
Abstract
Objectives
To investigate the impact on women, and their healthcare providers, of initial-reactive HIV test results which required re-testing in the New Zealand antenatal HIV screening programme.
Methods
Women with initial-reactive HIV test results from 2007 to 2011 were identified through the antenatal HIV screening programme. Semi-structured telephone interviews were undertaken with seven women and 30 healthcare providers. Responses to questions were written verbatim. Three researchers undertook preliminary coding of the interviews and identified common themes which were applied to the transcripts and key excerpts obtained.
Results
All of the women interviewed experienced considerable anxiety upon receiving the result, but the extent of this anxiety was rarely appreciated by their healthcare provider. Their main worries were for their own health, that of their children and family, and their relationship with a spouse or partner. Despite this stressful experience, support for the screening programme was strong. Adequate information and timely receipt of results were identified as vital. Healthcare providers also supported the programme but stressed that clear, timely and personal communication with laboratory personnel was important.
Conclusions
The ideal way to alleviate anxiety in women from re-testing is to limit the need for this by obtaining as much information as possible from the original sample. If re-testing is necessary, healthcare providers need to appreciate the anxiety that will arise, ensure that they have the best possible information and communicate this to the women, as soon as is practicable, in an easily understood manner.
INTRODUCTION
The risk of mother-to-child transmission of HIV can be markedly reduced through the use of antiretroviral treatment, avoidance of breast feeding and careful obstetric management. 1,2 This reduction can only be achieved when the woman is known to be HIV-positive either before or during her pregnancy. This has prompted governments and healthcare agencies around the world to encourage routine antenatal HIV screening.
Since 2006, the New Zealand Ministry of Health has progressively implemented a programme in which all pregnant women are offered HIV screening as part of standard antenatal care. Women whose initial enzyme immune-assay (EIA) test result is over the cut-off for a definitively negative result are required to provide a second blood sample, that is sent for viral load testing – which needs to be undertaken on anticoagulated blood – to exclude or confirm HIV infection. 3 This algorithm was developed by the National Screening Unit (NSU) and differs from that practiced for HIV diagnostic testing in New Zealand (sending the EIA test for a Western Blot confirmatory test). The main reason for this was to allow for the receipt of definitive results within a maximum of one month from the initial blood test, even with early infection, compared with up to six months for a conclusive result with a Western Blot test result. Even though the initial EIA tests now used are highly specific, as the prevalence of undiagnosed HIV is very low – prior to the screening programme this was estimated to be around one per 5000 4 – it was appreciated that there could be many more initially reactive tests among uninfected than infected pregnant women. As adverse experiences of re-testing could have an impact on the overall balance of harms and benefits of the screening programme, and the uptake of HIV screening, it was considered important to monitor the experiences of women being re-tested, and of the health professionals caring for these women.
Although antenatal screening for HIV has been in place in other countries for many years, and surveys and interviews have been used extensively to ascertain attitudes of pregnant women and providers to HIV screening, 5,6 no published studies have specifically investigated the effect on women, or among their healthcare providers, of receiving an initial-reactive result and requiring re-testing. The aim of this report is to investigate the experiences of women who had an initial-reactive test which was then confirmed as negative on re-testing, and the experiences of their healthcare providers.
METHODS
The staged introduction of the antenatal HIV screening programme in New Zealand began in 2006. Antenatal HIV coordinators in each district where the programme was operating informed the AIDS Epidemiology Group (AEG) of the name of the healthcare provider for all women who had an initial screening test that was reactive and could not definitively rule out HIV infection (referred to in this paper as an initial-reactive result). Healthcare providers were invited to participate in a short telephone interview. Those who responded and completed the interview were asked to send a letter of invitation to participate to the woman concerned. If the woman replied and agreed to the interview, her name and contact details were released to the AEG and a telephone interview was conducted between January 2007 and December 2011.
A qualitative research approach allowed the researchers to focus on the experiences and feelings of participants. Semistructured interviews were used to enable the interviewer to pursue unique lines of questioning, and to explore differences in the experiences of participants. 7 Each interview lasted approximately 10 minutes. This short time was deemed appropriate to fit in with the schedules of women and the healthcare providers.
Thirty healthcare providers (19 General practitioners and 11 midwives) and seven women agreed to be interviewed, representing a participation rate, among those contacted, of 34% (30/88) and 28% (7/25) respectively (Figure 1). Women who had a true positive HIV test result were excluded. The average age of six women was 31 (range 29–34). Five women were of European ethnicity and one Asian. For one woman the age and ethnicity was not known. The demographic characteristics of women who did not agree to be interviewed were not known. Interview content was written verbatim by the researcher (SM). To protect the privacy of the women, in this report, pseudonyms are used.
Flow chart of follow up of initial-reactive results and interviews done with healthcare providers and women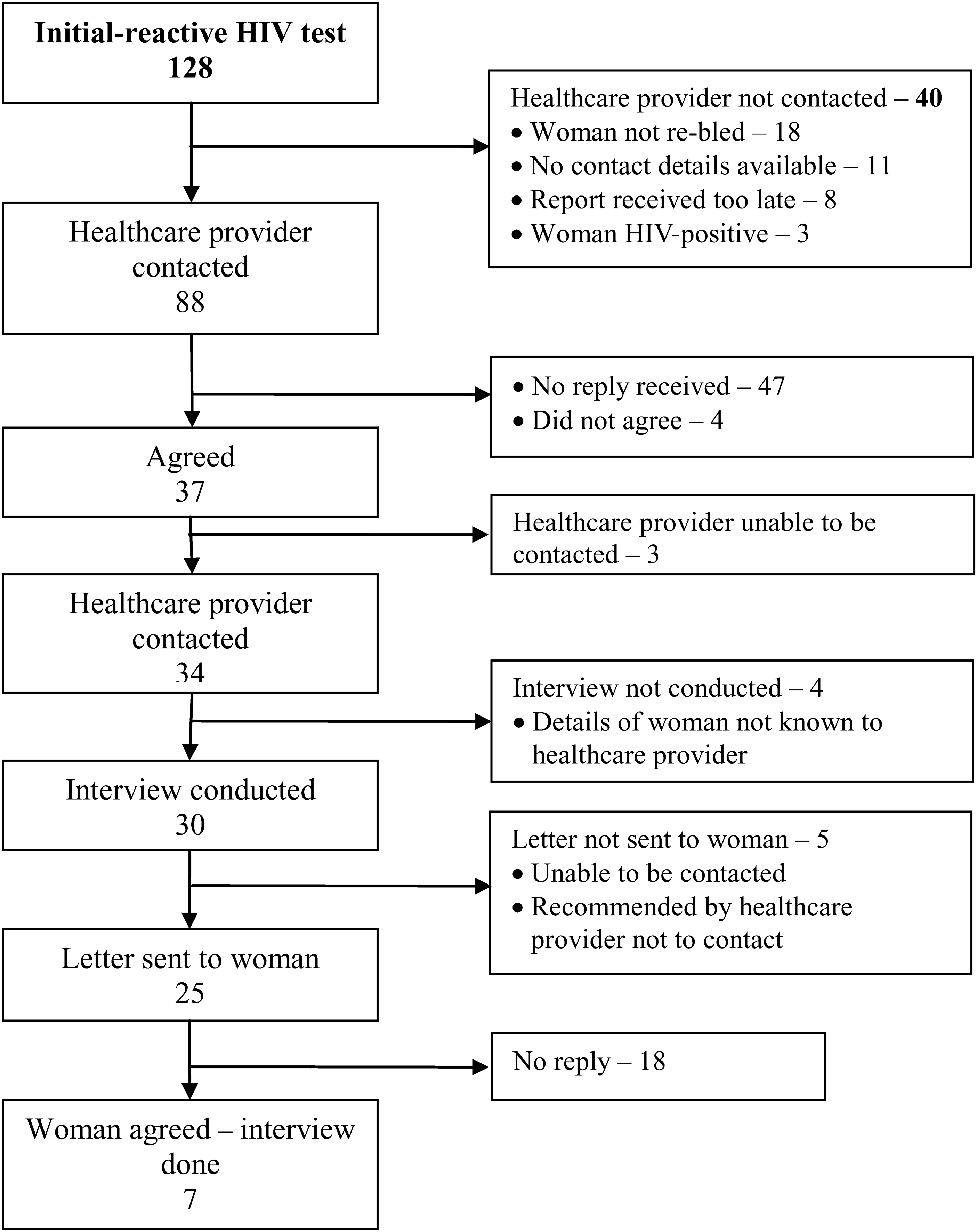
Three researchers (SM, SL and ND) undertook an iterative process of thematic analysis of the study data. 8 Multiple coding was followed by the cross-checking of coding strategies and agreement of a coding scheme. The primary coder (SM) applied the final coding scheme to the interview transcripts, re-read coded sections to extract themes and identified key excerpts from the interviews.
Ethical approval for the study was granted by the New Zealand Ministry of Health Multi-region Ethics Committee in December 2006 (MEC/06/10/129).
RESULTS
Interviews with the women
Initial reaction
Receiving an initial-reactive HIV test result had a considerable impact on all the women interviewed, with many reporting this in quite extreme terms: It was awful! Not something you expect. (Hailey) I was mortified – as though I had done something wrong. It shocked me. (Michelle) All sorts of things cross your mind – as a baby I had a blood transfusion and was that the reason. (Lisa) I've been with my husband for 10 years. As we were driving home after seeing the midwife we were both asking each other if there was anything that we had to tell each other. (Makayla) I even started thinking does my husband think I've had an affair. (Rachael) … I had a miscarriage – I don't know if all the stress etc – whether that causes a miscarriage or not. (Hailey) I don't suffer miscarriages easily but something like this could push you over. I stopped eating and sleeping – it was terrible – pretty crap. (Rachael) I've got two other children and I kept thinking what if I had it [HIV] and hadn't been tested in the other pregnancies and had passed it on to my children. I think every mother would feel like that. (Lisa) I was still pretty cut up about it and thinking I've shortened my life span and my partner's life. (Carly)
Contact with healthcare provider
It was important to all the women that the confirmatory tests were undertaken quickly and that they received the results clearly and without undue delay. Support from the healthcare provider was important and, for several women, the healthcare provider's knowledge of the process helped to allay their anxiety: My midwife was great though in explaining everything and her support was really good. (Makayla) I think the main thing is trying to understand why I had the false positive – what are the explanations for that … . (Lisa) When the specialist told me the final result I was quite angry. I wanted to know why the false result came up and he kind of just said its negative and that's it. I was real pissed off. (Carly) Looking back on it now I would have liked to know more information about what happens to the blood – where does it go, how is it tested and what are the chances of getting these false tests. (Michelle) I expected to get the result within a couple of days and I kept phoning the nurse and it hadn't come, hadn't come, so that was even more stressful … it was eight days later that I finally got the result. (Hailey) They reassured me that this [result of the second test] was OK but I am still worried about it. (Tara) It's cool that I don't have it, but it's hard being told that you do and then you don't.
Interviews with healthcare providers
Several of the healthcare providers also reported that it was difficult for them to receive the results of the initial-reactive test, particularly for clinicians who had not encountered such a situation before. Healthcare providers responded to this experience by informing themselves and gaining the support of laboratory personnel and colleagues: This was a first time for me and I didn't really understand it all very well… I wanted to get all the information I could so that I was ready to answer any questions she had. (GP E) We weren't sure what to do but [I] spoke with [a] colleague and read the policy and protocol that is written and followed that. (Midwife A) She has been with her husband for many years and he has had a test for insurance and was clear so we knew the result was just a lab error and she could not be positive. (GP A) She wasn't a high risk patient and she knew herself that she wasn't high risk. [She] has a husband and five children. (Midwife F) The hard bit was convincing the woman she was alright … . Patients don't always understand and it was quite a challenge for this lady. (GP L) She was a professional woman so seemed to ‘cotton on’ to it all quite well. (GP G) She is an educated woman so understood the process of false positives etc. (GP C) She was a bit taken aback initially but then once I explained it, it was all okay. (Midwife K) I think it depends how credible the doctor's explanation is to the patient as to how well the patient copes with it. (GP K)
Comparison of responses from interviews with both the woman and their healthcare provider
The narratives of the women interviewed could be linked to that of the healthcare providers, and frequently the latter did not appreciate the amount of stress the test result caused. This is demonstrated in the contrasting paired quotes below of healthcare providers and women commenting on the same situation: It was quite shocking at the time. (Tara) I told the woman and she was fine about it. (GP H) I was mortified – as though I had done something wrong. It shocked me. (Michelle) It was not actually a major issue although it could have been. (Midwife H) When she told me I thought ‘Oh my God how could this be… I was just freaking…. ’ (Rachael) The woman was quite relaxed about it. (Midwife C) I tell you Google isn't your friend when something like that happens – you get on there and find out all sorts of things that freak you out. (Rachael) She is an educated person and got onto the internet and studied everything there is to know so she kind of reassured herself. (Midwife C) It was a week before I then got the results back and that was quite stressful waiting (Lisa). The results came back quickly after the re-bleed. (GP M) It was eight days later when I finally got the result. It would have been a whole lot better if I could have known the result within 24 hours but it just took too long. (Hailey) The second test came back quickly so that was good and all in all it went quite smoothly I think. (GP G)
Recommendations from women and healthcare providers
Most of the women, despite having gone through the stress of receiving an initial-reactive test result, still supported antenatal screening for HIV: I would have another HIV test again and I would recommend it to others. I still think it's really important. (Michelle) If they had waited and let me know only after having it all confirmed it would have been better. (Hailey) It was a bit unusual because the routine test result took ages to come back and when it did it just said on the form that the test had been sent for confirmation. There was no phone call or anything to explain. So I phoned the microbiologist and he explained that it showed a very weak HIV but that it had to be re-tested. (GP H) It was great. I got a phone call from the laboratory and [they] explained everything, how it works and a thorough overview of it all…he really gave me the heads up so then I was able to phone my patient and explain it all. (GP C)
Overall, it appeared that, despite the initial surprise of receiving an initial-reactive test result for their patient, the clinicians found the process and support satisfactory. This was particularly so when there was direct communication with the laboratory personnel by telephone and clear advice was provided.
DISCUSSION
This qualitative study of interviews with women who had an initial-reactive screening result for HIV, and with their healthcare providers, has revealed that women experience significant anxiety upon receiving the result, but the extent of this anxiety may be underappreciated by their healthcare providers. Worries for their own health and the health of their children and family, as well as concern over their relationship with a spouse or partner, were paramount. Despite the stress caused, support for the screening programme remained strong among both women and their healthcare providers. Adequate information and timely receipt of results were considered important to alleviate women's anxiety. Similarly, clear, timely and preferably personal communication with laboratory personnel was important for healthcare providers’ understanding of the process.
Similar increased anxiety from receiving a false-positive result has been reported in other screening programmes, such as newborn screening. 9–11 Results from one such qualitative study reported that having to wait for test results increased anxiety, and that good communication with the paediatrician and adequate information and explanation helped reduce stress. 9 Parents of children requiring further hearing tests following newborn hearing screening also reported increased anxiety, which was reduced in those with greater knowledge and understanding, particularly around the meaning of recall for further tests. 10 Whether receiving a false-positive test is a deterrent for future testing has not been reported in pre or postnatal studies, but having a false-positive result was reported to show no difference in re-attendance for breast screening. 12
A strength of our study was the ability to link the interviews from the women with those from their healthcare provider, which allowed us to observe discrepancies in the responses. Also, even though only a small number of women were interviewed, thematic saturation was reached due to the relative homogeneity in feelings expressed by participants. The healthcare providers did act as gatekeepers to the women interviewed, and many of the women, in turn, opted not to participate in an interview. As a result, those women who were particularly inclined to discuss their experiences are more likely to have taken part in the study. While as a qualitative study this research does not seek to generalize to all pregnant women and their healthcare providers who received an initial-reactive test result, the consistency in findings across screening settings suggests a level of transferability to the themes identified. A possible limitation of the study was the brevity of the interviews. The use of a participant-led interview technique and reaching thematic saturation suggest, however, that the primary concerns of participants were identified. A further limitation of the study is that we were unable to accurately provide the rate of initially-reactive tests in the population although an earlier estimate of this was around one per 5000.
The ideal way to alleviate anxiety to women from re-testing is to limit the need for this, by obtaining as much information as possible from the original sample. This would be possible by undertaking a Western blot antibody test on the original sample, but this option was discounted in the original NSU algorithm as taking too long to give a conclusive result, especially in an early infection.
3
It was, however, estimated at the outset of the HIV antenatal screening programme that nearly all pregnant women infected with HIV would have established HIV infection. Moreover, the HIV test is normally undertaken along with other blood tests at an early stage in the pregnancy, so there is time to confirm the woman's HIV status before the delivery. If the current algorithm for re-testing is continued, healthcare providers need to anticipate and be trained to deal with, the major anxiety that this will generate in the women. Measures suggested from this work to moderate this impact include:
Obtaining the best information on the likelihood of the final result prior to seeing the woman who requires re-testing. This is probably best achieved through direct communication with a clinical microbiologist or infectious disease specialist. Good communication and the ability to explain rates and reasons for initial-reactive results will assist the few women who require re-testing.
13
Having the re-test results from the laboratory, and communicating these to the woman, as soon as possible.
These findings are particularly relevant in a country such as New Zealand, where the very low prevalence of undiagnosed HIV among pregnant women means that there are likely to be more inconclusive initial HIV tests among uninfected than infected women.
Footnotes
ACKNOWLEDGEMENTS
This study was funded by the National Screening Unit, New Zealand Ministry of Health. The views expressed in this paper are those of the authors and do not necessarily reflect those of the funder.
The authors wish to acknowledge Professor Charlotte Paul, Dr Beverley Lawton and Dr Chrystal Jaye for useful comments on an earlier draft of this paper.