
Abstract
Objectives
Although efficacious treatments for mood disorders are available in primary care, under-diagnosis is associated with under-treatment and poorer outcomes. This study compares the accuracy of self-administered screening tests with routine general practitioner (GP) assessment for detection of current mood disorder.
Methods
197 consecutive patients attending primary care centres in Santiago, Chile enrolled in this cross-sectional study, filling out the Patients Health Questionnaire-9 (PHQ-9) for depression and the Mood Disorder Questionnaire (MDQ) for bipolar disorder, after routine GP assessment. Diagnostic accuracy of these self-administered tools was compared with GP assessment, with gold standard diagnosis established by a structured diagnostic interview with trained clinicians (SCID-I).
Results
The sample was 75% female, with a mean age of 48.5 (SD 16.8); 37% had a current mood disorder (positive SCID-I result for depression or bipolar disorder). Sensitivity of the screening instruments (SI) was substantially higher than GP assessment (SI: 0.8, [95% CI 0.71, 0.81], versus GP: 0.2, [95% CI 0.12, 0.25]: p-value < 0.0001), without sacrifice in specificity (SI: 0.9, [95% CI 0.86, 0.96], versus GP: 0.9, [95% CI 0.88, 0.97]: p-value = 0.7). This led to improvement in both positive predictive value (SI: 0.8, [95% CI 0.82, 0.90], versus GP: 0.6, [95% CI 0.50, 0.64]: p-value < 0.001) and negative predictive value (SI: 0.9, [95% CI 0.78, 0.91] versus GP: 0.7, [95% CI 0.56, 0.72]: p-value < 0.01).
Conclusion
Self-administered screening tools are more accurate than GP assessment in detecting current mood disorder in low-income primary care. Such screening tests may improve detection of current mood disorder if implemented in primary care settings.
Introduction
Mood disorders, including major depressive disorder and bipolar disorder, are among the most common mental illnesses in the United States and developing countries. 1 Initial evaluation often occurs in a primary care setting, where mood disorders frequently go unrecognized.2–4 Some studies point to time constraints in general practice and the competing demands put upon general practitioners (GPs) as the potential cause of such oversight.5,6 In underserved populations, psychosocial problems such as occupational or marital difficulties may monopolize already scarce clinical time, masking symptoms or making thorough assessment difficult. 5
Many people suffering from mood disorders have repeatedly visited primary care facilities without receiving a correct diagnosis. In low-income settings, the average patient with a mood disorder has been evaluated by 8 physicians before the correct mood disorder diagnosis is made. 7 Moreover, the average patient has had symptomatic onset at least 10 years before any mood disorder diagnosis. 8
Major depressive disorder (MDD) is the most common mental disorder seen in primary care patients in developing countries, with prevalence rates ranging from 23%–35%. 9 Some data indicate that about 80% of MDD patients are treated solely in primary care facilities 10 , necessitating adequate diagnostic capability at this level. Epidemiological data show that MDD, a condition usually described as tending to recur chronically over time, is a major public health problem in Chile. 8 In one study examining prevalence rates of MDD in the primary care setting across 15 cities in 5 continents, Santiago had the highest MDD prevalence (27%). 11
Bipolar disorder (BD) is a chronic and recurrent disease that also often goes undiagnosed in primary care settings.12–14 It is the third leading cause of psychosocial disability adjusted life years (DALY, WHO) lost, surpassed only by depression and schizophrenia. 15 Epidemiological studies indicate that the prevalence of bipolar type I disorder in the general population is 1–2%, 13 which is also the case in Chile in the same non-consulting population (2%) according to the Chilean Psychiatric Prevalence Study. 16
Late diagnosis of these disorders may worsen their prognosis. 17 Currently, treatment options are available for mood disorders in primary care facilities, but due to late diagnosis, they are infrequently employed in a timely manner. Thus, new strategies to improve mood disorder detection are badly needed in primary care settings.
The use of self-administered screening tools may be a useful approach, improving detection of current mood disorders, lightening the general practitioner (GP) workload and allowing GPs to attend to other demands. The aim of this study is to compare accuracy of detecting current mood disorders between screening tools and GPs in a low-income population in Santiago, Chile.
Methods
Participants
Subjects were recruited consecutively from given sessions in the general medicine programmes in ten different low-income population primary care centres in Santiago, Chile, between 2009 and 2011. Recruitment sessions occurred as frequently as investigator resources permitted. Patients aged from 18 to 75 seeking primary care medical evaluation for common illnesses were included. In each primary care centre, potential participants were approached in the waiting area and asked if they were interested in a study on “mood disorders”. To participate, patients had to provide informed consent and have a cognitive status enabling them to complete assessments, as determined by a routine clinical mental status examination. Regular clinical assessment of the patients was performed by approximately five general practitioners in each primary care centre, although because of turnover, this list of GPs was not stable during the enrolment period in each centre. GPs selected had a minimum of five years of experience in primary care. The only additional exclusion criterion was the presence of any mood disorder in the period between 6 months and one month prior to study enrolment.
Procedure
A cross-sectional design was used for this prospective study to test two different methods of mood disorder detection by comparing them with a gold standard procedure in a “tandem-testing” manner. 18 After routine assessment by the GP, study investigators administered a protocol including an informed consent and the following self-administered screening instruments for mood disorders: the Patient Health Questionnaire (PHQ-9) 19 for depression and the Mood Disorder Questionnaire (MDQ) for bipolar disorder. 20 Then, blind to PHQ-9/MDQ screening results, a trained clinician applied the DSM-IV Structural Clinical Diagnostic Interview (SCID-I) to obtain mood diagnostic status for each participant. Patients were determined to have mood disorders if they were identified as such by SCID-I depression module or SCID-I bipolar disorder module. Finally, medical records were reviewed examining drug prescriptions (antidepressants, anxyolitics, antibiotics, NSAIDS, others), comorbidities (hypertension, diabetes, COPD, epilepsy, drug/alcohol abuse, obesity). and GP’s mood detection (See appendix 1: Flowchart of patients). The study obtained ethical approval from the Institutional Review Board (IRB) at the Clinical Hospital of the University of Chile.
Instruments
Demographics: A demographic form was used to collect standardized data on age, gender, marital status, and education level.
Determination of GP Assessment: In the last month, any of the following findings in patients’ medical records were counted as positive detection of mood disorders:
Any explicit mood disorder diagnosis. The words that were used to define an accurate diagnosis of each disorder are as follows: “Depression, major depression, major depressive episode, major depressive disorder, depressive syndrome, depressive-anxious syndrome, bipolar, bipolar disorder, manic episode, hypomanic episode, mania, hypomania or bipolar affective disorder”. Any clinical description of mood symptoms in the medical history along with changes in treatment or management of the patient (ie. antidepressant, mood stabilizers or neuroleptics prescriptions and/or mental health professional referral). The list of words included: “low mood, anxiety and low mood, sleep disturbances, insomnia, suicidal thoughts, worry, stress”.
Patient Health Questionnaire (PHQ-9): The PHQ-9 was used to screen for depressive disorders. It is a 9-item self-administered measure of depression, with documented reliability and validity in the sample population. 21 This measure screens for elevated depressive symptoms in the previous two weeks and can be used to measure either presence and/or severity of depression. A score equal to 10 points or higher is indicative of major depressive syndrome. 21 Severity can be categorized as follows: healthy (1-5 pts), subclinical depressive symptoms (6-10 pts), mild depression (11-15 pts), moderate depression (16-20 pts), and severe depression (21-27 pts).
Mood Disorder Questionnaire (MDQ): The MDQ was used to screen for bipolar disorder. 20 It is a 15-item self-administered scale with a score ranging from 1 to 13, also with demonstrated reliability and validity in local studies in primary care. 22 A score of 7 or higher indicates a positive screen for bipolar disorder.
Structured Clinical Interview for DSM-III-R Axis I Disorders (SCID-I) 23 : Administered as the gold standard to diagnose current (last month) major depressive or manic/hypomanic episode. After the GP consultation, clinicians with extensive psychiatric training administered the interview to subjects face-to-face. Training included reviewing the instruments and the DSM-IV, listening to audio recordings of experienced interviewers, practising via role play, observing experienced interviewers in person, and conducting interviews with a supervisor present until interviewers were deemed competent to conduct interviews alone. Interviewers had ongoing (ie. monthly) trainings to reduce rater drift. SCID-I raters also reviewed all interviews with an experienced and accredited trainer and clinical psychiatrist (PAV), who also randomly reviewed cases’ records to check accuracy of researchers assessment.
Data Analysis
Continuous variables were reported as means with standard deviations (SD). Categorical or binary variables were reported as frequencies (%) of the total sample. The primary goal was to assess the degree of agreement between GP assessment and screening tools with the gold standard evaluation (SCID-I), using Cohen’s Kappa statistic. Statistical significance was set at p ≤ 0.05 overall, which leads to 0.025 in individual comparisons. With β of 20% (1 -β = 80% power) and α at 0.05%, using Cohen’s Kappa test, a predicted sample of 140 patients was sufficient to detect a 20% difference between the two procedures (Screening/GP) and the SCID-I. 24 Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and positive/negative likelihood ratio (LR+, LR−) were calculated. When sensitivity of the screening tools was assessed, a negative screen by both the MDQ and PHQ was considered to be accurate when coinciding with a negative SCID-I interview. An accurate positive screen by the screening tools was defined as a positive result by the PHQ-9 or MDQ when in agreement with a positive SCID-I interview for that questionnaire's corresponding disorder (bipolar in the case of the MDQ, depression in the case of the PHQ-9).
Results
Sample Demographics and Clinical Characteristics (n = 197).

Abbreviations: LTR: long term relationship; SCID-I = Structured Clinical Interview for DSM-IV Axis I Disorders, PHQ-9 = 9-item Patient health Questionnaire, MDQ = Mood Disorders Questionnaire, NSAID = Non steroidal anti-inflammatory drugs, EPI = epilepsy, COPD = Chronic obstructive pulmonary disease. *: more than one category could apply. Total sum more than 100%. SD: standard deviation.
Consistent with prior studies, there was a 25% prevalence of major depressive disorder cases (MDD) in this Chilean primary care sample. 11 The sample was predominantly female (75%), as could be expected for patients attending primary care centres in Chile25,26, with a mean age of 48.5 (SD = 16.8). Less than 10% of the sample had reached college level education. Almost half of the enrolled patients lived with their children. The prevalence of chronic illness appeared representative of a primary care population: hypertension was found in 46%, obesity in 23%, and diabetes in 13%.
GP and screening tools assessment agreement with gold standard.
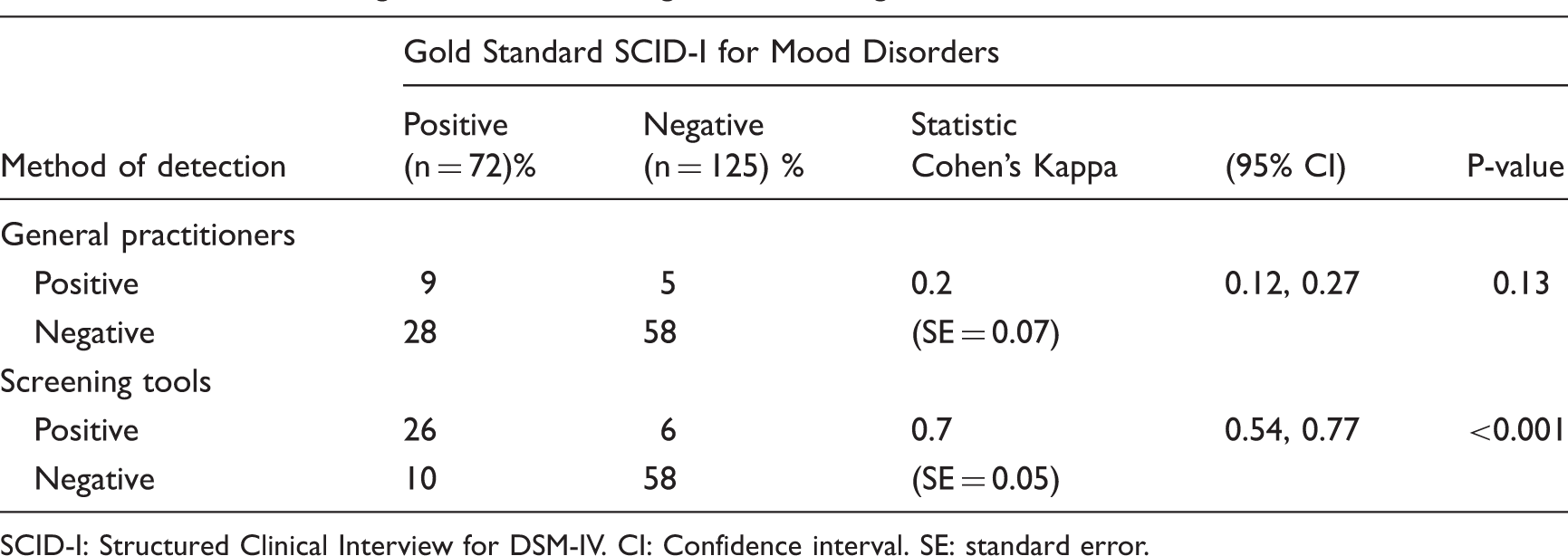
SCID-I: Structured Clinical Interview for DSM-IV. CI: Confidence interval. SE: standard error.
Comparison of sensitivity, specificity, and likelihood ratio of GP’s and screening tools assessment.

CI: Confidence interval.
Comparison of positive and negative predictive values for GP’s and screening tools assessment.
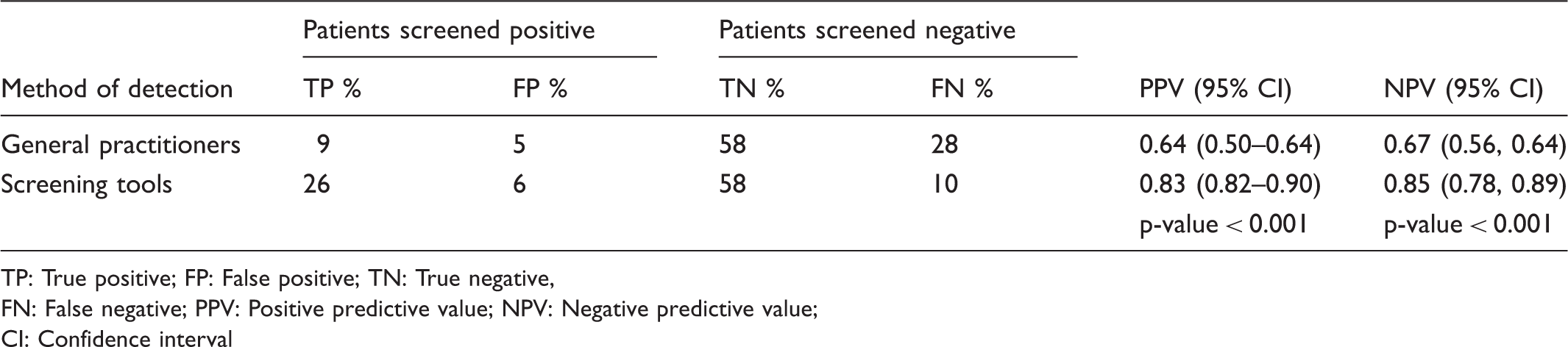
TP: True positive; FP: False positive; TN: True negative,
FN: False negative; PPV: Positive predictive value; NPV: Negative predictive value;
CI: Confidence interval
Taking into account a prior probability of mood disorders of 37% (prevalence of all mood disorders in this population) a positive likelihood ratio (LR+) of 8 [95% CI (6.97, 9.43)] was obtained for screening tools versus a LR + of 2 [95% CI (1.28, 2.72)] for GP assessment (p-value < 0.001). On the other hand screening tools reached a negative likelihood ratio (LR−) of 0.30 [95% CI (−0.43, 1.03)] versus a LR- of 0.92 [95% CI (0.87, 0.96)] for GP assessment (p-value < 0.001). When these measures were applied, if GP assessment was positive, the posterior probability of mood disorders increased to only 51%. In contrast, this posterior probability increased to 81% with positive assessment on mood disorder screening tools. Posterior probability of mood disorder changed little, to 33%, with a negative GP assessment, but decreased notably (14%) with a negative screening tool result (See Table 4).
Discussion
This study sought to compare the accuracy of detection of mood disorders by GP evaluators versus screening tools in a primary care setting with a low-income population. Using a structured research interview as a reference, we found that screening tools outperformed GP assessments considerably, without increasing false positive cases. Previous self-report psychiatric questionnaires have been validated in low-income primary care settings;27,28 however, this is the first time these methods have been compared with GP assessment in low-income primary care in a resource-poor country. We found that almost two-thirds of true mood disorder cases were missed by GP assessment, while the same proportion was correctly classified as having mood disorders by the screening tools. The Patient Health Questionnaire-9 (PHQ-9), one of the screening tools chosen, showed a higher PPV in this sample when compared with previous studies.29–31 One possible explanation for this finding could be the high prevalence of mood disorders in this Chilean population (almost 40%), seen in previous national and international studies.15,21 The likelihood ratios (LR) in our study suggest that screening tools could be useful for clinicians. These results may show how diagnostic accuracy can improve from a prior probability of 37%, baseline prevalence, to more than 80% for positive posterior probability and 15% for negative posterior probability. This may be especially useful in primary care settings where scarce resources and time impede the ability of GPs to explore mental health.
Strengths of this study include several methodological precautions to avoid biases, such as tandem testing diagnostic assessment 18 using a structured interview. Possible cases were approached after GP assessment in order to avoid a biased evaluation of mental health status by GPs. Assessment and accuracy of screening tools was compared with a gold standard, the SCID-I semi-structured clinical interview, unlike almost all prior studies of these screening tools.21,32,33 The gold standard, SCID-I assessment, was blind to screening tool or GP assessment results. The screening tools chosen are well validated and have been previously applied in primary care setting. 34 An expert (PAV) routinely reviewed randomly assessed cases to maintain accurate diagnosis.
Limitations of the study include the following: recruitment bias may be possible since patients with more visits to centres, who may have been more severely ill, were more likely to be enrolled. Moreover, the sample is clinically affected and not representative of the general population. This approach was deemed to be most appropriate due to time and budget constraints; furthermore, it has been used in similar investigations and should best resemble the typical population seen by general practitioners.35,36 Also, assessment of GP diagnostic skills was based only on medical records and conducted without their knowledge of the specific purposes of the study. This approach has a pragmatic and positive aspect of allowing for assessment of real-world practices but it may underestimate the actual diagnostic accuracy of GPs. Effective deployment of this screening method is limited to populations with sufficient literacy rates to enable patient comprehension of self-report questionnaires.
Conclusion
When compared with general practitioner assessment in low-income population primary care settings, screening tools for depression (PHQ9) and bipolar disorder (MDQ) were found to improve mood disorder detection. Thus, these screening tools may enhance detection and general management of mood disorders at the primary care level in low-income populations. Further research is needed to examine the feasibility and outcomes of broad implementation of screening in primary care. Future studies may also investigate assessments for other psychiatric disorders, such as anxiety disorders, that commonly present in primary care settings.
Footnotes
Declaration of interest
In the past 12 months, Dr. Nassir Ghaemi has received research grants from Pfizer and Takeda. Neither he nor his family hold equity positions in pharmaceutical corporations. No other authors have financial conflicts to declare.
Source of Funding
No funding was received for the present study.
Ethical Approval
This study was approved by the Institutional Review Board (IRB) at the Clinical Hospital of the University of Chile, Santiago.