
Abstract
Objectives
To measure whether uptake of breast cancer screening was affected by the publication of the Marmot Review and associated press coverage.
Setting
Eight NHS breast screening centres in the West Midlands of the UK.
Methods
Uptake of breast cancer screening invitations was compared in the week before and after the Marmot review publication. All 12,023 women invited for screening between 23 October 2012 and 5 November 2012 were included. A mixed effects model of the predictors of screening uptake (on date invited, or within 21 days) was created. Predictors considered for inclusion were whether the allocated screening appointment was before or after publication of the review, population factors (age, index of multiple deprivation income domain by quintile, previous attendance), and interaction terms.
Results
Uptake decreased after publication of the review from 65% to 62% (OR = 0.87 95%CI = 0.80–0.94), but a similar decrease was seen for the same dates on the previous year (OR = 0.85 95%CI = 0.78–0.93). Odds of attending screening were lower for women in the most deprived (uptake = 49%, OR = 0.54, 95%CI = 0.46–0.62) in comparison with the least deprived quintile (uptake = 71%). Odds of attendance also increased if the woman had ever previously attended (OR 3.9 95% CI 3.5–4.4), and decreased with each year of increasing age (OR 0.96 95% CI 0.96–0.97). There were no interactions between any of the other predictors and whether the appointment was before or after publication of the Marmot review.
Conclusion
No change in uptake of breast cancer screening above normal seasonal variation was detected after publication of the Marmot review.
INTRODUCTION
There has been much debate in the scientific community about the effectiveness of breast cancer screening, but little communication with the general public on the issue. The recent Marmot review of Breast Cancer Screening 1 received widespread press coverage in the UK.
The Marmot review was commissioned by the Department of Health and Cancer Research UK to examine the balance of benefits and risks. The findings were reported on 30th October 2012. The accompanying press release stated that ‘Breast Screening Programmes in the UK extend lives but at a cost, according to the results of an independent review published in The Lancet today. The Review estimated that while screening prevents about 1,300 breast cancer deaths per year, it can lead to about 4,000 women each year aged 50–70 in the UK having treatment for a condition that would never have troubled them’. There was coverage on the BBC today programme and BBC news, and extensive reporting in the printed press. It was the front page headline in the Guardian, ‘Breast screening, the verdict: it saves lives, but may also harm. Service saves 1,300 women a year. 4000 undergo unnecessary treatment’ 2 and the Daily Mail front page headline ‘Needless cancer therapy for 4000 women. For every life saved by breast screening, 3 patients undergo unnecessary treatment’. 3 It was not the main story but still printed on the front page of the Daily Telegraph with headline Breast screening ‘harming thousands’. 4 The story was reported on page 16 of the Times ‘Keep having scans despite the downsides, women told’ 5 , and page 19 of the Independent Benefits of breast cancer screening ‘just outweigh the risks’. 6 It was not reported at all in the Daily Mirror or the Sun. The results were reported on the NHS Breast Screening Programme website ‘The Review concludes that the NHS Breast Screening Programmes “confer significant benefit and should continue”. Their best estimate is that the Programme prevents 1,300 deaths a year’. 7
Media coverage has previously affected uptake of screening, notably an increase of cervical screening uptake after the death of Jade Goody. 8 Similarly negative media coverage of the MMR vaccine resulted in a reduction in uptake of vaccination. 9 Uptake of screening and immunization is dependent on the characteristics of the people invited, and the effect of press coverage may also differentially affect uptake in different groups. Uptake of MMR was greater with increasing maternal education and employment, with a U shaped association with age. 10 The impact of the negative press coverage over time affected different ethnic groups differentially, with a decrease in vaccination in white children and an increase in Asian children. 9
In the UK, the NHS Breast Screening Programme invites women aged 50 to 70 to undergo breast cancer screening with mammography every three years. Women are allocated an appointment for a particular date and can then either attend that appointment, rearrange for another date, simply not attend, or opt out of being invited again on a temporary or permanent basis. In this research we aimed to measure whether uptake of breast cancer screening changed in the week after the publication of the review findings, in comparison with the week before, and whether this was influenced by the age and socioeconomic status of the women invited.
METHODS
The effect of the publication of the Marmot review on breast screening uptake was determined using a mixed effects model of the factors affecting attendance at screening. Attendance at screening was defined as having screening mammograms taken either on the day the woman was invited, or at another appointment within 21 days. The base model was constructed, and whether the woman was invited for a screening appointment before or after publication of the review was added to that model. Factors considered for inclusion as fixed effects in the base model were the woman's age in years, a proxy for the woman's socioeconomic status (the quintile of the income domain of index of multiple deprivation (IMD) derived from her home postcode), and whether the woman had previously attended breast screening. The centre the woman was invited to attend was added as a random effect. Whether the appointment was before or after the review was added to the model, followed by its interaction with the woman's age, socioeconomic status, and previous attendance. Factors which had significantly non-zero coefficients at the 10% level (Wald test) were retained in the model. Second order penalized quasi likelihood analysis was used in MLwiN version 2.26. 11 This analysis was repeated for the same two week period in the previous year, to determine whether any seasonal variation can be expected at this time of year.
Sample size calculations indicated that to be able to detect a 5% change in uptake at eight centres with intracluster correlation coefficient 0.05 (at 5% level with 90% power) would require 2,500 women in each group, equivalent to 3 days of screening in the West Midlands both before and after the findings were released. To eliminate effects of days of the week, data for a full week before and after the publication of findings were included. The before measurements were from women invited to screening on Tuesday 23 to Monday 29 October inclusive. These were compared with measurements from women invited to screening on Tuesday 30 October (the date of publication) through to Monday 5 November inclusive (after).
All women invited for breast screening in the West Midlands of England in the time period are included in the analysis. The West Midlands has a mix of urban and rural areas, and a range from very deprived to very affluent areas. Data were extracted from the National Breast Screening Service database.
Approvals were granted by the Biomedical Research Ethics Committee at the University of Warwick reference 254-11-2012.
RESULTS
Characteristics of women invited for breast screening in the West Midlands of England in the week before and the week after the publication of the Marmot review of Breast Cancer Screening
*significantly different before and after the review at the 5% level
Of 12,023 women invited to attend screening, 6454 (54%) attended their allocated appointment and 1162 (10%) attended another appointment within 21 days. Uptake for women in the most deprived quintile according to IMD deprivation score was 49% in comparison with 71% in the least deprived quintile. Uptake by characteristics of women invited is described in table 2. Uptake was 65% in the week before the publication of the Marmot review and 62% in the week after. Uptake in the week before and after the review is shown in figure 1, alongside uptake over a longer time period and the previous year for the purpose of comparison. Rates of opting out of screening were similar at 5.3% before the publication of the Marmot review and 5.0% afterwards (table 2).
Uptake of breast screening for the 20 weeks before and after the Marmot review, with comparator data from the previous year (dashed line). Vertical red line denotes date of review publicity. Uptake is on original appointment date or within 21 days. Error bars are 95% confidence intervals Attendance by the characteristics of women invited for screening and whether their appointment was scheduled before or after Marmot review coverage *The ‘other’ category includes 177 women who could not attend due to being under care, 128 women who were ineligible because they were recently screened, 21 women who attended but were not screened, 20 women who had moved away, 6 women who had died, 4 women who had opted for a private screening appointment, and 3 women for whom their attendance status was unknown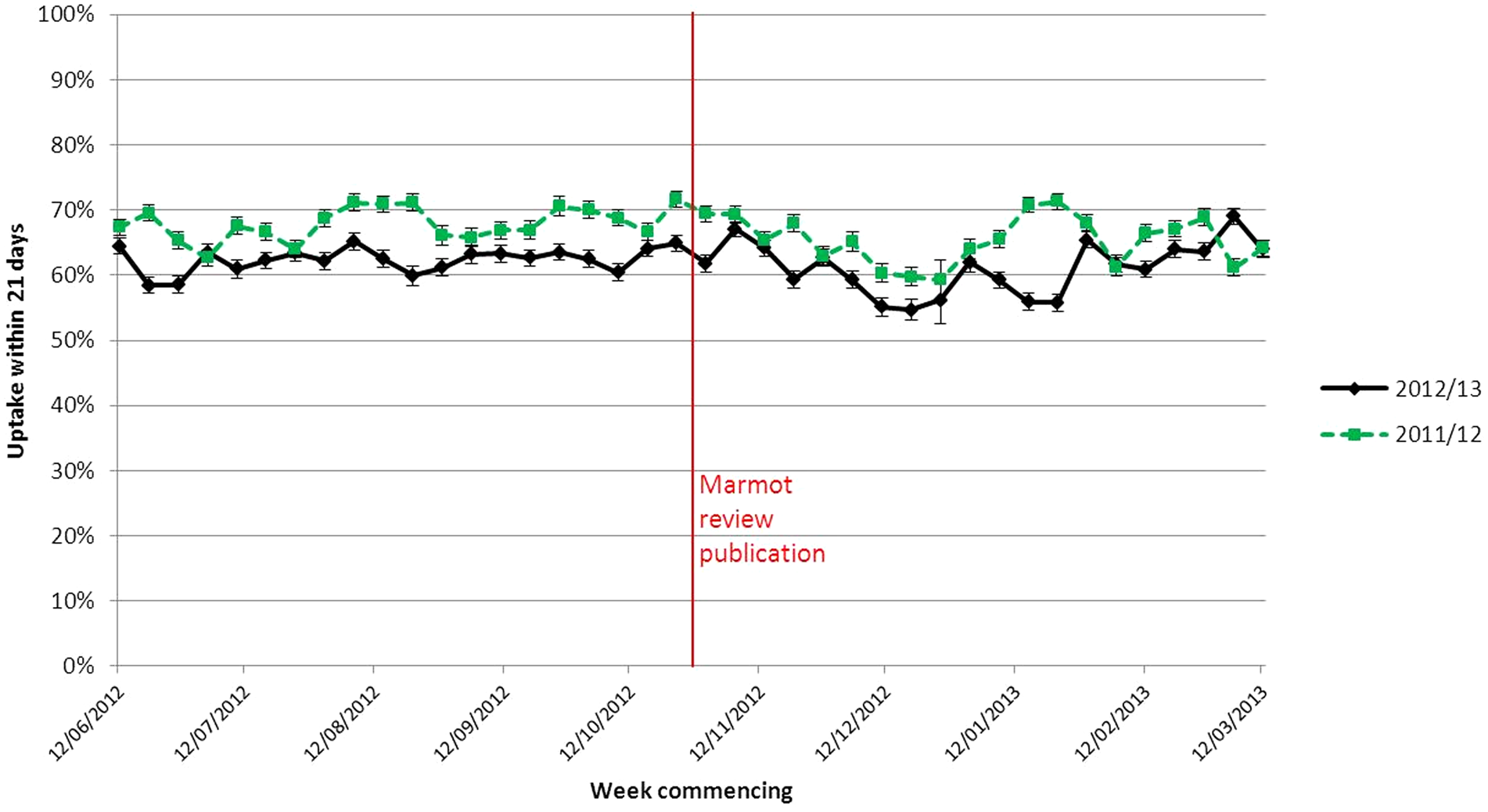
Final model of attendance at breast screening. Women who attended on or within 21 days of their appointment date were defined as attended, all other women were included and defined as not attending. Reference category for IMD is quintile 1 (least deprived), age is centred by mean. Centre was included as a random effect (variance = 0.022, st err = 0.013, χ2 = 2.9, p = 0.09)
As the 21 day cut-off may have introduced some contamination (women with an original appointment date before publication of the review may have been deterred from attending a rearranged appointment once the review was published, or alternatively women rebooking appointments after 21 days may have been excluded), we undertook a sensitivity analysis to model the effect of different definitions of uptake. Changing the definition to attendance at the original booked appointment only decreased the effect size to below the threshold for statistical significance (1.7% decrease in uptake, OR after publication = 0.93 95% CI = 0.86–1.00). Likewise, changing the definition to identify everyone who rebooked their appointment after 21 days as attending also decreased the effect size to below the threshold for statistical significance (OR after publication = 0.96 95% CI = 0.88–1.05).
DISCUSSION
Uptake of breast screening decreased slightly in the week after publication of the results of the Marmot review of breast screening, but this effect was also present for the same two weeks in the previous year, indicating that it is likely to be due to seasonal effects such as declining attendance in the weeks before Christmas. Attendance within 21 days of the original appointment decreased from 65% to 62% (OR = 0.87 95%CI = 0.80–0.94). No interaction was found between this change and the women's age, previous attendance at screening, or a proxy for her socioeconomic status.
In this study we analyzed uptake rates across eight centres over a two week period, and so had sufficient power to detect small changes. Data collection was four weeks after publication of the Marmot review, enabling analysis of effects on uptake in a short time period. However, this meant that if a woman rearranged her appointment more than three weeks after the original date, data were not available about whether she attended.
Sensitivity analysis using different definitions of attendance indicated that any decrease in uptake might be due to women rearranging, rather than never attending their appointment. There was a slight imbalance in the socioeconomic status of women invited for screening before and after review publication, (before the review 26.5% of women invited were in the second least deprived quintile in comparison with 24% after). This was corrected to some extent by inclusion as a predictor in the model, but there may still be a slight underestimation of effect size as a result. We would expect any effect on uptake as a result of the press coverage to manifest within a few days, as that is when women would be most aware of it in their decision making, and therefore this study is designed to investigate effects across several centres over a short time period. The Marmot review may have longer term impacts contributing to shifts in opinion over time, which merits further quantitative and qualitative research. This study is not a randomized controlled trial, so is subject to unknown confounders, and therefore we cannot infer that any change in uptake was as a result of the publication of review findings.
No previous studies were found assessing the impact of publicity on breast screening attendance, but response to negative publicity about the MMR vaccine was dependent on ethnicity. 9 In this study we included important covariates of age, socioeconomic status, and previous attendance at screening in the model. However, little ethnicity data is recorded in the Breast Screening Programme, so it was not possible to include the effect of ethnicity on uptake. We found no evidence that the publication of the review affected any group of women disproportionately (by age, socioeconomic status, or previous attendance), however, we do not know whether it differed by ethnic group.
The extensive media coverage of the Marmot review findings, which included potential harms of breast cancer screening, does not appear to have affected uptake or the number of women choosing to opt out of screening altogether. The reason for this is unclear. The media coverage was extensive, and so it would be unreasonable to conclude that there was negligible exposure. It is possible that among women who attend breast screening it is popular and valued, and therefore negative press coverage would not affect their decision to attend. This is variously argued to be either due to the programme's success and effectiveness, or due to overdiagnosis and the popularity paradox. There are a myriad of other possible reasons for this study finding no change in uptake beyond normal seasonal variation. We do not know what proportion of the women invited to screening were exposed to the media coverage, whether they were exposed to the negative or positive elements, how they interpreted them, or the level of trust they had in the sources. We did not investigate why there was no impact of the press coverage; this is beyond the scope of this paper, but merits further research.
More extensive work is required in the field to understand the reasons for overall differentials in uptake and on the relationships between press coverage and uptake, in particular women's understanding of the potential benefits and harms of breast cancer screening, and how this understanding is influenced by the popular media, the breast screening leaflet, and communication with health professionals and society. One of the main drivers of uptake is a woman's socioeconomic status, and so the potential differential effects by socioeconomic status and ethnicity should be included in such analyses.
CONCLUSIONS
We detected a small decrease in uptake for breast screening appointments scheduled in the week after publication of the Marmot review of breast screening (∼3%), but this decrease was also present for the same dates in the previous year, so is likely to be due to confounders or seasonal effects. We found no evidence for differential effects by age or socioeconomic status.
Footnotes
ACKNOWLEDGEMENTS
This report is independent research arising from a postdoctoral fellowship supported by the National Institute for Health Research. The views expressed in this publication are those of the authors and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health.