
Abstract
Objectives
In 2007, Australia implemented an ongoing, school-based human papillomavirus (HPV) vaccination programme for school-aged girls, and a catch-up programme for 18–26-year-old women that ran until the end of 2009. The availability of what is widely known as the ‘cervical cancer vaccine’ means there is the potential for women to believe, incorrectly, that they no longer require regular cervical screening, and this risk needs to be addressed. The current study aimed to assess the effect of three mass media campaigns to promote cervical screening on the rate of cervical screening tests in the Australian state of Victoria, after HPV vaccine became available.
Methods
Seasonal time series assessed the effect of media campaigns broadcast in 2007, 2009 and 2010 on the rate of weekly cervical screening tests in Victorian women from 2006 to 2010, stratified by time since last screening test.
Results
The 2007 and 2009 media campaigns significantly increased the number of cervical screening tests per week. The 2007 campaign had a significant impact on lapsed screeners (>36 months since last test), overdue screeners (28–36 months since last test), and women never previously screened. The 2009 campaign significantly increased screening tests for overdue screeners, and the 2010 media campaign was associated with a significant increase in screening tests for lapsed screeners.
Conclusions
A well-researched and carefully pretested television advertising campaign with accurate, actionable messages can elicit appropriate screening behaviour among some of the appropriate groups even in a changed environment of complex, and potentially competing, messages.
INTRODUCTION
Over the last 50 years, screening for cervical cancer precursor lesions with Papanicolaou (Pap) tests has been the main method used for the prevention of cervical cancer. In Australia and other developed countries where well-organized screening programmes have been instituted, the reduction in incidence and mortality from cervical cancer has been dramatic. 1 Cervical screening testing has imperfect sensitivity, so women need to attend for regular screening. 2 In Australia, the national policy is for women to attend for screening every two years from the time they are aged 18 (or 1–2 years after sexual intercourse, whichever is later) until they reach age 69.
In Australia, first-time cervical screening is initiated by the woman, and she can choose any practitioner. In Victoria, the second most populous state in Australia, after a woman has had her first cervical screening test she is listed on the Victorian Cervical Cytology Register (VCCR) (unless she chooses otherwise). VCCR sends a reminder letter to women whose screening test is overdue (27 months after a normal test). If women fail to respond to that reminder, they will not routinely be contacted again. Some cervical screening providers send reminder letters to their patients; however, this is organized by individual practices, so is not comprehensive. Thus, there are limited opportunities to communicate with women directly if they do not present for screening at appropriate intervals.
Mass media campaigns in conjunction with organized screening have been shown to increase cervical cancer screening, 3 although dedicated reviews on the subject are a decade old, and more is now known about the response of population subgroups. 4,5 For example, a mass media campaign developed in 2004 in Victoria was able to increase the Pap test rate among women who were overdue for their cervical screening test in both Victoria 6 and New South Wales, 7 and to be equally effective in doing so across socioeconomic groups. 8 Mass media campaign messages to promote cervical screening need to be carefully developed and pre-tested prior to implementation to ensure that they motivate women who need a cervical screening test, without prompting undue concern, or action, among those who do not.
Since the development of highly effective human papillomavirus (HPV) vaccines, the context in which cervical screening takes place has become more complex from a public education perspective. Both of the available vaccines (Gardasil®: CSL Biotherapies, Parkville, VIC, Australia, and Cervarix®: GlaxoSmithKline, Abbotsford, VIC, Australia) prevent infection with HPV 16 and 18, the two HPV types responsible for 70% of cervical cancer globally and approximately 50% of high-grade cervical lesions. 3,4,9,10 However, the vaccines need to be given before a woman is exposed to HPV, and do not provide protection against all oncogenic HPV types. Therefore, regular cervical screening tests are still recommended, even for women who have been vaccinated.
Australia implemented a broad HPV vaccination programme between 2007 and 2009, which provided the three-dose course of Gardasil® vaccine to all women aged 12–26 years. Immunization is now available free-of-charge only as part of a school-based vaccination programme for girls aged 12–13 years.
The introduction of the HPV vaccine has been a welcome initiative in efforts to reduce the incidence of cervical cancer. However, cervical screening participation by young women was already gradually declining over the past decade in Australia and other countries. 11 There has been concern that the availability of the vaccine might exacerbate the decline in young women's cervical screening rates, given the potential for women to misunderstand the limitations of the vaccine. A Victorian population study showed that among young, unvaccinated women, only 62.5% realized that the vaccine could not be used to treat cervical cancer or abnormalities. 12
In Australia, public education materials about the vaccine, produced by the National HPV Vaccination Program and by the vaccine manufacturers, included the information that the vaccine did not replace the need for screening. However, the message about preventing cervical cancer was also prominent: Protecting yourself from cervical cancer (National HPV Vaccination Program brochure); Join the fight against cervical cancer (CSL Biotherapies). The vaccine was also widely referred to in the news media as ‘the cervical cancer vaccine’, with headlines such as Cancer jabs for girls, 13 which could potentially counteract less salient messages about the ongoing necessity for screening.
News media coverage can be a positive influence, such as when Jade Goody, a well-known British reality television personality, was diagnosed with cervical cancer in 2008. The widespread media coverage of her diagnosis and death led to increases in cervical cancer screening and colposcopy referrals for women in Britain, particularly among younger women 14 and those from lower socio-economic backgrounds. 15 However, ‘newsworthy’ cancer screening media coverage may not support the aims of established screening programmes, or deliver ‘balanced and action-oriented content’. 16 Given the complex message environment, there is potential for women to misunderstand the limitations of the HPV vaccine and forego regular cervical screening tests after receiving it.
This study examines the effectiveness of three targeted mass media campaigns, broadcast in 2007, 2009 and 2010 in Victoria that promoted appropriate cervical screening test attendance against a background of the provision of the new HPV vaccine and the ensuing public awareness of the vaccine.
METHODS
VCCR data
VCCR is an opt-off, confidential, computerized database of Victoria women's cervical screening test results (
De-identified registry data from 1 January 2006 to 31 December 2010 were released to the investigators with the approval of the Cancer Council Victoria Human Research Ethics Committee. The data comprised: a randomized ID number, the date that the test was conducted, the woman's postcode, the pathology recommendation code, her age at the time of testing, and the time since her last screening test (screening interval), if any.
Screening interval groups were defined as: (1) <21 months since last cervical screening test (Early re-screeners), (2) 21–27 months since last screening test (Appropriate screeners), (3) 28–36 months (Overdue screeners), (4) >36 months (Lapsed screeners), and (5) women with no recorded Victorian test history (Never tested).
Mass media campaigns
Three state-wide mass media campaigns were broadcast in 2007, 2009 and 2010 to encourage women who had never had a cervical screening test and those overdue for their test to have one. The Don't Just Sit There (DJST) campaign was first broadcast on free-to-air television in 2004, 6 then again in 2005, 8 but we did not have access to data for those years in a format comparable with that for the more recent years. The DJST campaign was repeated in 2007, in the weeks commencing 10 and 17 September and 8, 15 and 29 October. In 2009, it was broadcast in the weeks 8, 15, 22 June, 19 July and 2 August. For each year we defined the ‘campaign period’ as the time the advertisement was on air plus an additional week at the end, based on research showing that campaign effects extend for a short period after the broadcast ends. 18 We previously observed this effect in past work, 6 which may be due to the time it takes women to organize to have a Pap test.
Target audience rating points (TARPs) were obtained for the campaigns. TARPs are a measure of campaign exposure, based on the proportion of a specific target audience – in this case metropolitan women aged 25–54 – estimated to be viewing the programmes in which the advertisements are broadcasted. Higher TARPs indicate greater potential exposure to the campaign. In 2007, TARPS totalled 730 over eight weeks (average per week = 91 or 100% of women viewing the advertisement 0.91 times) and in 2009, they totalled 914 over eight weeks (average per week = 114 or 100% of women viewing the advertisement 1.14 times).
Although a 30-second television advertisement does not enable complex messages to be explained fully– such as the link between HPV and cervical cancer and need for ongoing cervical screening – qualitative research indicated that modifying the voice-over for the DJST advertisement after the introduction of the vaccine could improve knowledge. The revised opening line of the advertisement captured attention with the statement ‘Now that there is a new cervical cancer vaccine do women still need Pap tests? Yes!’ The opening of the advertisement was also modified so that it began with a written graphic on screen stating, ‘There's a new cervical cancer vaccine’ (
The vaccine message was also incorporated into a new advertisement, developed in 2010, called Peace of Mind (PoM) (
Each of the televized media campaigns was supported by smaller investments in radio, print advertising and posters. The messages of DJST and PoM were based on findings from quantitative surveys indicating discomfort and ‘not getting around to it’ were key barriers to having a Pap test, and the advertisements were developed after extensive qualitative research to ensure they resonated with their target audiences.
Statistical analysis
All analyses were conducted using Stata 11.2, Texas, USA. 19 Victorian cervical screening tests were aggregated by week. As the data exhibited a strong cyclical pattern, with large, temporary decreases in weekly screening tests over the summer holiday period (December–January), seasonal autoregressive integrated moving average (SARIMA) time series were conducted. SARIMA models account for variation both within and across seasons. Separate multivariate SARIMA models were conducted for women overall, and then for each screening interval to estimate the effect of the 2007, 2009 and 2010 mass media campaigns on weekly cervical screening tests.
A SARIMA model is written as (p, d, q)(P, D, Q) s , where s is the seasonal cycle, p and q the non-seasonal autoregressive and moving average parameters, P and Q the seasonal autoregressive and moving average parameters, and d and D the non-seasonal and seasonal differencing of orders, respectively. 20 For fitting the SARIMA models for each screening interval, seasonality was taken into account by using 52 weeks as the seasonal differencing factor. The seasonal and non-seasonal autoregressive and moving average parameters were included where appropriate, and must be significant to remain in the model. Acceptable model fit is evidenced by residuals resembling white noise, as indicated by a non-significant Box-Ljung Q-test and by non-significant correlations on the residual autocorrelation function over 24 months.
The three mass media campaigns consisted of three dummy coded variables; that is, weeks in which a mass media campaign was broadcast plus one week after each advertising ‘block’ were coded as 1, and all other weeks as 0.
RESULTS
From 2006 to 2010, there were 2,742,838 cervical screening tests registered in Victoria. Excluded from the analysis were women with a clinical diagnosis from a test, which could necessitate rescreening more frequently than two yearly, as well as those who had more than an annual test (5 tests during the 5-year period) without an identifiable clinical justification. In addition, women whose postcode of residence was outside Victoria were removed before analysis. Only women aged 20–69 years were included in the analysis. A total of 2,371,709 cervical screening tests for 2006–2010 remained in the data-set.
The data were then aggregated by week for each screening interval category. Figure 1 shows that the largest number of screening tests fell within the ‘Appropriate screeners’ (21–27 months) category, with the lowest number of tests occurring for those who had never had a previous screening test. In addition, the strong annual pattern in the data is apparent within each screening interval group, with a large decrease in weekly screening tests over the summer months (December–January).
Weekly cervical screening tests from 2006 to 2010 for women in Victoria, Australia, by screening interval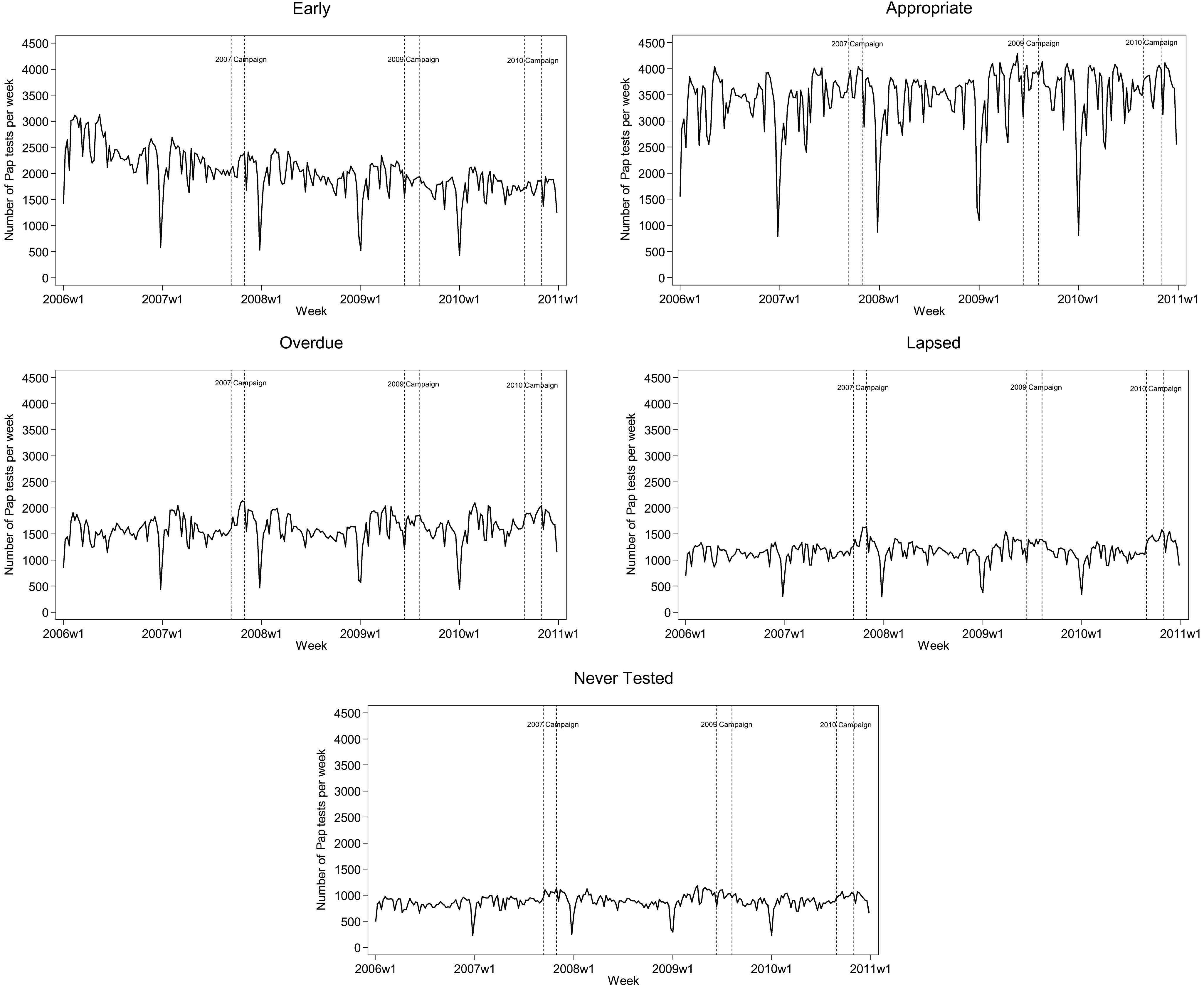
Parameter estimates for the SARIMA time series of weekly Victorian women's cervical screening tests, January 2006 to December 2010
CI, confidence interval
DISCUSSION
The impact of the media campaigns varied across the years, but none prompted an increase in early rescreening. Historically, early rescreening (having another test within 21 months of a negative test) has been an issue, with premature test rates as high as 43% in 1996, 21 declining to 22% by 2007. 22 The method for calculating early rescreening has changed slightly in that time, but all indications are that the problem has been diminishing. It is reassuring that there is no indication that the media campaigns influenced women to screen unnecessarily.
None of the campaigns led to additional screening among the women whose tests were almost due or up to three months overdue, although there was a trend for this in 2009. These women were not the target audience, as many would probably have presented for a test soon regardless of the media campaign, so it is encouraging that the campaign did not just ‘borrow from the future’. It may also be that these women did not perceive themselves as needing a Pap test yet, as the prompt of the VCCR reminder letter is not sent until a woman's test is three months overdue.
The campaign had different positive impacts across different years. The 2007 campaign was the most broadly successful, leading to increased screening overall and among all the appropriate groups, i.e. those women who had never had a cervical screening test, those who were overdue (3–9 months since a test) and those who had let their screening lapse (no test for more than 3 years).
The greater success of the 2007 campaign cannot be explained by more population exposure to the advertisement, as the overall TARPs and weekly averages were lower in 2007 (730; 91) than in either 2009 (914; 114) or 2010 (915; 92). The inclusion of the HPV message within the 2007 advertisement may have increased message salience: unpublished telephone survey data collected at the end of the 2007 campaign indicated that 25.2% of the 485 respondents who could recall seeing the television advertisement indicated it ‘told them something new’. This contrasts with 2004, when the advertisement was broadcast for the first time but did not contain an HPV message, when only 7% of the 567 women who recalled it thought the message was new. 23,24 In addition, the context of the introduction of the HPV vaccine (or ‘the cervical cancer’ vaccine) meant that cervical cancer had a greater media profile than usual, including some television advertising by GlaxoSmithKline promoting the Cervarix® vaccine. Rather than detracting from the screening message, the HPV vaccine's media profile may actually have enhanced the advertisement's salience.
The 2009 advertising campaign also significantly increased overall rates of screening but by a smaller amount than the same advertisement used two years previously. Campaign-attributable screening was apparent only among women whose test was overdue, with trend for increase among those with no previous test. This narrower benefit could be related to the fact that that the Don't Just Sit There campaign had been used over a number of years by then and was less new or relevant.
The new 2010 campaign positively influenced the behaviour of women who had gone for more than 3 years without a cervical screening test, with a trend for an increase among never screeners.
Although it was disappointing that the 2009 and 2010 campaigns did not influence all at-risk groups, detecting a benefit among the overdue and lapsed screeners is important because they are among the most difficult to reach, as the Registry only sends one reminder letter to women (at 27 months). Furthermore, if women whose test is more than three years overdue can be motivated to have another, they then return to the routine reminder system, thereby increasing the possibility that they may resume regular screening.
The strength of the current study is that using time series provides a robust test of campaign impact using long-term data, after accounting for seasonal trends, auto-regression and moving averages in the data. The analysis also allowed for the examination of differential effects of the campaign for each screening interval group, by using models specific to each subgroup.
CONCLUSION
Overall, this study suggests that well-researched and carefully pretested television advertising campaigns with accurate, actionable messages promoting cervical screening can elicit population-based behavioural change among some of the appropriate population subgroups, even in a broader environment of complex and potentially confusing messages. An important factor was the capacity to adapt an existing cervical screening media advertisement to include an HPV message in the voice-over when the vaccination programme was announced. Further research is needed to determine the optimum frequency for broadcasting media campaigns, and the extent to which messages require refreshing in order to influence all at-risk population subgroups. Another avenue for further research would be study of campaign impact among different population groups, particularly the impact on young, vaccinated women.
Footnotes
ACKNOWLEDGEMENTS
The study was funded by PapScreen Victoria. PapScreen is a joint Commonwealth-State funded programme delivered by Cancer Council Victoria. We are very grateful to the staff at the VCCR for facilitating access to the cervical screening data.