
Abstract
Background
The COVID-19 pandemic significantly impacted the delivery of cancer screening. The resulting decrease in outpatient visits and cancellations of non-urgent procedures have negatively affected colorectal cancer (CRC) screening. We aimed to determine the effect of the pandemic on CRC screening at a safety-net hospital and a private health system based in New York City.
Methods
We identified individuals eligible for CRC screening aged 50 to 75 years presenting for outpatient care at a safety-net public hospital and private health system in April through September of 2019 and 2020. The primary outcome was the proportion of screening-eligible patients seen in primary care who underwent CRC screening.
Results
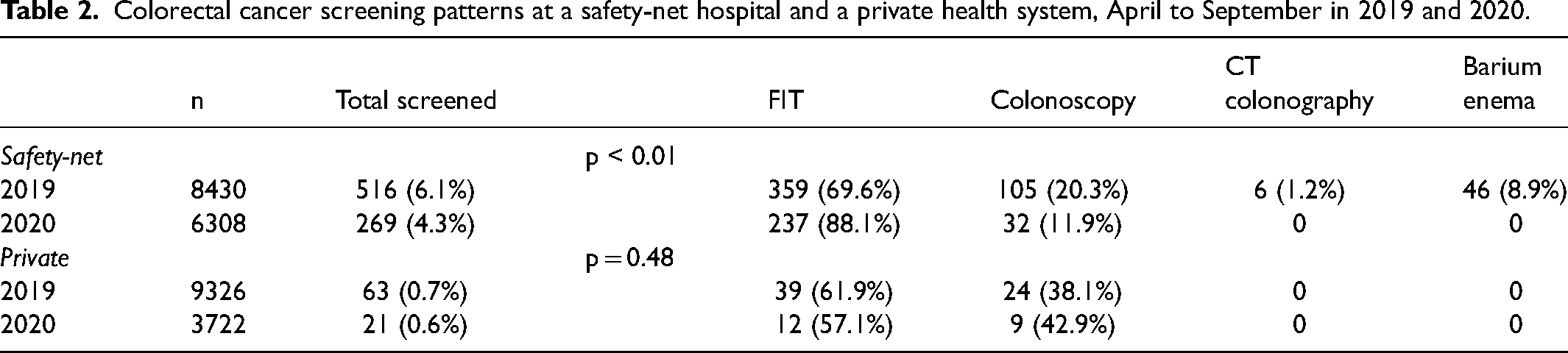
The safety-net hospital had 516 (6.1% of screening-eligible individuals) and 269 (4.3%) screening tests completed in 2019 and 2020, respectively (p < 0.01). Fecal immunochemical tests (FIT) accounted for 69.6% of screening in 2019 and 88.1% in 2020. Colonoscopy accounted for 20.3% of screening in 2019 and 11.9% in 2020. The private health system had 39 (0.7%) and 21 (0.6%) screening tests completed in 2019 and 2020, respectively (p = 0.48). FIT accounted for 61.9% of screening in 2019 and 57.1% in 2020. Colonoscopy accounted for 38.1% of screening in 2019 and 42.9% in 2020.
Conclusion
Absolute numbers of screening tests decreased for both institutions during the COVID-19 pandemic. We observed a decrease in screening uptake and increase in proportional FIT use in the safety-net hospital but no change in the private health system.
Introduction
The coronavirus disease 2019 (COVID-19) pandemic had led to severe reductions in cancer screening globally, as healthcare systems redirected efforts towards both acute COVID-19 surges and minimizing unnecessary contact to decrease transmission. These policy implementations over multiple surges worldwide have led to the cancellation of non-urgent patient visits and procedures, which subsequently impacted cancer screening. 1
Colorectal cancer (CRC) is the second leading cause of cancer-related mortality in the United States. 2 Disparities in CRC screening, diagnosis, and mortality are evident across underserved, minority populations and continue to widen as screening and treatments improve.3,4 In urban settings, specifically New York City, there is evidence of decreased screening colonoscopy use among recent immigrants, low-income groups, and those experiencing homelessness.5,6 These individuals from medically underserved populations are less likely to complete CRC screening, have less follow-up, and have decreased access to CRC treatment. 7
The COVID-19 pandemic has disproportionately affected vulnerable patient populations and has widened the chasm along pre-existing inequities. Studies have shown a significant decline in cancer screening when comparing patient encounters early in the pandemic to the months leading up to the pandemic.8–10 Initial guidelines from the American Society for Gastrointestinal Endoscopy (ASGE) recommended delaying elective procedures (such as screening colonoscopy and follow-up colonoscopy after abnormal stool test) 11 and the American Cancer Society recommended against going to a healthcare facility for routine cancer screening. 12
Our study sought to identify changes in CRC screening patterns in a large urban setting where the initial wave of the pandemic was most pronounced. Outpatient volume has been demonstrably reduced during the pandemic, 13 and because CRC screening is largely opportunistic it requires an outpatient visit. Thus, we aimed to evaluate patterns of screening and follow-up in patients who had at least one outpatient visit during the pandemic. We examined data from two different health systems (a private healthcare system and a safety-net public hospital in New York City) to determine the effect of the pandemic on CRC screening, and whether its impact differed between two health systems with different patient populations.
Methods
Study design and setting
In this retrospective cohort study, we identified patients who received outpatient care at a safety-net public hospital (Bellevue Hospital) and private health system (NYU Langone Health) in New York City. To better compare patients between these health systems we geographically limited the clinics to Manhattan. As a result, we evaluated one primary care clinic at the safety-net hospital and eight at the private health system. For both health systems, we evaluated patients who received care between April to September in 2019 and 2020, with the latter representing the first wave of the pandemic.
Study population
We evaluated patients aged 50 to 75 years who were eligible for screening and had at least one documented primary care outpatient visit (including televisits) during the time periods noted above. We excluded patients if they were up to date with CRC screening before each study period, or had received a prior diagnosis of CRC, a hereditary CRC syndrome, inflammatory bowel disease, or colectomy. Specifically, being up to date was defined as completing a fecal immunochemical test (FIT) within 1 year, colonoscopy within 10 years, flexible sigmoidoscopy within 5 years, CT colonography within 5 years, and barium enema within 5 years of the start of each respective time period for screening purposes.
Patient demographics and screening data were obtained through queries of the Epic (Verona, WI, USA) electronic medical record (EMR) at both institutions. Data regarding CRC treatment were obtained through manual record review of the EMR. Colonoscopies at the safety-net hospital were specifically obtained through manual record review of Provation MD (Minneapolis, MN, USA) endoscopic software.
Statistical analysis
Patient demographics were summarized by health system and year. The primary outcome was the difference in proportion of patients who underwent screening between the two time periods by healthcare system. Secondary outcomes included the difference in sociodemographic characteristics, difference in proportion of patients with abnormal FIT who received follow-up colonoscopy, and diagnosis of CRC within 6 months following the end of each time period. Statistical comparisons were made using chi-squared tests. We used R (R Core Team 2021, R Foundation for Statistical Computing, Vienna, Austria) for all statistical analyses and considered P < .05 as statistically significant.
Results
Patient demographics
Table 1 shows demographic characteristics in the two health systems. A total of 14,738 patients with outpatient visits were eligible for evaluation in the safety-net hospital, with 8430 in 2019 and 6308 in 2020. Insurance coverage was significantly different between 2019 and 2020 in the safety-net hospital, with an increase in Medicare-insured individuals (28.4% vs. 29.6%, + 1.2% difference) and decrease in patients with no or unreported insurance (30.8% vs. 29.9%, −0.8% difference, p = 0.03). Patient characteristics were otherwise not significantly different between 2019 and 2020 in the safety-net hospital.
Demographics of the screening-eligible patient population at a safety-net public hospital and a private health system, 2019 and 2020.
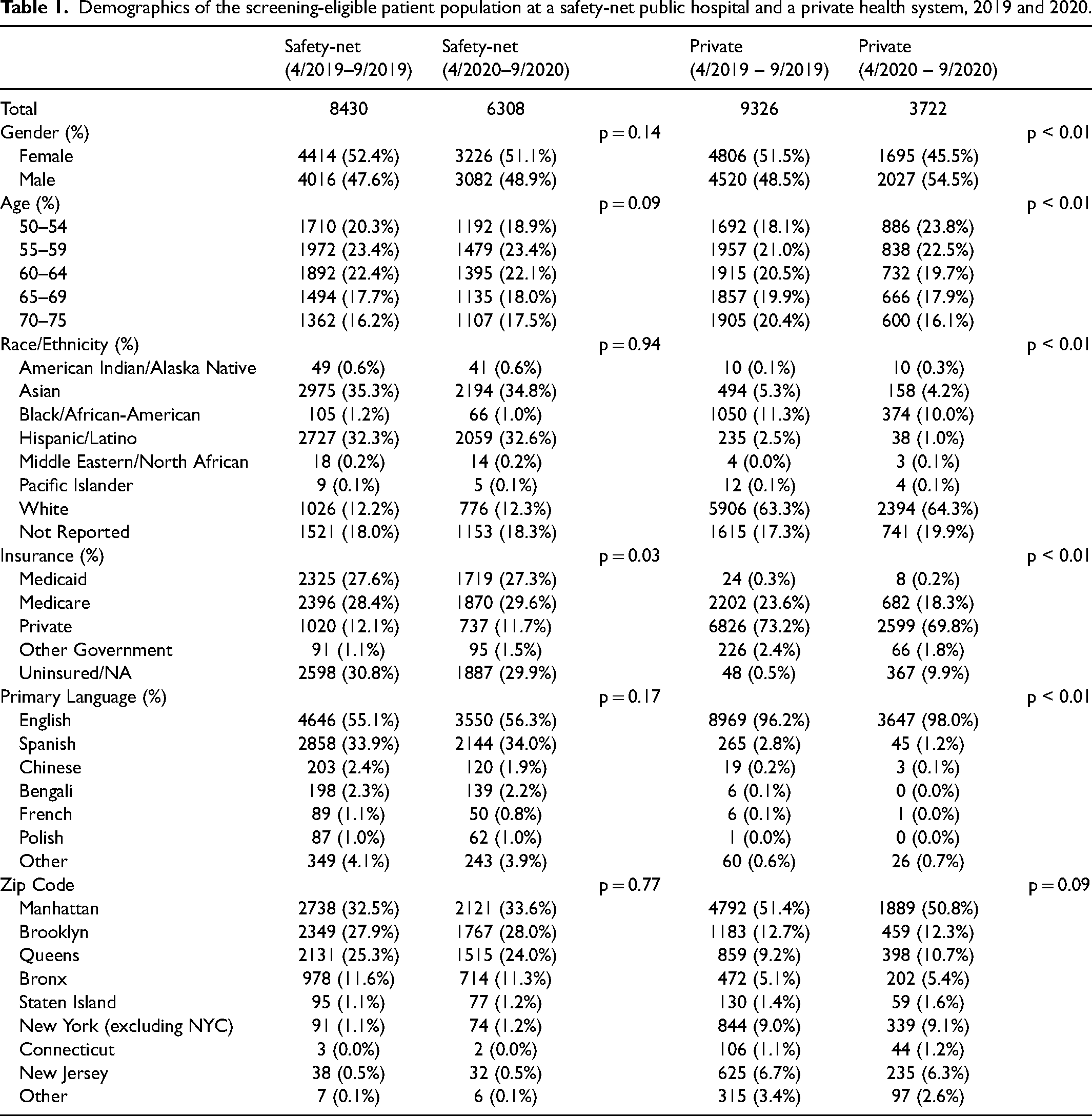
A total of 13,048 patients with outpatient visits were eligible for evaluation in the private health system, with 9326 in 2019 and 3722 in 2020. There were significant differences in multiple demographic categories in the private health system. From 2019 to 2020, the proportion of female patients decreased (51.5% vs 45.5%, −6.0% difference, p < 0.01). In terms of age distribution, the proportion of patients aged 50 to 54 years increased (18.1% vs. 23.8%, + 5.7% difference) while those aged 70 to 75 years decreased (20.4% vs. 16.1%, −4.3% difference, p < 0.01). With respect to race and ethnicity, with the exception of individuals classified as White or unreported, most other groups saw a proportional decrease (p < 0.01). Similarly, with the exception of individuals with no or unreported insurance, all other types of coverage saw a proportional decrease (p < 0.01). From 2019 to 2020, the proportion of individuals whose primary language was English increased (96.2% vs. 98.0%, + 1.8% difference, p < 0.01).
Both health systems had a decrease in outpatient visit volume from 2019 to 2020, with a significantly larger decrease for the private health system (60.0% vs. 25.2% decrease, p < 0.01). At baseline and during the pandemic, the safety-net hospital cared for a greater proportion of individuals who were non-White, were government-insured or uninsured, and primarily spoke a language other than English.
Colorectal cancer screening
In the safety-net hospital during the pandemic, there was a significant decrease in the proportion of patients with an outpatient visit who were screened (6.1% vs. 4.3%, −1.8% difference, p < 0.01, Table 2). There was a significant increase in the proportion of screening by FIT in 2020 (69.6% vs. 88.1%, + 18.5% difference, p < 0.01). There was a corresponding decrease in all other forms of screening, and colonoscopy was the only other modality used during the pandemic. For individuals who had abnormal FIT results, 17.2% in 2019 and 25.0% in 2020 had colonoscopy follow-up within 6 months (p = 0.62, Table 3).
Colorectal cancer screening patterns at a safety-net hospital and a private health system, April to September in 2019 and 2020.
Fecal immunochemical test (FIT) outcomes and follow-up of abnormal results at the safety-net and private health systems, April to September in 2019 and 2020.
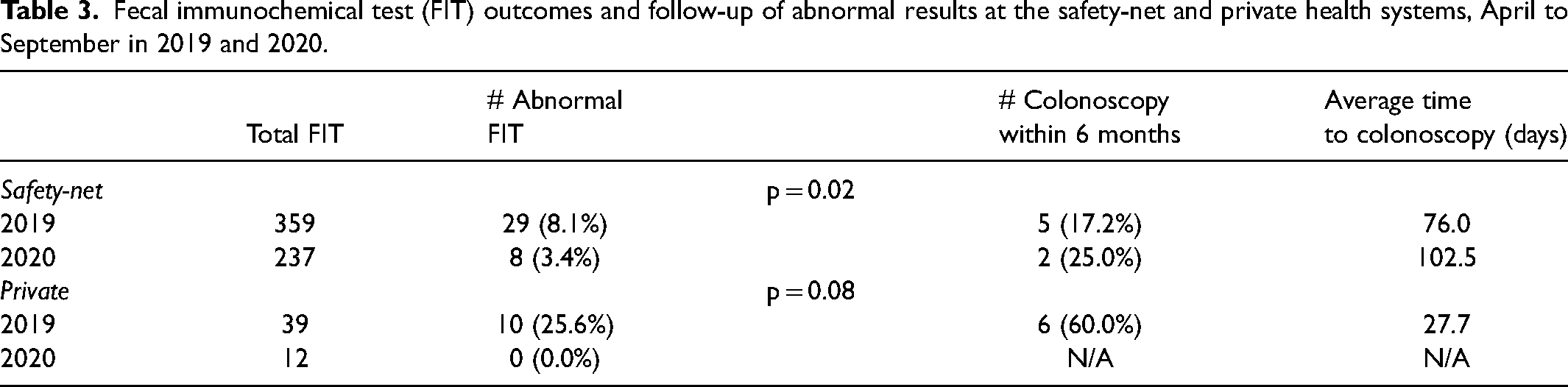
In the private health system, there was no significant difference in proportion of patients screened in 2019 compared with 2020 (0.7% vs. 0.6%, p = 0.48, Table 2). Patients in this system only used FIT and colonoscopy as screening modalities. For individuals who had abnormal FIT results in 2019, 6 patients (60%) had colonoscopy follow-up within 6 months; there were no abnormal FIT results in 2020 (Table 3).
Colorectal cancer diagnosis and treatment
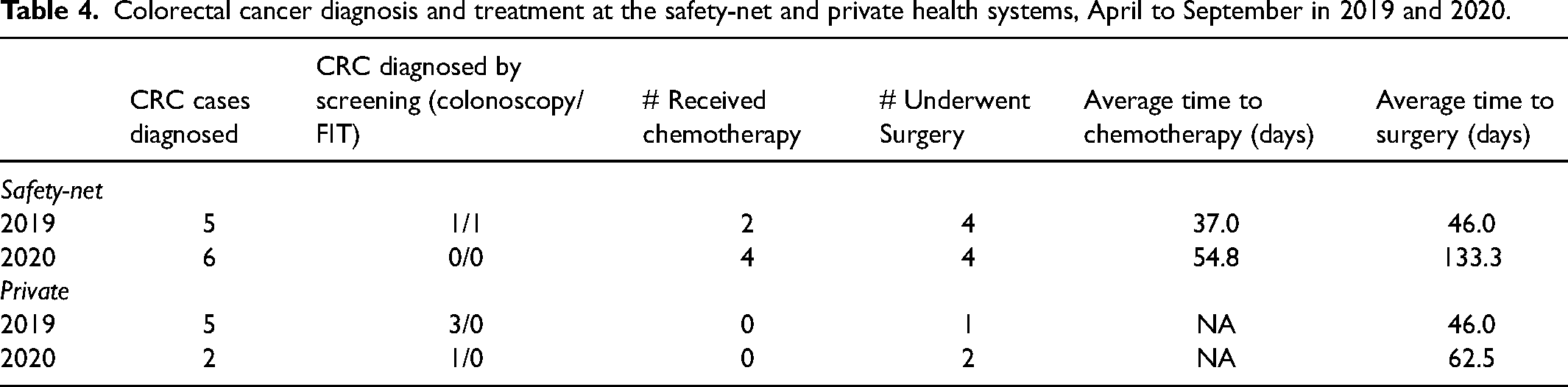
In the safety-net hospital during the 2019 and 2020 periods, screening detected 2 (of 5 total) and 0 (of 6 total) cases of CRC, respectively (Table 4). Similarly, screening in the private health system detected 3 (of 5 total) and 1 (of 2 total) CRC during the same periods. The safety-net hospital had 1 CRC diagnosed by FIT screening. All other screening-detected CRC in both hospital systems were diagnosed by colonoscopy. There were no significant differences in the number of CRC cases diagnosed and no deaths from CRC were observed. Though average time to chemotherapy and surgery were higher in 2020 for both health systems, there were no significant differences between years or hospital system.
Colorectal cancer diagnosis and treatment at the safety-net and private health systems, April to September in 2019 and 2020.
Discussion
The impact of the COVID-19 pandemic on patterns of CRC screening has not been clearly delineated. Overall screening may have declined because of a decrease in primary care visits; however, we aimed to better characterize screening patterns of those with a primary care encounter during the pandemic. Our findings demonstrate that in the public hospital, screening during the pandemic was significantly lower than during the previous year. We observed no change in screening in the private health system, which may be a marker of the difference in resources between the two health systems. However, screening uptake was much lower at baseline in the private health system.
Previous studies have largely focused on the decrease in screening during the peak of the pandemic, with reductions of 70% to 100% compared to the pre-pandemic baseline.9,10,14,15 One study comparing screening from January to September in 2019 and 2020 found a decrease of 53% in FIT completion, though this was in an organized screening program. 16 Another analysis evaluated a full year of screening after the start of the pandemic (March 2020 to March 2021) and found an overall 25% decrease in screening, similar to what was observed for the safety-net hospital in our study (29% decrease). 14 However, our study is unique in accounting for a decreased visit volume and still showing a decrease in screening uptake in the safety-net hospital, suggesting the nature of outpatient visits may also have changed with respect to prioritizing cancer screening and the ability to refer for screening modalities other than FIT. While the screening in the safety-net hospital decreased, the uptake was bolstered by an increase in FIT screening, which as an inexpensive and mailable modality has strong potential value in maintaining or improving screening during periods of decreased outpatient visits. 17
Our findings did not show a change in diagnosis of CRC. In comparison, an Italian study showed 12% fewer CRC cases diagnosed in January to October 2020 compared to the same time period the year prior. 18 Our study did not find significant changes in average time to CRC treatment, but this was difficult to evaluate given the low number of cases diagnosed; however, another single-center study also found no change in numbers of those who received chemotherapy and surgery. 19 We can expect health systems with decreased screening will have fewer CRC diagnoses in the short term, but models evaluating these interruptions in screening predict increased avoidable cancer deaths and later stage at diagnosis in the long term.20,21
We observed decreases in outpatient visits in both health systems, with a significantly larger decrease in the private system. Some studies noted a decrease in outpatient visits during the pandemic, with a reduction of 50% to 70% during the peak of the pandemic, followed by a subsequent rebound in visit volume.13,22 One study in a managed care system compared visit volume in January to October 2019 and 2020 and found a 24% to 43% decrease, similar to what we observed in the safety-net hospital. 23 The larger decrease in visit volume in the private health system could be explained by a higher proportion of both Manhattan (who may have had the means to leave the city during the pandemic) 24 and non-New York City residents who may have pursued care elsewhere compared to the safety-net population.
Our findings highlight the differences in populations between the two health systems, which persisted during the pandemic. At the safety-net hospital, differences in patient population before and during the pandemic were minor. The change in insurance was driven by a slight increase in proportion of Medicare beneficiaries, and a decrease in those with no or unreported insurance, which may signal more people obtaining insurance in response to the pandemic. In comparison, there were many statistically significant differences between patient populations before and during the pandemic at the private health system. The patient population during the pandemic skewed younger, less female, and increasingly uninsured or underinsured. Despite this significant difference, the magnitude of changes was modest and the overall distribution across demographics remained similar. It is possible the patient population in the private health system with more socioeconomic privileges (e.g., older, insured) had the opportunity to leave and obtain care outside of a COVID-19 hotspot. Those without similar privileges may have been confined to the city and obtained medical care as usual, as evidenced by the minor differences in the safety-net population before and during the pandemic.
Our study has several limitations. At the private health system, many patients likely receive care (including screening) at other institutions, which would underestimate the measured screening uptake of this population. On the other hand, the safety-net hospital likely serves a population that receives much of its care at this institution. Additionally, the safety-net hospital transitioned to a new EMR system on April 1, 2019 and the private health system also transitioned to a new EMR system in 2011, with screening records not available prior to these dates. Therefore, a subset of the patient cohort at both institutions may not have been eligible for screening. Excluding these up-to-date patients may lead to a higher screening percentage, particularly at the safety-net hospital. However, we estimate the number of these patients to be relatively low, especially since FIT is the leading screening modality at the safety-net hospital, and patients are more likely to be eligible for annual re-screening during our time period of interest. Lastly, we evaluated screening in the context of primary care outpatient visits. As a result, we may have also missed screening orders placed outside of an encounter (e.g., chart review and phone call) or placed and completed by a specialist (e.g., gynecology, gastroenterology) without seeing a primary care provider. Phone and chart messages without true encounters may be more common in the pandemic era, though televisits were still included in our analysis and most screening remains managed by primary care. Lastly, our findings are specific to two distinct health institutions in New York City, which may not be generalizable to other health systems.
Further research could evaluate overall screening in these institutions and elucidate areas of screening not initiated by primary care doctors. Evaluation of screening in other health systems and regions will also contextualize our results and increase generalizability. Additionally, while models exist that predict more advanced disease and increases in avoidable deaths due to decreased screening, no observational studies exist. With a lens on health equity, there are many proposed solutions for improving screening in underserved populations in the COVID-19 era, such as increasing telehealth accessibility and mailed FIT kits. 25 Along these lines, the uptake of mailed FIT programs should be supported and studied in the setting of mandatory social distancing.
In conclusion, we found that during April to September of 2020 there was an absolute decrease in screening across both a public safety-net hospital and a private health system in New York City when compared to the previous year, with a significant decrease in proportion screened at the safety-net hospital. Our findings add to a body of literature documenting the impact of the COVID-19 pandemic on CRC screening. Our findings are novel in that we determined patient eligibility by outpatient visits to better isolate those obtaining screening by their primary doctor. While we confirm that moments of social upheaval, such as a pandemic, may lead to significant decreases in CRC screening and widen disparities in care, the value and efficacy of non-invasive screening are highlighted and may attenuate these losses.
Footnotes
Author contributions
Data acquisition/preparation (BL, SY, RW, PSL); study design (BL, PSL); data analysis (BL); data interpretation (BL, SY, RW, PSL); writing (BL); critical review and editing (BL, SY, RW, PSL)
COI/financial disclosures
PSL has received research support from Epigenomics and Freenome and is on the advisory board for Guardant Health.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
PSL is supported by grant K08 CA230162 from the National Cancer Institute.
Disclaimer
This material is the result of work supported in part by resources from the Veterans Health Administration. The content is solely the responsibility of the authors and does not represent the views of the U.S. Department of Veterans Affairs or the U.S. government.