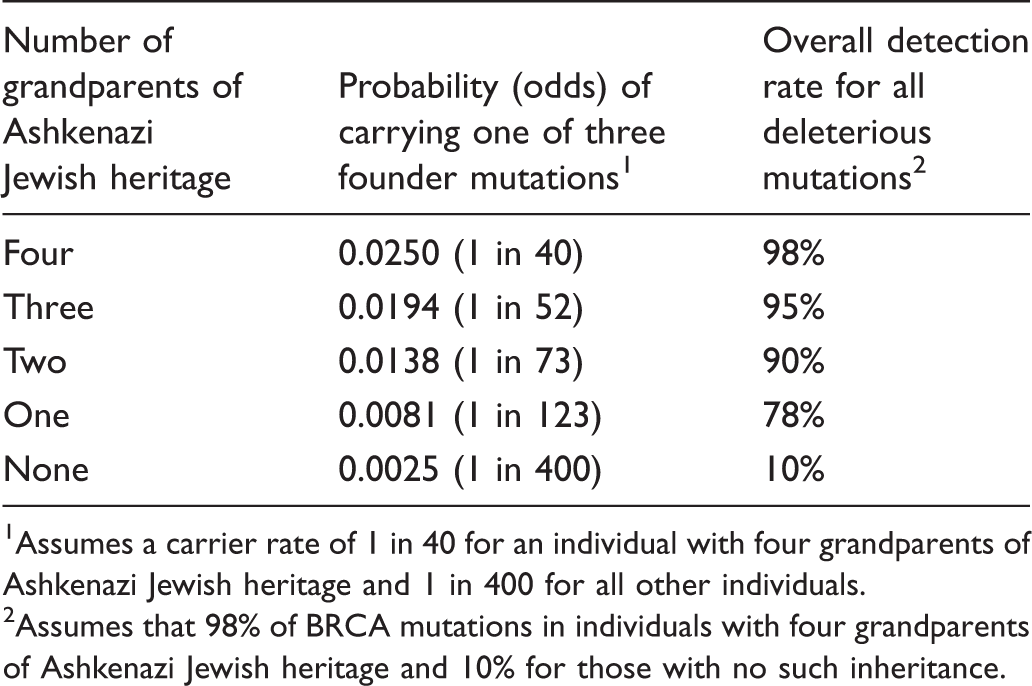
1 Assumes a carrier rate of 1 in 40 for an individual with four grandparents of Ashkenazi Jewish heritage and 1 in 400 for all other individuals.
2 Assumes that 98% of BRCA mutations in individuals with four grandparents of Ashkenazi Jewish heritage and 10% for those with no such inheritance.
Proportion of all BRCA mutations identified by testing only those with Ashkenazi Jewish heritage.
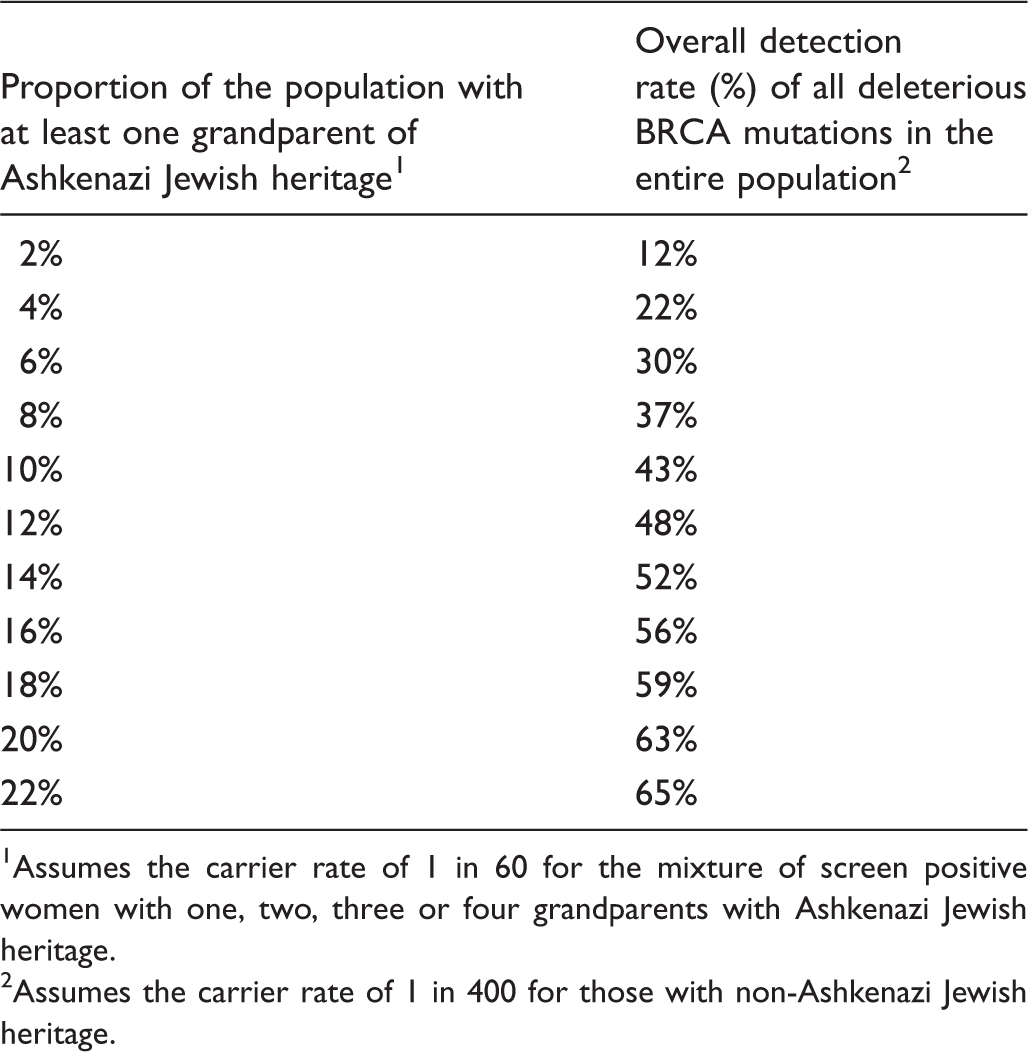
1 Assumes the carrier rate of 1 in 60 for the mixture of screen positive women with one, two, three or four grandparents with Ashkenazi Jewish heritage.
2 Assumes the carrier rate of 1 in 400 for those with non-Ashkenazi Jewish heritage.
In summary, there are now no important gaps in knowledge that would preclude broad-based screening for BRCA mutations when preceded by screening questions regarding age and grandparents’ ethnicity. Demonstration projects would be helpful in documenting initial positive rates on the questions, proportion of screen positive results that may have already had BRCA mutation testing, uptake rate of mutation testing in those who had not been tested, and subsequent decision-making in those with a founder mutation. If such screening were eventually implemented throughout the US, perhaps 4 million (5% of the 81 million females age 30 to 69 in the US in 2013) could be offered screening and approximately 67,000 women with a deleterious mutation could be identified (1 in 60 of the 4 million). This would represent about one-quarter of all adult women that carry a deleterious BRCA mutation.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.