
Abstract
Objectives
To assess women's perception of pain and acceptability of low vaginal swab (LVS) and anorectal swab (ARS) for antenatal screening for Group B Streptococcus (GBS), and to compare the detection rate between these tests.
Methods
Separate LVS and ARS were collected at the 36-week antenatal visit, either by the patient herself or by her clinician. Acceptability and pain were evaluated on a Likert scale using a standardised questionnaire.
Results
A total of 278 women were recruited, with a median gestation of 36.3 weeks (IQR 36–37). Of these women, 96% undertook specimen self-collection. The overall prevalence of colonisation was 64/278 (23%); 52 women had positive LVS results (18.7%), and an additional 12 (5.5%; 95% CI 2.5–8.5) were negative on LVS but positive on ARS. Most women rated LVS (99%) and ARS (92%) to be either ‘pain-free’ or causing ‘mild discomfort’, and found the LVS (90%) and ARS (84%) to be either ‘totally acceptable’ or ‘somewhat acceptable’.
Conclusions
The addition of an ARS resulted in an enhanced GBS positive rate, and most women found the test acceptable.
INTRODUCTION
Antenatal screening for Group B Streptococcus (GBS) is performed using both low vaginal swab (LVS) and anorectal swab (ARS), as there is a large body of evidence that demonstrates an improved detection rate with the addition of ARS compared with LVS alone. 1–5 However, some women do not like performing anorectal swabbing, which has been reported to be painful, 6 and this may adversely affect the uptake of a screening programme. To assess these aspects of the GBS screening recommendation, we undertook a prospective study to: (1) determine the pain and acceptability of LVS versus ARS; and (2) compare the GBS positive rate from LVS alone with that from LVS and ARS.
METHODS
Between August and November 2008, all women seen for their 36-week antenatal visit and booked for vaginal delivery at a large regional Australian teaching hospital were asked to participate in what was standard of care at this institution. In accordance with standard practice in the unit, education on the collection of screening swabs using both verbal and written instructions was given to antenatal women. If women felt uncomfortable with self-sampling, they were given the option of having the swabs performed by a maternity care provider (doctor or midwife).
Demographic data collected included age, gravidity, parity, ethnicity and smoking status. Women choosing to perform their own swabs were directed to a private room at the antenatal clinic to perform the swabs. They were asked to insert a sterile, single cotton tipped microbial swab (Amies Agar Gel M40, Copan, Italy) 2 cm into the vagina and a second, separate swab, 1 cm into the anus. Immediately after collection of the swabs, women were asked by a staff member at the antenatal clinic to grade the physical pain and acceptability of each test on a 5-point Likert scale, ranging from ‘pain-free’ to ‘unbearable’, and ‘totally acceptable’ to ‘not at all acceptable’.
A previous study has indicated that 73% of women reported some level of pain from the ARS. 6 To show a 20% difference in the number of women reporting pain with the ARS versus the LVS, with a power of 80%, and a type 1 error rate of 5% (2-tailed), a sample size of 100 is required.
Data were collated and statistical analyses undertaken using SPSS version 18 (SPSS Inc, Chicago Ill). The concordance of the LVS versus ARS results was assessed using McNemar's test and Kappa co-efficient. A P-value of <0.05 was considered statistically significant.
RESULTS
ARS versus LVS result in women who had both LVS and ARS performed
Of the swabs performed, 266/278 (95.7%) LVS and 258/268 (96.3%) ARS were self-collected by study subjects. Whether the swab was self-collected or collected by the clinician made no statistically significant difference in the positivity rate for the LVS (P = 0.09) or the ARS (P = 0.99).
There is a strong concordance between a positive LVS and ARS (Kappa 0.77; P < 0.001), with no directional bias among those with discordant results (McNemar's test P = 0.36). Fifty-two women had positive LVS (18.7%), and an additional 12 (5.5%; 95% confidence interval 2.5–8.5) were negative on LVS but positive on ARS. Using a positive result in either the LVS or ARS to indicate colonisation, the overall prevalence of GBS colonisation in this population was 64/278 (23.0%).
Of the 201 women who found the LVS to be ‘pain-free’, 42% (84/201) reported some level of pain with the ARS, whereas of the 123 women who reported the ARS as ‘pain-free’, only 4.9% (6/123) reported some level of pain with the LVS (Kappa 0.34, McNemar test P < 0.0001). Most women did not report a high level of pain with sample collection, with 270/274 (99%) and 242/263 (92%) of women rating the LVS and ARS, respectively, to be either ‘pain-free’ or causing ‘mild discomfort’ (Figure 1).
Pain scores (1 = pain-free, 2 = minor discomfort, 3 = moderate pain, 4 = very painful, 5 = unbearable) and acceptability scores (1 = totally acceptable, 2 = somewhat acceptable, 3 = acceptable, 4 = not acceptable, 5 = not at all acceptable)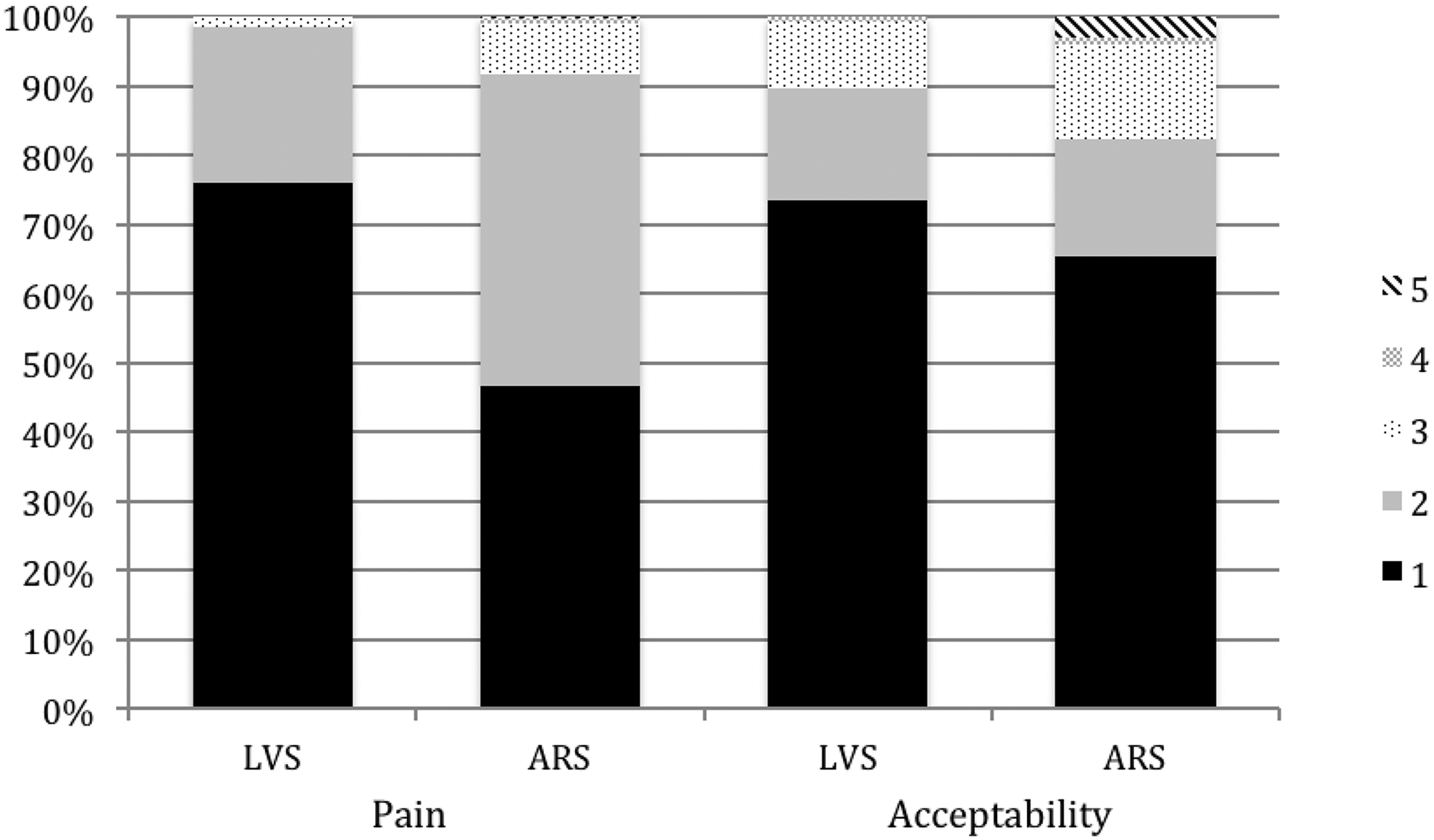
The majority of women found the LVS (244/272, 90%) and ARS (219/261, 84%) to be either ‘totally acceptable’ or ‘somewhat acceptable’. Of the 86 women who did not find the ARS ‘totally acceptable’, 23 (27%) found the LVS ‘totally acceptable’. The 174 women who reported the ARS to be ‘totally acceptable’ also reported the same acceptability for the LVS. Whilst there is a strong concordance between the acceptability of the LVS and ARS (Kappa 0.79), women were more likely to find the ARS not ‘totally acceptable’ (McNemar test P < 0.001).
DISCUSSION
For antenatal GBS screening, the use of combined LVS and ARS is recommended and supported by previous studies, 1–5,7 and our study has demonstrated that the addition of ARS results in an increase in the positivity rate from 18.7% to 23.0% compared with the use of LVS alone. The reason to swab both the vagina and the anorectum is that GBS may colonise either or both of these areas. 5,8 If the women in our study were screened using LVS alone, 12/278 (4.3%) of the study population would have been erroneously categorised as ‘GBS negative’, and denied chemoprophylaxis in labour. The maternal GBS colonisation of 23.0% in our study population is consistent with the 24% colonisation rate previously reported in Australian women. 9
The addition of ARS does not increase screening costs, because only a single combined swab, sampling both the lower vagina and the anorectum, is laboratory tested. 10 In spite of this, the acceptability of the ARS to women is often seen as a barrier to its use in GBS screening. In work where swabs were clinician-sampled, anorectal swabbing has reportedly caused ‘mild to moderate pain’ for 68% of women, and 5% reported ‘severe pain’. 6 These results are in contrast to our self-sampled population, where the majority of women described minimal pain and found the procedure quite acceptable. GBS self-sampling has been previously validated 11–13 and is included within the guidelines from most authorities. 10,14 A randomized study where subjects had both self-collected and clinician-collected rectovaginal swabs performed found a GBS positive rate of 18.8% (62/330) in clinician-obtained specimens and 17% (56/330) in self-obtained specimens, with a strong correlation between the two sampling methods. 13 Evidence supports self-sampling, with 58–83.6% of women preferring this collection method 12,13 and 90% not finding the procedure difficult. 12 Results from our study concur with these findings.
There are limitations to our study. We are unable to show whether the additional 12 cases (5.5%) of GBS colonisation detected by the ARS is clinically significant, as this would require a much larger longitudinal study looking at neonatal outcomes. It has been estimated that at least 24,000 women need to be screened in order to prevent one neonatal death from early-onset GBS sepsis. 15 Therefore, in order to show a 5% difference in neonatal mortality from a screening programme using LVS versus another using combined LVS/ARS, a study with a sample size of over one million women would be required, for a power of 80%.
CONCLUSIONS
Most women found the ARS to be at least ‘somewhat acceptable’, causing at most ‘minor discomfort’. Given that GBS screening using combined LVS/ARS would result in an additional 5.5% of colonised women being detected, and considering the serious morbidity and mortality associated with early onset GBS neonatal sepsis, a pragmatic approach to antenatal GBS screening may be to recommend the use of a combined LVS/ARS for all women, but to give the minority of women who find the ARS unacceptable the option of screening using LVS alone.
Trial identification: ACTRN12611000863932