
Abstract
Objective
To evaluate the extent and histopathological characteristics of asymptomatic breast cancer detected outside the Norwegian Breast Cancer Screening Program (NBCSP) in women targeted by the programme.
Methods
Our study included 568 primary breast cancers (523 invasive and 45 ductal carcinoma in situ) diagnosed in 553 women aged 50–70, residing in Møre og Romsdal County, 2002–2008. The cancers were divided into screening-detected cancers in the NBCSP, interval cancers (ICs) and cancers detected in women not participating in the NBCSP (never participated and lapsed attendees), and further into asymptomatic and symptomatic cancers. Nottingham Prognostic Index (NPI) was used for comparisons across the groups and the distributions were compared using chi-square tests for statistical significance.
Results
Twenty percent (19/97) of the ICs and 32% (69/213) of the breast cancers in non-participants were asymptomatic, with opportunistic screening as the most frequent detection method (42%, 8/19 for ICs and 54%, 37/69 for non-participants). There were no differences in distribution of NPI prognostic categories across subgroups of asymptomatic invasive cancers (screening-detected cancers in the NBCSP, asymptomatic ICs and asymptomatic cancers in non-participants) or between subgroups of symptomatic invasive cancers (symptomatic ICs and symptomatic cancers in non-participants). Asymptomatic cancers had a significantly more favourable distribution of NPI prognostic categories compared with symptomatic cancers (P < 0.001). The proportion of invasive cancers with excellent/good NPI was 53% (164/310) for all asymptomatic and 25% (52/211) for all symptomatic invasive cancers.
Conclusions
A considerable percentage of breast cancers detected outside the organized screening programme were asymptomatic, with a prognostic profile comparable with screening-detected breast cancers in the NBCSP. Individual data regarding the detection method for all breast cancers are needed for a complete evaluation of the organized screening programme in Norway.
Introduction
According to unpublished results, the participation rate in the Norwegian Breast Cancer Screening Program (NBCSP) varies between 55% and 85% by county. An extensive use of opportunistic screening in private institutes prior to the implementation of the NBCSP,10,11 as well as after the screening programme started, 12 has been reported. The varying participation rate in the NBCSP might be attributable to some women preferring opportunistic screening to participating in the organized programme. If, consequently, asymptomatic cancers are being diagnosed among non-participants in the NBCSP, this has to be taken into account in studies evaluating the effectiveness of the Norwegian screening programme. If it is not, the potential benefit of attending screening mammography will be underestimated. Furthermore, the interval cancer rate is often used as a quality measure of a service screening programme. If some of the interval cancers are asymptomatic cancers detected by opportunistic screening, the outcomes of these quality assurance measures might be misleading.
The objectives of our study were to evaluate the extent and histopathological characteristics of asymptomatic cancers detected outside the NBCSP. We firstly quantified the percentage of asymptomatic interval cancer and asymptomatic breast cancer in 50–70 year old women not participating in the NBCSP. Secondly, we analysed and compared prognostic factors within and between asymptomatic and symptomatic cancers.
Methods
The study was approved by the Regional Committee for Medical and Health Research Ethics, The Norwegian Social Science Data Services, The Data Inspectorate and The Norwegian Directorate of Health. The study was performed with passive consent (all women received written information about the project and had the opportunity to withdraw from the study).
The Service Screening Programme In Møre Og Romsdal
The study was performed with data from the service screening programme in Møre og Romsdal County, which is a part of the NBCSP. The NBCSP offers women aged 50–69 two view screening mammography every second year. The programme is described in detail elsewhere. 13 Women invited to participate in the programme can opt out from receiving invitations, and as of 2012 about 3% of women targeted by the programme have done so (unpublished quality assurance parameters). This percentage ranges from 1% to 8% by county and is 8% in Møre og Romsdal. The participation rate in Møre og Romsdal is 72% of those invited, compared with 78% nationwide (Table 1). 13 The target population for the NBCSP in Møre og Romsdal County is approximately 25,000 women, representing about 5% of the total target population for the NBCSP. Further results of early performance measures from the NBCSP in Møre og Romsdal are shown in Table 1.
Early outcome measures of the NBCSP in Møre og Romsdal County, 2002–2008
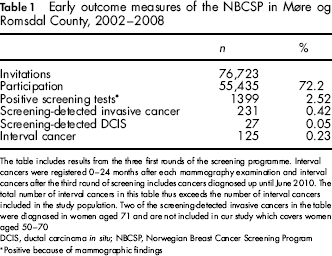
The table includes results from the three first rounds of the screening programme. Interval cancers were registered 0–24 months after each mammography examination and interval cancers after the third round of screening includes cancers diagnosed up until June 2010. The total number of interval cancers in this table thus exceeds the number of interval cancers included in the study population. Two of the screening-detected invasive cancers in the table were diagnosed in women aged 71 and are not included in our study which covers women aged 50–70
DCIS, ductal carcinoma in situ; NBCSP, Norwegian Breast Cancer Screening Program
Positive because of mammographic findings
Study Population
The Cancer Registry of Norway identified all women aged 50–70 residing in Møre og Romsdal and diagnosed with breast cancer (invasive and ductal carcinoma in situ [DCIS]) in the period April 2002 to start of September 2008 (N = 563). This corresponds with the three first screening rounds in the county. Although the upper age limit for the NBCSP is 69, several invited women are screened at the age of 70 because of the biennial screening interval. The age group included in our study was thus 50–70 years. Three women declined to participate in the study and seven women with secondary breast cancer in the ipsilateral breast were excluded from the analyses. Fifteen women were diagnosed with bilateral breast cancer during the study period. Bilateral cancers represent two histopathological distinct cancers, which might have different methods of detection and were therefore included and analysed as two individual cases. The study thus includes 568 primary breast cancers (523 invasive and 45 DCIS) diagnosed in 553 women.
Data Extraction
Information about detection method and histopathological tumour characteristics was obtained from the Cancer Registry of Norway. Detection methods for interval cancers and cancers in non-participants were cross-checked with the patient's medical records and the records were also examined in cases with missing data. We defined interval cancer according to the European Guidelines 14 and included all cancers diagnosed within 24 months of a negative screening examination in the NBCSP.
Detection Methods
The cancer cases were classified as
Screening-detected cancer in the NBCSP; Interval cancer in women participating in the NBCSP; Cancer detected in women not participating in the NBCSP (hereafter referred to as cancer in non-participants).
Cancers in non-participants included both cancers in women who had never attended the programme and cancers in lapsed attendees, i.e. cancers diagnosed outside the programme more than 24 months after a negative screening examination in the NBCSP. Two cases classified as interval cancers in official statistics from the NBCSP (one invasive and one DCIS) were diagnosed on a scheduled short time follow-up after a positive screening examination. In our study we defined these two cases as screening-detected because they were diagnosed as the consequence of a screening examination. This is in accordance with the European Guidelines. 14
We further divided the cancer cases into asymptomatic and symptomatic, depending on the indication for the diagnostic mammography examination. Symptomatic cancer was defined as cancer diagnosed secondary to symptoms that corresponded with the diagnosed malignancy (same side and location). All other cancers were defined as asymptomatic.
Asymptomatic cancer:
Screening-detected (in the NBCSP or by opportunistic screening); Routine examination in patients with increased risk of breast cancer (previous breast cancer in the contra-lateral breast, positive family history defined by the referring physician, estrogen therapy); Follow-up because of previous findings (includes short-term follow-up because of minimal signs of pathology on a previous mammogram or because of fibroadenomatosis or other benign conditions); Incidental finding (the woman had been referred because of a palpable lump or other breast symptoms that did not correspond with the cancer that was diagnosed). Symptomatic cancer:
Palpable breast lump; Other breast symptoms (nipple discharge, pain, tenderness); Palpable axillary lump; Diagnosis prompted by symptomatic distant metastasis.
Nottingham Prognostic Index
Nottingham Prognostic Index (NPI) is a prognostic index for patients with primary, operable invasive breast cancer, combining tumour size, nodal status and histological grade. 15 Depending on the NPI, the patients can be placed in different prognostic categories. The method was developed in 1979–198215,16 and is validated in several studies.17–20 We calculated the NPI for all primarily operated invasive cancers and assigned them to the following prognostic categories: (a) excellent/good, (b) moderate and (c) poor. Because of missing data on tumour size, NPI could not be calculated for locally advanced tumours or for tumours that were not excised because of distant metastasis (n = 35). However, to include these cancers in the comparisons we assigned them to the poor prognostic category (c).
Statistical Analysis
The distribution of screening-detected cancers in the NBCSP, interval cancers and cancers detected in non-participants was given in numbers and percentages. The distribution of NPI prognostic categories was compared between subgroups of asymptomatic and symptomatic invasive cancers as well as between all asymptomatic and all symptomatic invasive cancers. The distribution of cancers detected in participants and non-participants in the NBCSP per year, as well as the distribution of asymptomatic and symptomatic cancers in non-participants per year, was illustrated graphically.
We performed statistical analysis using SPSS. Distribution of NPI prognostic categories were compared with cross table methods and tested for significance using Pearson's chi-square test. A P value of <0.05 was considered statistically significant.
A previous study reported that 50% of screening-detected cancers had excellent/good prognostic NPI. 20 Under the assumption that 50% of the asymptomatic invasive cancers would have excellent/good prognostic NPI, we performed a power analysis given our actual sample sizes. The analysis revealed 80% power at anα-level of 0.05 for detecting a 13 percentage point difference in cases with excellent/good prognostic NPI between all asymptomatic and all symptomatic invasive cancers.
Results
Distribution of Cancers: Participants and Non-Participants in the Nbcsp
A total of 45% (258/568) of all the cancers (DCIS and invasive) diagnosed in the study population during the study period were screening-detected in the NBCSP; 17% (97/568) were interval cancers and 38% (213/568) were diagnosed in non-participants (Figure 1). DCIS constituted 8% (45/568) of all cancers: 10% (26/258) of the screening-detected cancers in the NBCSP, 5% (5/97) of the interval cancers and 7% (14/213) of the cancers in non-participants.
Detection methods for breast cancer cases in women aged 50–70, Møre og Romsdal County 2002–2008. *The number of cases is adjusted for excluded cases (women who declined to participate and women with secondary cancer in the ipsilateral breast). Two cases that were registered as interval cancers in the official statistics from the NBCSP (Table 1) were defined as screening-detected cancers in our study, because they were diagnosed on a scheduled short time follow-up after a positive screening examination in the NBCSP. **Norwegian Breast Cancer Screening Program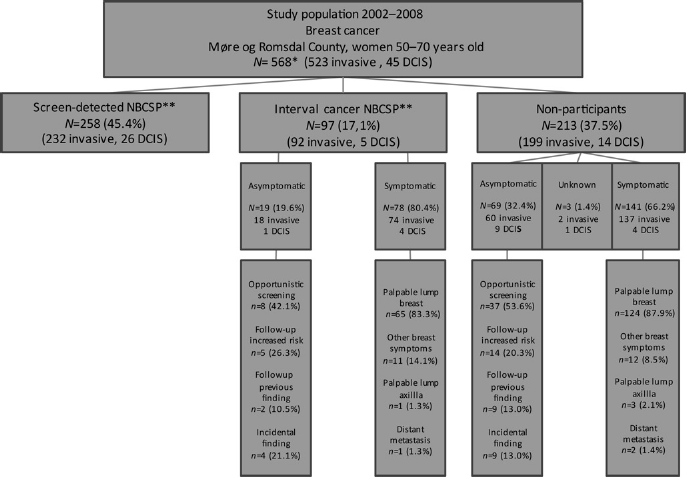
In 2002 38% (26/68) of the cancers were detected among participants in the NBCSP (Figure 2). This percentage increased as the coverage became complete and after 2003 more than 65% of the cancers were detected among participants in the NBCSP.
Distribution of breast cancers (DCIS and invasive cancers) diagnosed in participants (screening-detected and interval cancers combined) (N = 355) and non-participants (N = 213) in the NBCSP; women aged 50–70, Møre og Romsdal County 2002–2008. DCIS, ductal carcinoma in situ; NBCSP, Norwegian Breast Cancer Screening Program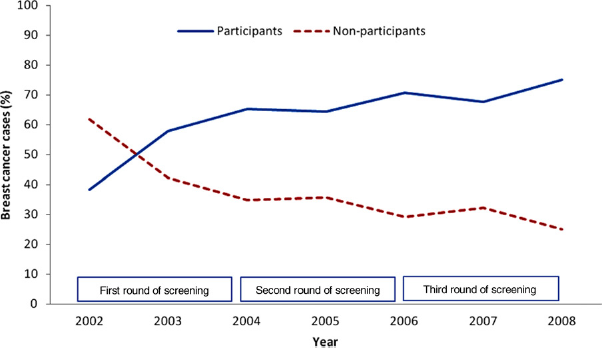
Distribution of Asymptomatic And Symptomatic Cancers: Interval Cancers And Breast Cancers In Non-Participants
Interval Cancers (N = 97)
Twenty percent (19/97) of the interval cancers were asymptomatic. The rate was 20% both for DCIS (1/5) and invasive cancers (18/92). Opportunistic screening was the most common detection method (42%, 8/19), followed by increased risk of breast cancer (26%, 5/19), incidental findings at mammography prompted by other symptoms (21%, 4/19), and follow-up because of previous findings (11%, 2/19). The remaining cases (80%, 78/97) were symptomatic.
Breast Cancers In Non-Participants (N = 213)
A total of 32% (69/213) of the breast cancers diagnosed in non-participants were asymptomatic. The percentage was higher for DCIS (64%, 9/14) than for invasive cancers (30%, 60/199, P = 0.015). Opportunistic screening was the most common detection method (54%, 37/69), followed by increased risk of breast cancer (20%, 14/69), incidental findings (13%, 9/69) and follow-up because of previous findings (13%, 9/69). A minor percentage of the breast cancers detected in non-participants had unknown detection mode (1%, 3/213). The remaining 66% (141/213) were symptomatic.
During the first years of the study period 24–26% of the breast cancers diagnosed in non-participants were asymptomatic (10/42 in 2002, 12/46 in 2003 and 8/31 in 2004), rising to 47% during the last years (9/19 in 2006, 14/30 in 2007 and 7/15 in 2008) (Figure 3).
Distribution of asymptomatic (N = 69) and symptomatic (N = 141) breast cancers diagnosed in non-participants in the NBCSP; women aged 50–70, Møre og Romsdal County 2002–2008. NBCSP, Norwegian Breast Cancer Screening Program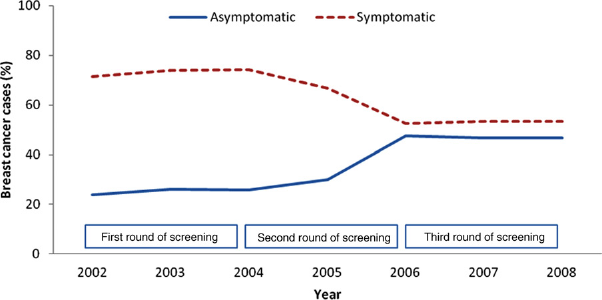
Nottingham Prognostic Index
Subgroups of Asymptomatic And Symptomatic Invasive Cancers
We observed no statistically significant differences in the distribution of NPI prognostic categories across the three different subgroups of asymptomatic cancer (P = 0.924) (Table 2). The percentages of cancers with excellent/good NPI were 54% for screening-detected cancers in the NBCSP, 50% for asymptomatic interval cancers and 48% for asymptomatic cancers in non-participants.
Nottingham Prognostic Index (NPI) for invasive breast cancers in women aged 50–70, Møre og Romsdal County 2002–2008
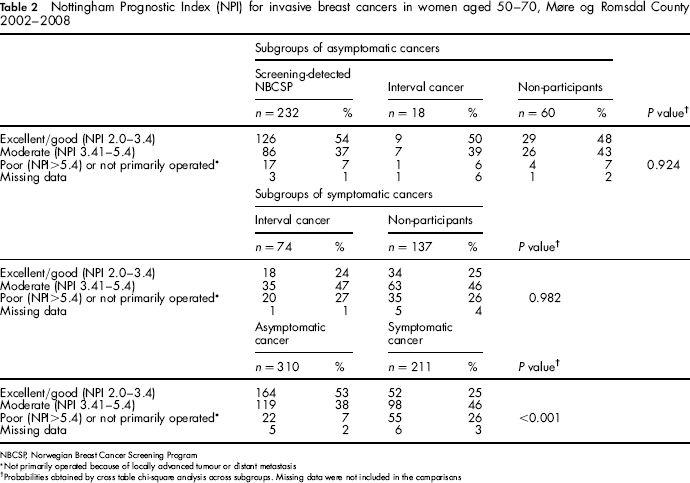
NBCSP, Norwegian Breast Cancer Screening Program
Not primarily operated because of locally advanced tumour or distant metastasis
Probabilities obtained by cross table chi-square analysis across subgroups. Missing data were not included in the comparisons
Furthermore, we did not observe any statistically significant differences in the distribution of NPI prognostic categories when comparing symptomatic interval cancers with symptomatic cancers in non-participants, P = 0.982 (Table 2). In both subgroups about 24% of the cancers had excellent/good prognostic NPI.
All Asymptomatic Versus All Symptomatic Invasive Cancers
We found a significantly more favourable distribution of NPI categories for all asymptomatic compared with all symptomatic invasive cancers (P < 0.001; Table 2). The percentage of cancers with excellent/good NPI was 53% (164/310) for all asymptomatic and 25% (52/211) for all symptomatic invasive cancers. This yields a relative risk of 2.1 (95% CI 1.7–2.8) in favour of asymptomatic cancers.
Discussion
Our study showed that 20% of interval cancers and 32% of breast cancers detected in non-participants in the NBCSP were asymptomatic, with a prognostic profile comparable with screening-detected breast cancers in the programme. Opportunistic screening was the most common detection method for these asymptomatic cancers. Our study did not investigate why some women preferred opportunistic rather than organized screening. Enrolments in opportunistic screening programmes prior to the first invitation to the NBCSP, closer geographical location to the screening site, or other personal preferences are possible explanations. Some women might also want to be screened annually and choose to attend the NBCSP every second year and a private institute in the years in between.
Routine mammography in women with increased risk of breast cancer was another important detection method for asymptomatic cancers outside organized screening. In our study, increased risk was defined as a positive family history of breast cancer, previous breast cancer in the contra-lateral breast, or exposure to estrogen therapy. Women with increased risk often attend mammography on a yearly basis. In order to do so they must either opt out from the organized programme altogether or have clinical mammography in public or private institutes in the years in between organized screening.
Asymptomatic invasive cancers showed a more favourable distribution of NPI prognostic categories than symptomatic invasive cancers. The percentage of cancers with excellent/good NPI was 53% for all asymptomatic and 25% for all symptomatic invasive cancers. We found no significant differences in distribution of prognostic categories when comparing screening-detected cancers in the NBCSP with asymptomatic interval cancers and asymptomatic cancers in non-participants, or when comparing symptomatic interval cancers and symptomatic cancers in non-participants. Previous studies have concluded that screening-detected breast cancers have a more favourable prognostic profile than interval cancers and cancers detected in non-participants6–9 which is as expected due to lead time. Our results suggest, however, that the prognostic profile depends on whether the cancer is asymptomatic or symptomatic, rather than on whether it is diagnosed as the results of participating in an organized screening programme or not. All asymptomatic cancers might thus be referred to as ‘screening-detected’ and ought to be taken into consideration when the effect of a screening programme is evaluated. In order to identify these asymptomatic cancers, there is a need for individual data regarding the detection method for all women with breast cancers. The lack of individual data regarding cancers detected outside the NBCSP represents a limitation in several studies evaluating the effectiveness of the programme.21–23
Our study does not include data on mammography activity prior to the implementation of the NBCSP in Møre og Romsdal. However, given the amount of asymptomatic cancers detected among non-participants even after the commencement of organized screening, it seems reasonable that asymptomatic cancers were also detected before the programme was implemented. This is in line with the study of Olsen et al. which found that widespread use of mammography in the prescreening period represents a bias in the evaluation of the NBCSP. 23
It takes two years to invite all eligible women when starting up a biennial screening programme. In our study 38% of all cancers diagnosed during the first year of screening were within the programme, rising to 65–70% per year when the coverage was complete. The high percentage of cancers diagnosed in non-participants during the first round of screening is an important factor that must be acknowledged when evaluating a screening programme.
In Møre og Romsdal the interval cancer rate during the three first rounds was 0.23% of all screens (Table 1). If we assume that approximately 80% of these interval cancers were symptomatic, this gives a symptomatic interval cancer rate of 0.18%. When the interval cancer rate is used as a quality measure of a screening programme, 14 it would thus be reasonable to adjust for the number of asymptomatic cases, or else the rate will be overestimated.
Cancers in participants and non-participants of the NBCSP were diagnosed during the same time period, eliminating any temporal bias caused by increased breast cancer awareness or improved diagnostic performance. The women resided in the same county. The data-set was almost complete and only 0.5% of the women declined to participate in our study. The Cancer Registry database is considered more than 98% complete on solid tumours. 24
The main limitation to our study is the small study group. However, using the NPI, which combines three different prognostic factors, it is possible to demonstrate statistically significant differences between asymptomatic and symptomatic breast cancers. Our study does not include mammography history for cancers detected in non-participants. Hence, we do not know if some of these cases could be labelled as ‘interval cancers’ after negative opportunistic screening or negative clinical mammography in the 0–24 months prior to the diagnostic examination. The attendance rate is lower and the opt-out rate is higher in Møre og Romsdal compared with the average for the NBCSP. Care should therefore be exercised in generalizing our findings to all the other counties in Norway.
Conclusions
A considerable percentage of breast cancers detected outside the organized programme in women aged 50–70 were asymptomatic, with a prognostic profile comparable with screening-detected cancers in the NBCSP. These cancers were most commonly detected by opportunistic screening, but increased risk of breast cancer, follow-up of previous findings and incidental findings also contributed as detection methods. Our findings emphasize the importance of individual data regarding detection method for all breast cancers. Lack of such information will hamper a complete evaluation of the organized screening programme in Norway.