
Abstract
Objectives
To examine attitudes towards an annual faecal immunochemical test for haemoglobin (FIT) versus three-yearly colonoscopic surveillance of individuals at intermediate risk of colorectal cancer (CRC).
Setting
A London hospital.
Methods
Five semi-structured discussion groups were conducted with 28 adults (aged 60–74, 61% female) with different levels of CRC risk and experience of colonoscopy or colonoscopic surveillance. Information was presented sequentially using a step-by-step discussion guide. Results were analyzed using thematic analysis.
Results
When evaluating FIT in the context of a surveillance programme, all respondents readily made comparisons with related tests that they had been exposed to previously. Those with no experience of surveillance were enthusiastic about an annual FIT to replace three-yearly colonoscopy, because they felt that the higher testing frequency could improve detection of advanced lesions. Those with experience of colonoscopic surveillance did not perceive FIT to be as accurate as colonoscopy, and therefore either preferred colonoscopy on its own or wanted an annual FIT in addition to three-yearly colonoscopy.
Conclusions
FIT may be well-received as an additional method of surveillance for new patients at intermediate risk of CRC. More research is required to better understand potential barriers associated with FIT surveillance for patients with experience of colonoscopic surveillance.
Introduction
Screening for colorectal cancer (CRC) was introduced into the National Health Service (NHS) Cancer Screening Programmes in England in 2006 to reduce CRC mortality rates by early cancer detection. Individuals aged 60–69 (currently being extended up to age 74) are offered a biennial guaiac faecal occult blood test (gFOBt). About 2% of individuals 1 receive an abnormal gFOBt result and are followed up with an investigative colonoscopy. If the colonoscopy result is negative or defines individuals as at low risk of CRC, individuals are referred back to the Bowel Cancer Screening Programme (BCSP) for biennial gFOBt screening. For the purposes of this paper, these individuals are described as being at ‘average risk’ of developing CRC. Individuals with large (one or more ≥1 cm) or multiple (3 or 4) small adenomas detected at investigative colonoscopy are considered to be at ‘intermediate risk’ of developing CRC, and therefore referred for colonoscopic surveillance at three year intervals. 2 Individuals are considered to be at ‘high risk’ of developing CRC if they have ≥3 adenomas one of which is large (≥1 cm) or if they have ≥5 small adenomas identified at investigative colonoscopy. These individuals would be recommended for colonoscopic surveillance at 12 months and then three-yearly thereafter. 2
The success of any screening or surveillance programme is dependent on the diagnostic performance and acceptability of the test among eligible individuals. Patients have personal preferences for different CRC screening tests 3 and are more likely to complete a test they prefer. 4 A study in the United States found that the most preferred test attributes were non-invasiveness, no pain or preparation and high sensitivity and specificity. 5 Furthermore, a study in the United States looking at the priorities for CRC screening among average risk patients, found that these patients value the potential to prevent cancer over specific test attributes such as avoiding side effects and false positives. 6 There is emerging evidence that risk status may also influence test preferences, with two studies showing that individuals with a family history of CRC prefer tests they perceive to be more ‘accurate’ 7 whereas asymptomatic individuals with no reported family history prefer convenient and non-invasive tests. 8
Attendance for colonoscopic surveillance is around 80% 9 , similar to uptake rates of colonoscopy following an abnormal gFOBt in the BCSP.1,10 Sub-optimal uptake of colonoscopy may in part be attributable to some well-documented patient-reported barriers to colonoscopy, such as the laxative bowel preparation, procedural anxiety and anticipated pain. 11
An alternative to colonoscopic surveillance could be the faecal immunochemical test for haemoglobin (FIT) set to a low threshold for positivity. FIT uses antibodies raised against the globin component of haemoglobin, making it more specific for human blood than the gFOBt. 12 Depending on the threshold for positivity, FIT may be more sensitive than the gFOBt.13–15 Furthermore, a recent systematic review has found that participation rates are higher in screening programmes that use FIT compared with gFOBt 16 , supporting the view that individuals may find FIT more acceptable than gFOBt because it only requires one stool sample and does not involve any dietary restrictions.17,18 Several studies have interspersed colonoscopic surveillance with an ‘interval’ FIT, finding that it may help detect fast-growing adenomas, missed adenomas or cancers earlier than scheduled colonoscopic surveillance.19,20 In the light of these promising results, a large clinical study (‘FIT for Follow-Up’) is in progress. This three-year study will determine the clinical sensitivity and specificity of an annual, single-sample FIT (OC-Sensor by Eiken, Tokyo, Japan) for detecting advanced adenomas or CRC, compared with colonoscopic surveillance at three years in patients at intermediate risk of CRC due to a history of adenomas.
Most research into FIT has focused on clinical efficacy, with limited research on patient acceptability in the context of population screening. One study found that average risk patients who were concerned about procedural discomfort were more likely to choose FIT over colonoscopy as a screening modality, and FIT completion rates were higher than colonoscopy attendance rates 21 , a finding supported in a recent randomized control trial. 22
To our knowledge, there is currently no research examining the acceptability of FIT as a surveillance modality among people at increased risk of CRC. Neither are there any studies describing patient responses to a change in surveillance. However, a study reporting acceptability of predictive genetic testing for familial adenomatous polyposis shows that patients are often reluctant to cease surveillance. People who had been on colonoscopic surveillance expressed a strong desire to continue these examinations (which were universally described as extremely unpleasant), even after they were told that the genetic test had classified them as low risk, ie. surveillance was no longer required. 23 The authors postulated that once people have invested effort in managing their risk, they become reluctant to give up the security of surveillance. There is also evidence that the perceived benefits of colonoscopic surveillance increases with time 24 , and that discomfort diminishes with each round. 25 This suggests that individuals adhering to surveillance guidelines are likely to have had positive experiences with colonoscopy which would potentially make them less enthusiastic about changing to a different surveillance modality.
As part of the ‘FIT for Follow-Up’ study, this qualitative study examined (1) how individuals conceptualize FIT and consolidate their understanding of, and attitudes towards, FIT as an alternative surveillance method, (2) potential barriers to completing FIT, and (3) preferences for an annual, single-sample FIT versus three-yearly colonoscopy as an alternative method of CRC surveillance for individuals at intermediate risk of CRC. We focused particularly on whether previous experience of colonoscopy, or risk of CRC, moderated responses.
Methods
Participants and recruitment
Participant profiles (n = 28).
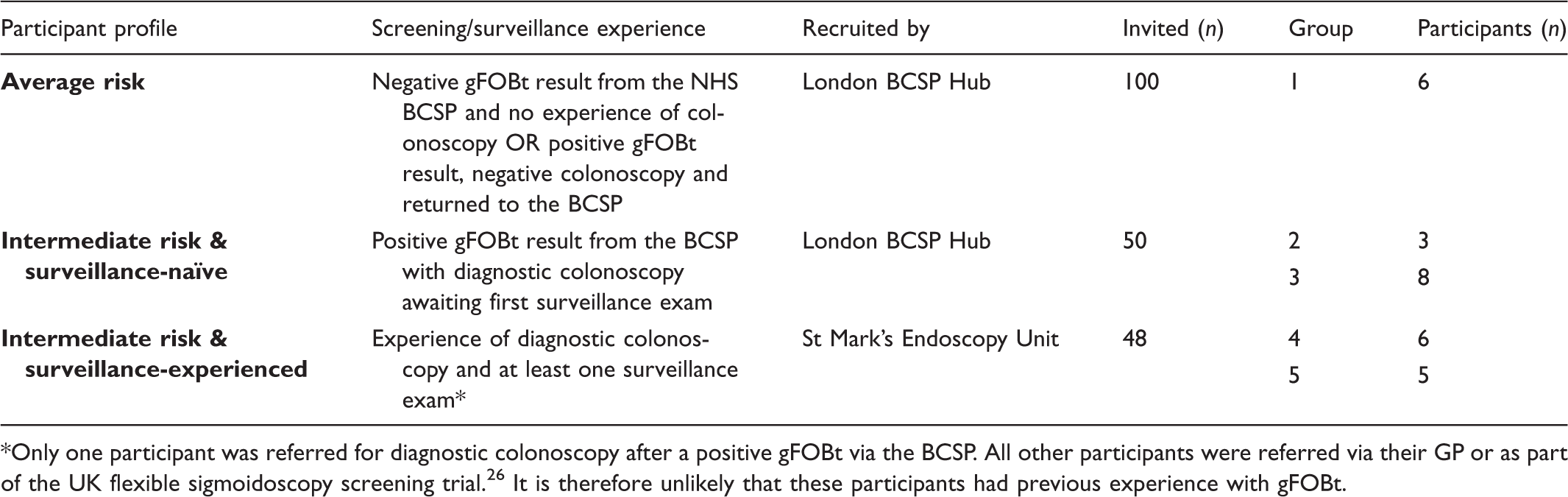
Only one participant was referred for diagnostic colonoscopy after a positive gFOBt via the BCSP. All other participants were referred via their GP or as part of the UK flexible sigmoidoscopy screening trial. 26 It is therefore unlikely that these participants had previous experience with gFOBt.
Materials
The discussion guide included information on the practical issues, results and outcomes, accuracy, and possible risks. This selection was based on previous research on information needs and informed decision-making in CRC screening27,28, and interviews with twelve patients on CRC surveillance who reviewed our discussion guide prior to this study. From these interviews it was apparent that individuals may be concerned about the accuracy of FIT and therefore wanted detailed information about the outcomes of FIT, particularly false-negative and false-positive results. The interviewees also made suggestions about how to present this information simply, e.g. to avoid unnecessary medical terminology.
Procedure
We conducted two discussion groups for each participant profile, to ensure that groups remained relatively small and that our findings for each profile did not reflect the dynamics of a single group. Discussion groups were carried out in November 2011 in a hospital-based teaching room in London, each lasting no more than two hours. The groups were moderated by HB, GV, and CVW, and were semi-structured. Information about the tests was presented in a stepwise fashion using a PowerPoint presentation, with participants invited to ask questions, discuss their reactions, and express their opinions in between each element of the presentation. A copy of the PowerPoint presentation is available on request.
Information preferences
At the beginning of the discussion group, participants were presented with a brief summary of the information that would be covered on four attributes relating to FIT and colonoscopy (practical issues, results and outcomes, accuracy, and possible risks) during the discussion group (see Figure 1). Participants were asked to use an electronic audience response system to select the attribute they believed to be the most and least important to them. Their responses were then presented to them in an electronic bar chart in order to facilitate discussion.
Summary of information to be covered in discussion group.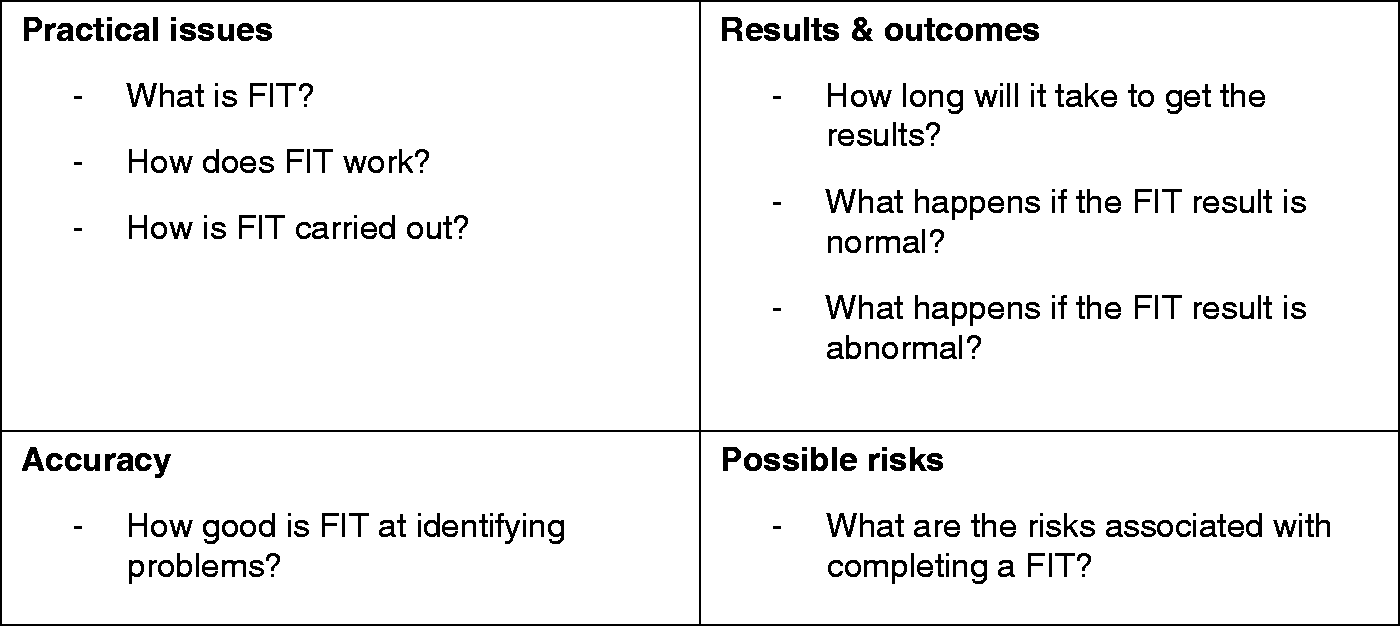
Semi-structured discussion guide
The discussion group was split into four sections, each covering a different test attribute. Information on the practical issues was given first, followed by information on the results and outcomes, test accuracy and lastly, information about possible risks.
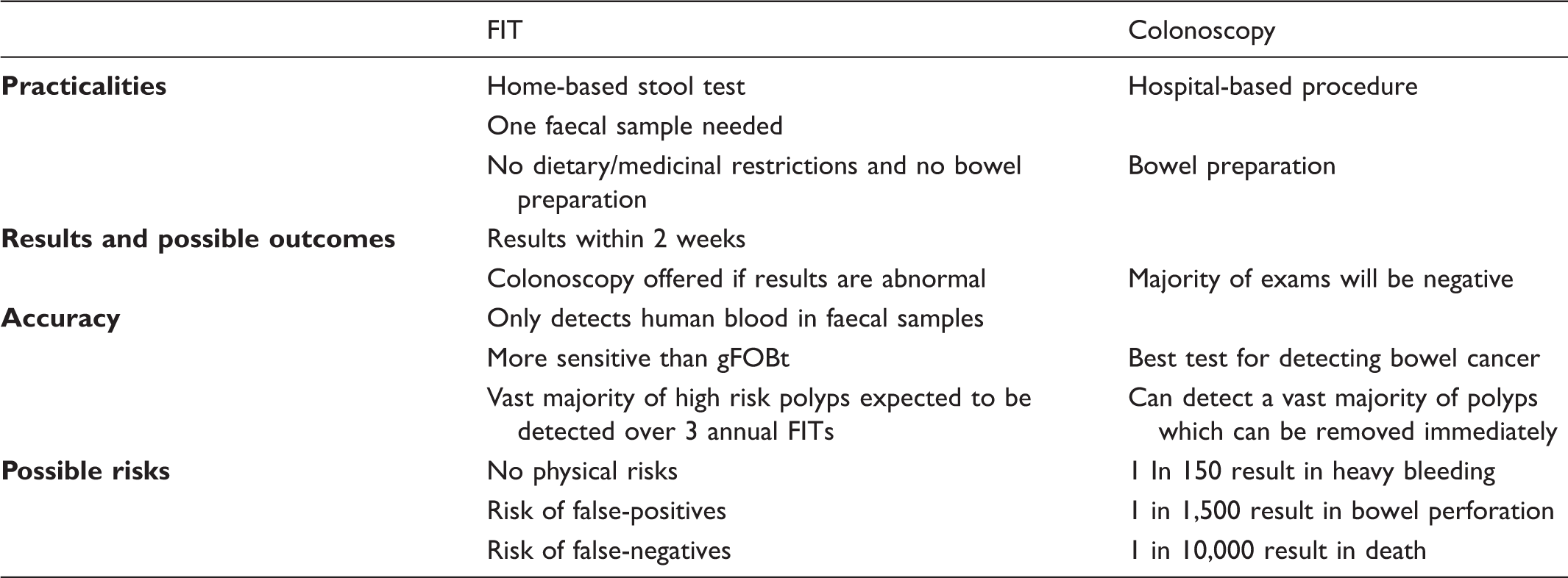
Participants were first introduced to colonoscopic surveillance as it is offered within the NHS, including information on how and why individuals are referred. They were told that a colonoscopy is a hospital-based procedure which involves preparing the bowel using laxatives and that a sedative is offered at the start of the procedure. They were then introduced to FIT, a one-sample home-based stool test that is similar to the gFOBt offered in the BCSP. This information was particularly pertinent for participants in the surveillance-experienced group, most of whom had no prior experience of a gFOBt. An example FIT kit was shown to participants and they were given the opportunity to read instructions on how to complete and return the kit. Participants were informed that a positive FIT result would lead to a colonoscopy referral, but that the majority of colonoscopy results are negative. They were then introduced to the idea of annual FIT surveillance, with referral to colonoscopy if the result is positive, as an alternative to three-yearly colonoscopic surveillance.
Summary of information on test attributes provided.
At the end of each section participants responded to the following question: “Consider the information you have just seen about FIT replacing a routine colonoscopy. How would you feel about the offer of a FIT every year instead of a three-yearly colonoscopy?”. They responded using an electronic response device, selecting an option on a 6-point scale from “very positive” to “very negative” before discussing each section as a group. Once participants had received and discussed information on each attribute, they stated their final overall preference.
Analysis
The group discussions were digitally recorded and transcribed. Transcripts were analyzed by HB using thematic analysis. 30 Once identified, the themes were organized in terms of participant profile and then in the order in which information was provided. Software for qualitative research 31 was used to help manage and interpret the data. Initial themes were identified by HB and discussed and confirmed with GV and CVW.
Results
Sample
Forty-five individuals agreed to participate (a response rate of 23%) and 31 individuals (19 female; 12 male) were recruited to the six discussion groups (see Table 1). Participants were aged 61 to 73 (mean = 66). The data from all participants in group 2 were excluded from the qualitative analysis because two participants did not speak English. Therefore the analyzed sample size was 28.
Information preferences
At the beginning of the discussion, test accuracy was ranked as the most important test attribute (n = 22/28, 78.6%), followed by results and outcomes (n = 6/28, 21.4%). Information about practical issues was ranked as the least important test attribute (n = 14/28, 50%), with most other participants having no preference (n = 13/28, 46.4%).
Practical issues and possible risks
After receiving information on practical issues, participants who had undergone colonoscopy mentioned that it would be easier to complete the FIT than to have another colonoscopy because it would avoid preparation (“Well from my point of view it’d be good not to starve yourself”; female, surveillance-experienced group) and the risks associated with colonoscopy (“It [FIT] takes away that risk of bleeding and perforation… so you know, gotta be a plus”; male, surveillance-naïve group).
Test sensitivity
Even before information on test sensitivity had been given, believing in the ability of the FIT test to detect early signs of CRC was a prerequisite of accepting the proposed change to the surveillance programme (“It [FIT] looks very easy to carry out but there is that element of doubt… is it 100% accurate?”; male, surveillance-experienced group).
After receiving information on practical issues, a main advantage mentioned by participants (regardless of their risk and experience) was that FIT would provide more frequent reassurance about not having CRC (“I would say the fact you’re doing it every 12 months rather than 3 years, should be better shouldn’t it? Because you know you’re getting an update more frequently than you would otherwise”; male, surveillance-experienced group). Many of these participants were concerned about waiting three years between colonoscopies (“Well, having had [some] polyps removed last December, I’ve wondered about waiting three years; and a three-year gap seems like a long time”; female, surveillance-naïve group).
The value of early detection of cancer was further highlighted after information was given on potential results and outcomes, with comments made about the link between early detection and survival (“Hopefully it’d been caught in a short time so you’ve got more of a chance of recovering from it”; female, surveillance-experienced group).
Before being given information on test accuracy, participants at intermediate risk with experience of colonoscopic surveillance suspected that colonoscopy was more sensitive than FIT because it involved a visual inspection of the bowel (“Once you’ve had a colonoscopy you feel very reassured yourself because you’ve actually seen the whole procedure and you know when you come out of there, that there is not anything wrong with you… whereas with this FIT, does it work, does it not… you don’t know”; female, surveillance-experienced group).
When discussing practical issues at the beginning of the discussion group participants were made aware that the FIT regimen being discussed required only a single faecal sample, unlike the three samples required for the gFOBt used in the BCSP. Interestingly, some participants at this point noted that the increased number of samples may favour gFOBt in terms of its ability to detect blood (“I’m very comfortable with the FIT but it also has a downside that it… wouldn’t detect as much as providing three samples, possibly”; female, average risk group). In this respect, all participants expressed concerns about polyps bleeding intermittently which would make them more easily missed by a test that relied on a single faecal sample. This was particularly true if their polyps had not been detected through a gFOBt (“I’ve never had any bleeding or anything like that, just polyps so…it [FIT] wouldn’t show anything, would it”; female, surveillance-experienced group).
Overall, after receiving all of the information on the attributes of both tests the majority of participants at intermediate risk felt that colonoscopy was more accurate than FIT, although in some cases they exaggerated the protective effect of colonoscopy (“I’d be reassured that colonoscopy is 100% accurate and would not miss anything, whereas with the FIT that’s the only choice I’ve got, and if it does miss it I’ve got a good chance of catching bowel cancer”; female, surveillance-experienced group) and did not identify the possibility that FIT may pick up a cancer missed by a prior colonoscopy.
Test specificity
Concerns about the possibility of false-positive results were rarely brought up. When probed more explicitly during discussions on results and outcomes (see Figure 1), participants gave mixed responses (“I would feel a bit unhappy because… that means that the FIT is not accurate”; female, average risk group), versus (“There are risks with everything; I don’t think it’s any different. False-positives, false-negatives, you can’t guarantee anything”; female, intermediate risk, surveillance-naïve group).
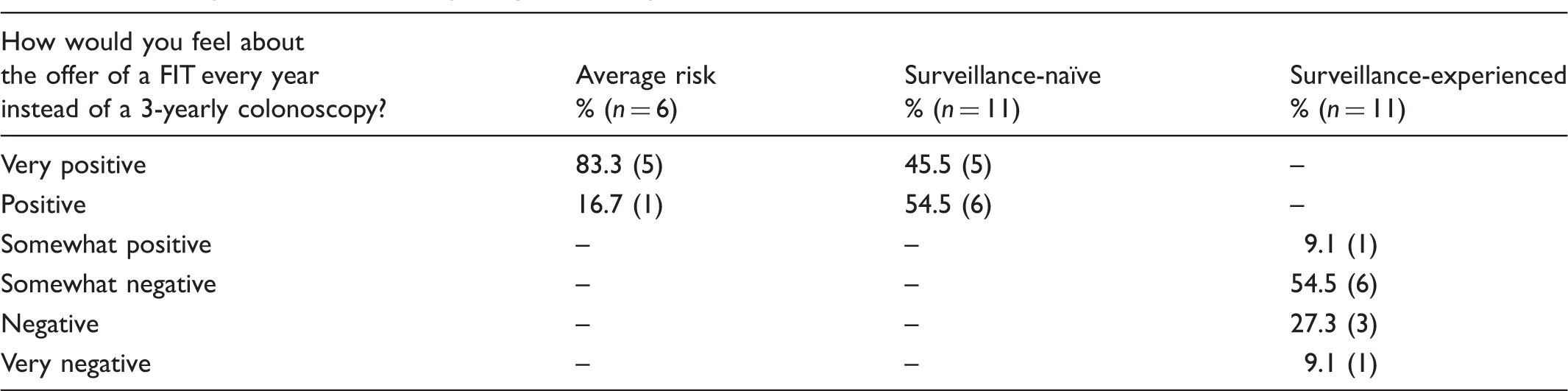
Overall preferences
Overall preference for FIT replacing colonoscopic surveillance.
Discussion
This qualitative study explored patient perceptions of FIT in the context of surveillance following adenoma removal. All participants agreed that FIT was less demanding than colonoscopy.
Previous research on individuals at average risk of CRC found that those who were concerned about procedural discomfort in CRC screening preferred FIT over colonoscopy 21 , however, participants were not provided with information on test frequency. In the current study, participants were provided with information on both procedural discomfort and test frequency. Being tested more frequently, and the impact this can have on early detection during surveillance were the main reasons that participants at average risk chose FIT over colonoscopy overall. This suggests that test frequency influenced overall preferences more than procedural discomfort in average risk and intermediate risk participants without surveillance experience. Concerns about the FIT kit relying on a single stool sample were noteworthy, and seemed to come from previous experience with the gFOBt in the BCSP which uses three separate stool samples.
Experience of colonoscopic surveillance seemed to influence considerations among intermediate risk participants. Those who had yet to undergo colonoscopy as part of the surveillance programme were generally more positive about FIT as a replacement of colonoscopy. Our observation that those with experience of colonoscopic surveillance were more resistant to the idea of FIT surveillance was concordant with the limited amount of literature in this area suggesting a reluctance to relinquish current surveillance practice. 23 It was particularly interesting to note that the main justification for this reluctance chiefly related to participants reporting having had non-bleeding adenomas detected by colonoscopy. This belief may be particularly prevalent among those who come to be on colonoscopic surveillance without ever having experienced home-based stool testing. Future research is required to better understand the reluctance exhibited by the surveillance-experienced group, particularly the extent to which their beliefs reflect inexperience with home-based stool testing, or as suggested by previous research, a reluctance to let go of an existing surveillance regime.
This study had a number of limitations. Recruitment of the discussion groups proved challenging particularly among people at average risk of CRC. Furthermore, in common with other qualitative studies, the sample size was limited, making it difficult to generalize the findings. We did not measure socio-economic status on an individual level, however, the sample was predominantly drawn from London Boroughs (Harrow and Brent). While Harrow is a slightly more affluent Local Authority than the national average (ranking 184th most deprived Local Authority out of 354), Brent is the 35th most deprived Local Authority in England. 32 Both Harrow and Brent are very ethnically diverse with a substantially higher proportion of non-white residents (58% and 64% respectively) than the national average (92%). 33
This study benefited from the step-by-step or ‘drip-feed’ approach used for the discussion guide, which allowed us to gain a better understanding of the specific benefits and weaknesses people attributed to each test. Our use of different patient profiles enabled us to further refine how these perceptions are moderated by individual risk of CRC and experience with other colorectal tests.
The findings have several implications for the design of patient materials and future research. Patient information materials for prospective FIT users need to take account of how perceptions of the FIT may be affected by previous experiences with other types of CRC tests. Patients referred to surveillance via the BCSP may benefit from specific reassurance about how FIT achieves higher rates of clinical sensitivity compared with gFOBt, even though it is based on one rather than three faecal samples.
The potential concerns of patients with previous experience of colonoscopic surveillance may be more challenging to address and therefore the differences we observed between the two intermediate risk groups require further investigation. Specifically, it is important to determine if there are circumstances in which surveillance-experienced individuals would find it acceptable to replace colonoscopic surveillance with FIT. Quantitative research such as conjoint analysis would allow participants to specify the minimum level of sensitivity for FIT (eg. 80%, 90%, or 99%) at which it would become an attractive replacement for colonoscopic surveillance.
Conclusions
This set of discussion groups is the first to consider patients’ views about the use of a FIT as part of surveillance for individuals at intermediate risk of CRC. Previous experience appeared to be an important moderator of patient preference. These results suggest that the introduction of FIT for surveillance is likely to get the best reception from individuals who are new to surveillance, while more research is required to better understand potential barriers associated with FIT surveillance for patients with experience of colonoscopic surveillance.
Footnotes
Funding
This study was funded by a National Institute for Health Research Health Technology Assessment (NIHR HTA) programme grant 09/22/192 and will be published in full in Health Technology Assessment. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the HTA programme, NIHR, NHS or the Department of Health.
Acknowledgements
We thank Lindy Berkman for her comments on the FIT materials, and the London BCSP Hub and St Mark’s Bowel Cancer Screening Centre for their support.