
Abstract
Objectives
Flexible sigmoidoscopy (FS) screening for colorectal cancer will be introduced into the National Cancer Screening Programmes in England in 2013. Patient-reported outcome measures (PROMs) from trial participants indicate high acceptability and no adverse physical or psychological consequences, but this may not generalize to routine screening in the community. This study examined PROMs in a community-based FS screening programme.
Methods
Eligible adults aged 58–59 (n = 2016) registered at 34 London general practices were mailed a National Health Service-endorsed invitation to attend FS screening. Pain and side-effects were assessed in a ‘morning-after’ questionnaire, and satisfaction was assessed in a three-month follow-up questionnaire. Anxiety, self-rated health and colorectal symptoms were assessed at prescreening and follow-up.
Results
In total, 1020 people attended screening and were included in the current analyses, of whom 913 (90%) returned the morning-after questionnaire, and 674 (66%) the follow-up questionnaire. The prescreening questionnaire had been completed by 751 (74%) of those who attended. The majority (87%) of respondents reported no pain or mild pain, and the most frequent side-effect (wind) was only experienced more than mildly by 16%. Satisfaction was extremely high, with 98% glad they had the test; 97% would encourage a friend to have it. From prescreening to follow-up there were no changes in anxiety or self-rated health, and the number of colorectal symptoms declined. Satisfaction and changes in wellbeing were not moderated by gender, deprivation, ethnicity or screening outcome.
Conclusions
PROMs indicate high acceptability of FS screening in 58–59 year olds, with no adverse effects on colorectal symptoms, health status or psychological wellbeing.
Introduction
Because screening tests are offered to people who are typically asymptomatic and ‘healthy’, the psychological costs and benefits of screening participation are important clinical indicators. Patient-reported outcomes measures (PROMs) are therefore an essential component of the evaluation. 6 They also help to identify opportunities to improve the screening service, and make it possible to identify socioeconomic or ethnic differences in the experience of screening that could contribute to inequalities in uptake. 7
In both the UK and the Norwegian Trials, acceptability of FS screening was very high.8–11 However, trial participants are a research volunteer population, and outcomes in the trial context may not generalize to screening delivered as part of a population-based programme. This study therefore examined patient satisfaction, and measures of health and wellbeing in a ‘demonstration’ project in which FS screening was offered to all eligible adults in an ethnically and socioeconomically diverse area of London, England. 12
Methods
Participants and Procedures
The demonstration project was carried out between November 2006 and May 2008 in two ethnically diverse North London boroughs. General Practices (n = 34) from areas spanning a wide range of socioeconomic status based on the Index of Multiple Deprivation (IMD) 13 were invited to participate. All men and women aged 58–59 (n = 2260) registered with the Practices were sent an invitation to FS screening. Invitation recipients were asked to contact the screening clinic to discuss their suitability for the test if they had one of following conditions: bowel cancer, any inflammatory bowel disease, kidney failure (on dialysis), artificial heart valve, taking warfarin, recent heart attack (last 6 months), awaiting heart surgery or coronary angioplasty, any other serious illness, any bowel examinations in the last 3 years. Ethical approval was obtained from the local National Health Service Research Ethics Committee.
Invitations were sent six weeks before the screening appointment with the request to confirm, decline or change the appointment. Information about the test and a prescreening questionnaire were included. After two weeks, non-responders were sent a reminder and another questionnaire. A week before the appointment, patients were sent an enema to self-administer an hour before leaving home for the FS test.
FS was performed with a standard 140 cm Olympus colonoscope without sedation. The aim was to reach the junction of the sigmoid and descending colon without causing undue pain or distress. Carbon dioxide was used to insufflate the bowel.
Those who attended and underwent the test were asked to complete a brief questionnaire the morning after the test asking about their experiences. A follow-up questionnaire was mailed after three months to allow time for any further procedures (e.g. colonoscopy) to be completed.
Measures
Demographic Variables
Age, gender and home address were obtained from GP records. Individual socioeconomic status was indexed using IMD rank for the home address, and categorized into quintiles. The prescreening survey included ethnicity items from the UK Census, 14 but due to the large number of different ethnic subgroups and the small number within each group, responses were recoded into non-white versus white for analysis.
Screening Outcome
Screening outcome was recorded by the endoscopist: no polyps; ‘low-risk’ polyps; ‘high-risk’ polyps, with low-risk polyps removed and patients discharged. Patients with ‘high-risk’ polyps (categorized following British Society of Gastroenterology guidelines which included any of: three or more adenomas; diameter 1 cm or larger; tubulovillous or villous histology; severe dysplastia or malignancy) were referred to colonoscopy. All polyps removed during screening and colonoscopy were sent for histological analysis.
Experience of the Test (Morning-After Questionnaire)
Experience of pain was recorded with two questions: ‘How much pain did you feel during the test?’ (none/mild/quite a lot/severe) and ‘Was the test more painful or less painful than expected’ (less painful/about the same/more painful). Side-effects were assessed with the question: ‘Did you have any of the following after the test’: abdominal pains/cramps, nausea/vomiting, faint feeling or dizziness, wind, bottom soreness, soiling, sleep disturbance (none/mild/moderate/severe). A final open-ended question asked: Do you have any other comments about any aspect of the test’. Responses were coded as positive, negative, neutral and both positive and negative by two independent coders (KR and SHL), with a kappa inter-rater reliability of 0.87.
Satisfaction (Three-Month Follow-Up)
Satisfaction with the procedure overall was assessed with two items: ‘On balance, were you glad you had the test’ (yes/no/not sure) and ‘If a friend asked you if they should have the test, would you encourage or discourage them’ (strongly encourage/encourage/neither/discourage/strongly discourage). Satisfaction with individual elements of the test was assessed with four items: ‘How satisfied were you with…’ (a) ‘the information you were given before your test’; (b) ‘the facilities at the unit’; (c) ‘the attitude of the staff’; and (d) ‘the way the results of the test were explained’; with response options of: very satisfied, satisfied, dissatisfied and very dissatisfied.
Health and Wellbeing From Prescreening to Follow-Up
Colorectal symptoms were assessed in both prescreening and three-month follow-up questionnaires. Prescreening, the stem of the question read: ‘Because we are studying bowel screening, we would like to know how often people get these bowel symptoms. In the last three months have you …’. At follow-up, the stem was: Because you ve recently had the Flexi-Scope Test we would like to know how often you've had these bowel symptoms and bowel problems. Since you had the test have you…’. Symptoms listed were: ‘constipated’, ‘haemorrhoids (piles)’, ‘diarrhoea’, ‘wind’, ‘pains in the abdomen (gut)’, ‘bowel incontinence’ and ‘blood in your stools’ (no/occasionally/frequently). A symptom score was created as the sum of the items reported as having occurred occasionally’ or frequently’ (range: 0–7). 10
Self-rated health was assessed before screening and at follow-up with ‘Would you say that for someone of your age your own health in general is… (excellent/good/fair/poor). This has been shown to be valid in middle-aged adults. 15 For analysis, responses were recoded into excellent/good vs. fair/poor.
Anxiety was assessed before screening and at follow-up with a 4-item version of the Spielberger State Anxiety Inventory.16,17 People are asked how they feel right now’, with the following items: ‘I feel calm’, ‘I am tense’, ‘I feel upset’ and ‘I am relaxed’ (not at all/somewhat/moderately/very much). Scores were multiplied by 20 to be comparable with the full STAI (range: 20–80), and a cut-off of 44 was used to indicate clinical levels of anxiety. 18
Statistical Analysis
Because data were skewed, non-parametric methods were used. We tested for differences in pain, side-effects, and satisfaction by demographic characteristics (gender, area-level deprivation, ethnicity) and screening results using the Mann-Whitney U test (two groups) and the Kruskal-Wallis test (three or more groups); using a P value of < 0.01 because of multiple testing. Among respondents who completed both prescreening and follow-up questionnaires, we examined change using Wilcoxon signed-rank. Data were analysed using SPSS version 17.
Results
Sample Characteristics
Of 2260 people sent the screening invitation, 244 were ineligible and 1024 (51% of the eligible sample) attended. 12 Two patients were found to have cancer and were excluded from analyses, and two others attended but were unable to undergo the test due to poor bowel preparation; it is not known why the test was not rescheduled. Of the remaining 1020 people screened, 751 (74%) had returned the prescreening questionnaire, 913 (90%) completed the morning-after questionnaire and 674 (66%) returned the three-month follow-up questionnaire. There were no differences in questionnaire response rates by gender, deprivation or screening outcome.
Pain And Experience of Side-Effects
Of the 913 participants returning the morning-after questionnaire, 87% reported no pain or mild pain during the test, and less than 1% described the pain as severe (Table 1). The procedure was less painful than expected for 51% of respondents and more painful for 14%. Fewer women than men reported only none or mild pain (81% versus 93%; z = -5.35, P < 0.001), and more women than men found it more painful than they expected (18% versus 9%; z = – 3.36, P = 0.001). There were no differences by ethnicity or deprivation.
Flexible sigmoidoscopy (FS) screening attenders’ (n = 1020) response to the morning-after questionnaire
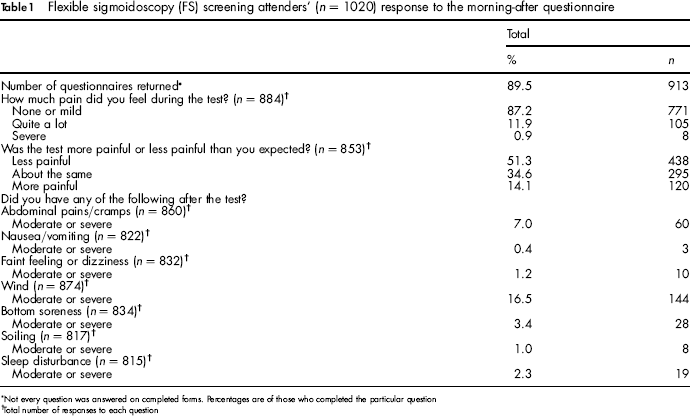
Not every question was answered on completed forms. Percentages are of those who completed the particular question
Total number of responses to each question
The most common side-effect to reach moderate/severe levels was wind (16%), with abdominal pains and cramps the next most commonly reported (7%). Less than 4% of respondents experienced moderate/severe levels of any other side-effect. Women reported abdominal pain more often than men (10% versus 4%; z = – 3.96, P < 0.001) but there were no other gender differences, and no differences by ethnicity or deprivation.
Participants’ Responses to ‘Any Other Comments’
In total, 482 participants of the 913 returning the morning-after questionnaire made written responses to the open-ended question. Responses were predominantly positive (74%) with 15% coded as positive and negative, 8% as negative and 3% as neutral. Illustrative quotes are presented in Box 1.
Illustrative quotes from the questionnaire completed the morning after FS coded as positive, positive and negative, negative and neutral
Positive
‘I was very happy by how easy it all was and how little time the test took. Thank you.’ Male, White British, most deprived IMD quintile.
‘Communication and explanation by the staff made me feel very relaxed. Procedure was performed very gently as well. I had three polyps removed, did not feel a thing.’ Female, Indian, third most deprived IMD quintile.
‘Very quick and efficient. Did not take as long as anticipated. Staff very friendly and helpful and reassuring. Interesting to see pictures of my colon – a first for me!’ Female, White British, second most deprived IMD quintile.
Positive and negative
‘I found the procedure very painful however I was relieved that the test was negative.’ Female, Caribbean, third most deprived IMD quintile. Prior to the test I was scared, but the staff were very sympathetic and helpful to calm down my anxiety and [feelings of discomfort]. I [had] this test to avoid any unforeseen problems.’ Female, Pakistani, most deprived IMD quintile.
Negative
‘The preparation [enema] at home before the test made me feel uncomfortable.’ Male, White British, third most deprived IMD quintile. When discussing patients’ results I believe this should be done in private not in front of other patients as this can be disconcerting to patients.’ Male, White British, most affluent IMD quintile.
Neutral
‘This test should be carried out once every 18 months’ Male, Caribbean, second most deprived IMD quintile ‘I felt like passing wind during the test not after. [The] next day my first motion was loose.’ Male, Indian, third most deprived IMD quintile.
Satisfaction (3-Month Follow-Up)
Satisfaction with the flexible sigmoidoscopy test was very high at follow-up (Table 2), with almost all (98%) respondents glad they had the test, while 97% would strongly encourage a friend to have it. Satisfaction with specific aspects of the procedure was also very high, with responses of ‘satisfied’ or ‘very satisfied’ reported by 98% for the prescreening information, 97% for the facilities, 99% with the attitude of the staff and 98% with how the test results had been explained. There were no significant differences by gender, deprivation or ethnicity.
Flexible sigmoidoscopy (FS) screening attenders’ (n = 1020) response to satisfaction measures three months after FS
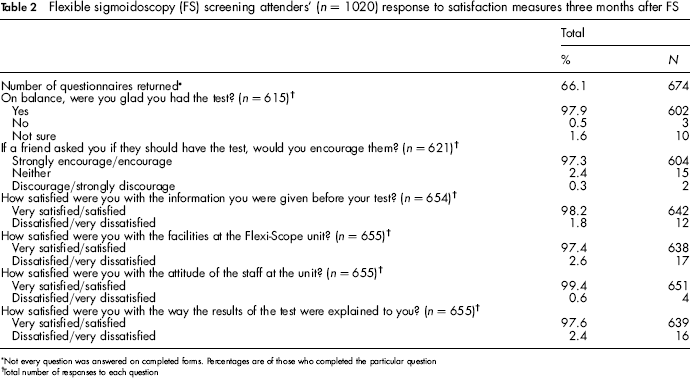
Not every question was answered on completed forms. Percentages are of those who completed the particular question
Total number of responses to each question
Patient-Reported Outcomes By Screening Result
Seventy-five percent of participants had a negative result, 19% had ‘low risk’ polyps requiring no further investigation, and 5% had ‘high risk’ polyps and were referred for colonoscopy. There were no differences in satisfaction, pain or side-effects by screening outcome.
Changes In Health And Wellbeing From Prescreening to Follow-Up
We examined change in number of colorectal symptoms, self-reported health and anxiety among participants (n = 534, 52%) who returned both the prescreening and follow-up questionnaires. There were no differences on prescreening scores among those who did and did not complete follow-up.
On average, respondents reported 0.81 fewer colorectal symptoms at the three-month follow-up than prescreening (Table 3). No significant changes were found for anxiety or self-reported health. Results did not differ by gender, deprivation, ethnicity or screening outcome.
Changes in colorectal symptoms, general health and anxiety from before to three months after screening among respondents to both questionnaires (n = 534)

Total number of responses to both questions
Discussion
The results of this study indicate that the acceptability of population-based FS screening, delivered in a similar manner to the UK's population-based national screening programme, was extremely high. Patient-reported outcomes were strikingly comparable with those found in the gastroenterologist-led UK FS Trial, which invited only individuals who had indicated they were interested in taking part in the Trial.8–10
Overall, 98% of participants were glad they had the test and 97% would encourage a friend to have it. Half the participants (51%) found FS less painful than they expected and less than 1% reported severe pain. Side-effects were minimal, and the most common, wind, reported by only 16%.
There were few demographic differences, but women reported more abdominal pain following the procedure which is consistent with previous work. 19 Strategies to address pain, particularly in women, could help improve FS screening programmes. It was reassuring that no detrimental differences were found by deprivation or ethnicity, and based on these results, participant experience is unlikely to drive inequalities in uptake. 7
We found no evidence that self-reported health or anxiety changed from before to three months after the test, and colorectal symptoms declined. Results were similar for patients with or without polyps, suggesting that the impact of polyp removal on wellbeing was minimal. This is consistent with findings from the gastroenterologist-led UK FS Trial, with the sole difference being a reduction in anxiety in the previous study. 10
It is possible that the high patient satisfaction could be partly attributed to staff attitude and behaviour, which can be difficult to regulate in a nationwide programme. In this demonstration pilot, screening was delivered by experienced nurse endoscopists who were well-trained to practice in the screening setting as documented in a previous qualitative study. 20 Staff training is important given the differences in screening and diagnostic services. Using PROMs as part of ongoing audit of services once FS screening is implemented nationally would make it possible both to assess service characteristics and to give feedback to screening centres. A further limitation is that the satisfaction results are based on the 66% of FS screening participants completing the follow-up questionnaire. However, follow-up responders did not differ from non-responders on any of the available demographic characteristics (gender, area-level deprivation). Comparing the findings with the potentially more motivated UK FS Trial participants, where 94% returned the follow-up questionnaire, satisfaction levels only differed slightly. This suggests that these positive results may generalize to the screening eligible population in a national FS programme.
Conclusion
Patient-reported outcomes indicate high acceptability of flexible sigmoidoscopy screening delivered by specialist nurse endoscopists in a socioeconomically and ethnically diverse community sample. Screening had no adverse impact on colorectal symptoms, self-reported health or anxiety.
Footnotes
Funding from the Department of Health and Cancer Research UK is gratefully acknowledged.