
Abstract
Objectives
To estimate improvements to four antenatal screening tests for Down's syndrome (first trimester Combined, second trimester Quadruple, and first and second trimester Integrated and Serum Integrated tests) based on adding ductus venosus pulsatility index (DVPI), fetal nasal bone examination (NBE) and serum placental growth factor (PlGF).
Setting
Statistical analysis of data from several sources modelled using the maternal age distribution of live births in England and Wales from 2006 to 2008.
Methods
Monte Carlo simulation carried out to estimate the screening performance of tests with the addition of combinations of DVPI, NBE and PlGF.
Results
At a 95% detection rate (DR), with first trimester markers measured at 11 completed weeks’ gestation, the addition of DVPI, NBE and PlGF decreased the false-positive rate (FPR) of the Combined test from 16.1% to 3.0%, the addition of PlGF to the Quadruple test decreased the FPR from 15.7% to 15.3%, the addition of DVPI, NBE and PlGF to the Integrated test decreased the FPR from 4.1% to 0.6% and the addition of PlGF to the Serum Integrated test decreased the FPR from 15.1% to 11.1%. At a 90% detection rate, the reductions in the FPR were from 6.8% to 0.8%, 7.7% to 7.4%, 1.2% to 0.1% and 6.2% to 4.8%, respectively.
Conclusions
The addition of DVPI, NBE and PlGF to the Combined and Integrated tests significantly improves screening performance, reducing the FPRs by over 80%. The Integrated test with DVPI, NBE and PlGF is significantly better than the Combined test with DVPI, NBE and PlGF.
INTRODUCTION
Over the last decade there have been incremental improvements in the performance of antenatal screening for Down's syndrome, based on the use of ultrasound and serum markers in combination with maternal age. These improvements have enhanced the performance of screening tests: the first trimester Combined test (nuchal translucency [NT], free β- or total human chorionic gonadotrophin [hCG] and pregnancy associated plasma protein A [PAPP-A] with maternal age), the second trimester Quadruple test (alphafetoprotein [AFP] unconjugated estriol [uE3], free β- or total hCG and inhibin-A with maternal age), the Integrated test (first trimester NT and PAPP-A, and second trimester AFP, uE3, free β- or total hCG and inhibin-A with maternal age) and the Serum Integrated test (Integrated test without NT) tests based on markers in both trimesters. For example, ductus venosus pulsality index (DVPI) 1 and fetal nasal bone examination (NBE) 2 have become more common, and placental growth factor (PlGF) is recognized as a useful additional screening marker. 3 The precision of NT measurement has increased. 4
An indication from the Wolfson Institute (London, UK) screening service that the standard deviation of Inhibin-A has decreased over time required a review of the relevant distribution parameters in the screening algorithm. These developments prompted us to provide an updated summary of screening performance of the screening tests with and without the addition of DVPI, NBE and PlGF and compare estimates with those relating to the newer methods of screening based on sequencing DNA in maternal plasma.
METHODS
We used marker distribution parameters for NT, hCG, PAPP-A, AFP, uE3 and inhibin-A from the Serum Urine and Ultrasound Screening Study (SURUSS) which included 98 Down's syndrome pregnancies, 5,6 incorporating improvements based on the use of gestation-specific NT median multiple of the median (MoM) values in Down's syndrome pregnancies 7 and the reduced standard deviation of NT over time. 4 Distribution parameters for DVPI were taken from Borrell et al. 1 (66 Down's syndrome pregnancies), parameters for NBE from Cicero et al. 2 (333 Down's syndrome pregnancies) and parameters for PlGF from Wald et al. 3 (532 Down's syndrome pregnancies). Revised standard deviations of inhibin-A were derived from 223 Down's syndrome pregnancies and 146,966 unaffected pregnancies screened using the Wolfson Institute screening service between 2003 and 2011.
Monte Carlo simulation was used to simulate 500,000 Down's syndrome and 500,000 unaffected pregnancies to estimate screening performance. Each simulated pregnancy was assigned a maternal age based on the distribution of maternities in England and Wales from 2006 to 2008 inclusive (the latest available at the time the study was performed) 8 and the maternal age-specific odds of an affected livebirth. 9–11 For each simulated pregnancy, the risk of being affected with Down's syndrome in the early second trimester was calculated by multiplying the maternal age-specific odds of having an affected live birth (adjusted to early second trimester by multiplying by 1/0.77 to allow for the general fetal loss in Down's syndrome pregnancies from this time in pregnancy until term 12 ) by the likelihood ratio for being affected (for the simulated set of marker values) which was calculated from the multivariate Gaussian distributions of marker levels in affected and unaffected pregnancies. Each simulated pregnancy was classified as screen positive if the resulting risk estimate was greater than or equal to a specified cut-off level. First trimester PlGF was used with the Combined, Integrated and serum Integrated tests; second trimester PlGF with the Quadruple test. NBE (present or absent) depends on the NT measurement, and the method of incorporating it into the algorithm is given in Appendix A (Statistical appendix). NBE was assumed to be independent of DVPI. While it is unlikely to be completely independent because DVPI and NBE are not completely independent of NT, it is not likely to be strong enough to have a material effect on screening performance.
Estimates of screening performance were specified as: the detection rate (the proportion of affected pregnancies with a positive result) for a specified false-positive rate (the proportion of unaffected pregnancies with a positive result), and the false-positive rate for a specified detection rate. The detection and false-positive rates for a specified risk cut-off, and the corresponding odds of being affected given a positive result were also estimated.
The distribution parameters used in estimating screening performance are given in Appendix B (Distribution parameters). Previously published parameters (referenced in Appendix Tables B1–B4) were used, except for (i) standard deviation of inhibin-A and (ii) AFP truncation limits. (i) The standard deviation of inhibin-A in affected pregnancies was 0.2213 (smaller than 0.2679 in SURUSS 5 ) and in unaffected pregnancies was 0.1779 (0.2078 in SURUSS 5 ); the tighter standard deviations had little effect on correlations between Inhibin-A and the other markers. (ii) Because of the strong influence on the risk of having a Down's syndrome pregnancy of very high or low AFP MoM values (that still fell within published truncation limits), and after further examination of the probability plot for AFP in the SURUSS report, 5 the truncation limits for AFP were narrowed to 0.5–2.5 (instead of 0.4–3.0).
The paper presents results based on free beta human chorionic gonadotropin (β-hCG) as the hCG marker. Appendix C (Results using total hCG as the hCG marker) gives the corresponding Appendix Figures C1–C5 and Appendix Tables C1–C6 for total hCG as the hCG marker.
RESULTS
Detection rates for specified false-positive rates and false-positive rates for specified detection rates for the Combined, Integrated, serum integrated and Quadruple tests with and without the addition of first trimester measurements of ductus venosus pulsatility index (DVPI), nasal bone examination (NBE) and placental growth factor (PlGF) First trimester markers measured at 11 completed weeks
Tests ranked according to detection rate for a 2% false-positive rate
DR, detection rate; FPR, false-positive rate *PlGF measured in early second trimester
Detection rates for specified false-positive rates and false-positive rates for specified detection rates for the Combined, Integrated, serum integrated and Quadruple tests with and without the addition of first trimester measurements of ductus venosus pulsatility index (DVPI), nasal bone examination (NBE) and placental growth factor (PlGF) First trimester markers measured at 12 completed weeks
Tests ranked according to detection rate for a 2% false-positive rate
DR, detection rate; FPR, false-positive rate *PlGF measured in early second trimester
Detection rates for specified false-positive rates and false-positive rates for specified detection rates for the Combined, Integrated, serum integrated and Quadruple tests with and without the addition of first trimester measurements of ductus venosus pulsatility index (DVPI), nasal bone examination (NBE) and placental growth factor (PlGF) First trimester markers measured at 13 completed weeks
Tests ranked according to detection rate for a 2% false-positive rate
DR, detection rate; FPR, false-positive rate *PlGF measured in early second trimester
Figure 1 shows a plot of the
false-positive rate against the detection rate for the four screening tests (first
trimester markers measured at 11 completed weeks’ gestation for the tests that use first
trimester markers). The screening performance of the Integrated test is substantially
better than that of the Combined and serum Integrated tests. The latter are, in turn,
substantially better than the Quadruple test. For example, Figure 1 and Table 1 show that at an 85% detection rate the Quadruple test has a 4.4%
false-positive rate compared with 3.3% using the Combined test, 3.0% using the serum
Integrated test and 0.4% using the Integrated test. At a 90% detection rate the
corresponding false-positive rates are 7.7% (Quadruple test), 6.8% (Combined test), 5.4%
(Serum Integrated test) and 1.2% (Integrated test). At a 95% detection rate, the
corresponding false-positive rates are 15.7%, 16.1%, 12.4% and 4.1%, respectively. With
the first trimester measurements performed at 12 and 13 weeks instead of 11 weeks,
screening performance is reduced (Tables 2 and 3). Detection rate plotted against false-positive rate for the Combined (CT),
Quadruple (QT), serum integrated (SIT) and Integrated (IT) tests (first
trimester markers measured at 11 completed weeks)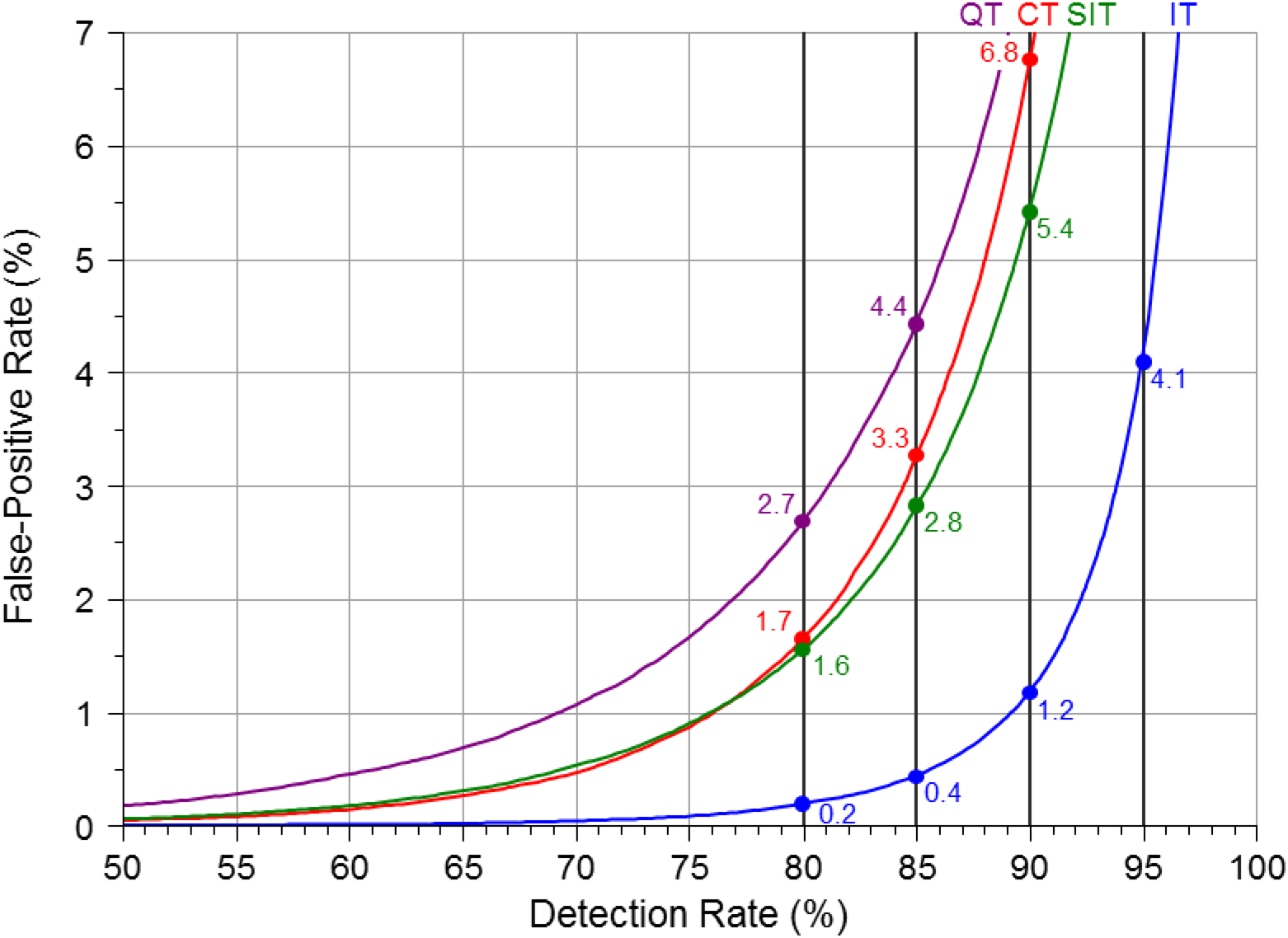
Figure 2 shows the screening performance
of the Combined test and the Integrated test with and without DVPI, NBE and with both
(with the first trimester markers measured at 11 weeks). The addition of NBE and DVPI
improves screening performance. For example, the Integrated test achieves a 95%
detection rate for a 0.7% false-positive rate, a much lower false-positive rate than
with any of the other test options. With the first trimester measurements performed at
12 and 13 weeks instead of 11 weeks, screening performance is reduced (Tables 2 and 3). Detection rate plotted against false-positive rate for the Combined (CT) and
Integrated (IT) tests without (dashed lines) and with (solid lines) first
trimester measurement of ductus venosus pulsatility index (DVPI), nasal bone
examination (NBE) or both (first trimester markers measured at 11 completed
weeks)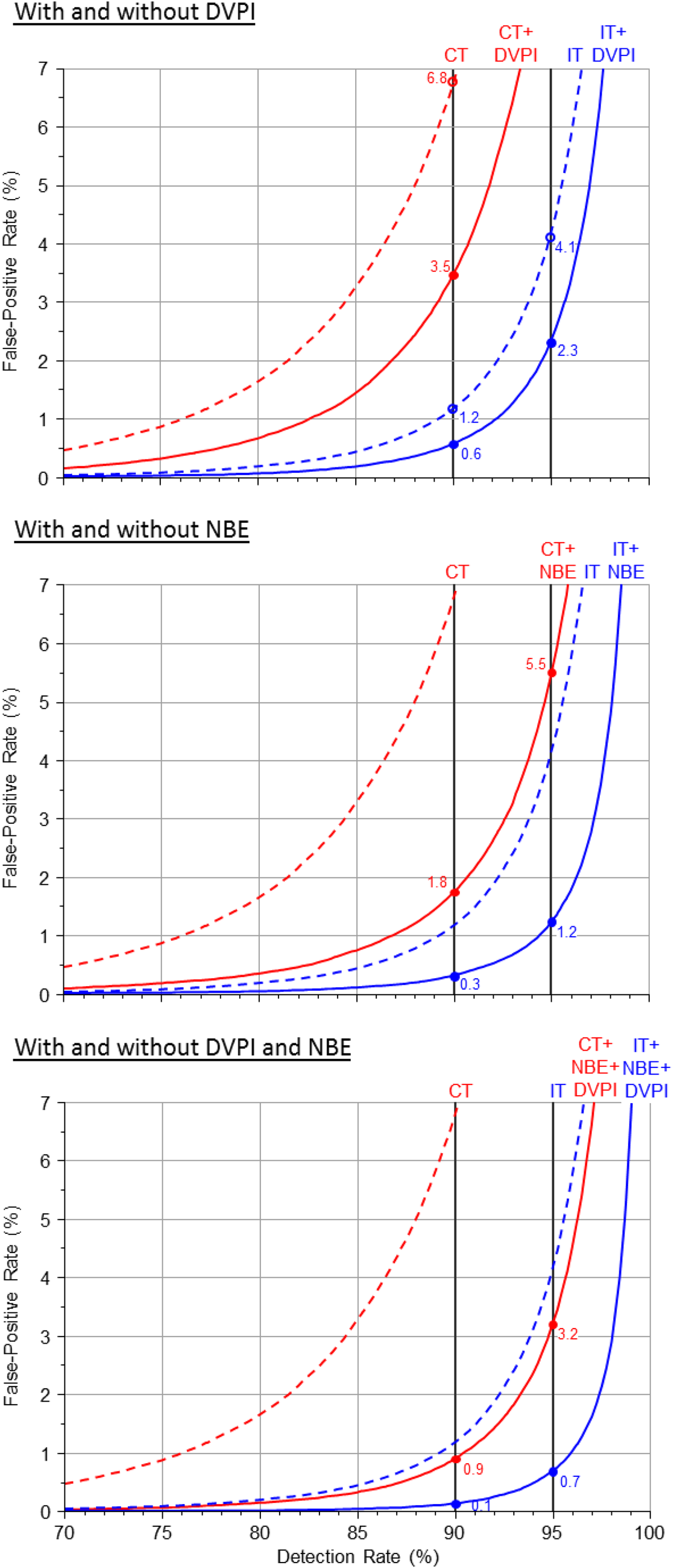
Figure 3 shows the screening performance
of the Integrated and Combined tests and the serum Integrated test with and without
first trimester PlGF according to the week (11 or 13) when the first trimester
measurements are performed. PlGF improves screening performance more at 13 weeks than 11
weeks. For example at a 95% detection rate the Integrated test improvement with first
trimester measurements at 11 weeks is a 0.4 percentage point reduction in the
false-positive rate (3.7% versus 4.1%) but with their measurement at 13 weeks it is a
4.2 percentage point reduction (3.3% versus 7.5% [see Table 3]). Detection rate plotted against false-positive rate for the Combined (CT), serum
integrated (SIT) and Integrated (IT) tests without (dashed lines) and with
(solid lines) first trimester measurement of placental growth factor (PlGF)
according to completed week of first trimester marker measurements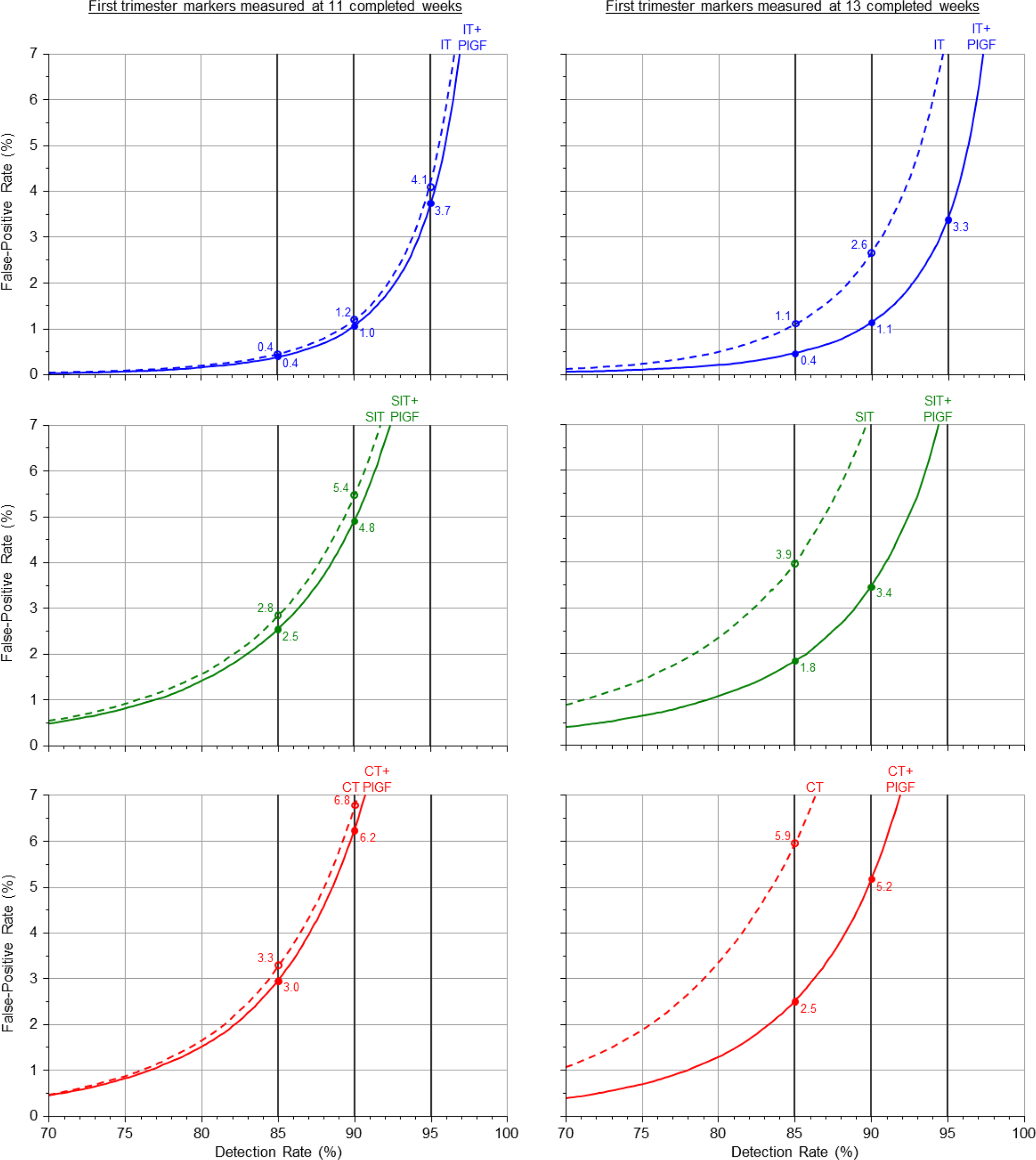
With the second trimester Quadruple test there is a small improvement in screening performance with the addition of second trimester PlGF, namely a 0.2 percentage point reduction in the false-positive rate (4.2% versus 4.4% for an 85% detection rate; see Table 1).
Figure 4 shows the screening performance
of the four tests with the addition of NBE, DVPI and PlGF to the Combined and Integrated
tests and PlGF to the Quadruple and serum Integrated test, again with first trimester
measurements at 11 weeks. The three additional markers substantially improve screening
performance for the Combined and Integrated tests. For example, at a 95% detection rate
the false-positive rate using the Combined test is 3.0% compared with 16.1% without the
three extra markers, and 0.6% compared with 4.1% with the Integrated test. Detection rate plotted against false-positive rate for the Combined (CT) and
Integrated (IT) tests with the addition of first trimester ductus venosus
pulsatility index (DVPI), nasal bone examination (NBE) and placental growth
factor (PlGF), the serum integrated test (SIT) with the addition of second
trimester PlGF and the Quadruple test (QT) with the addition of second
trimester PlGF (first trimester markers measured at 11 completed weeks)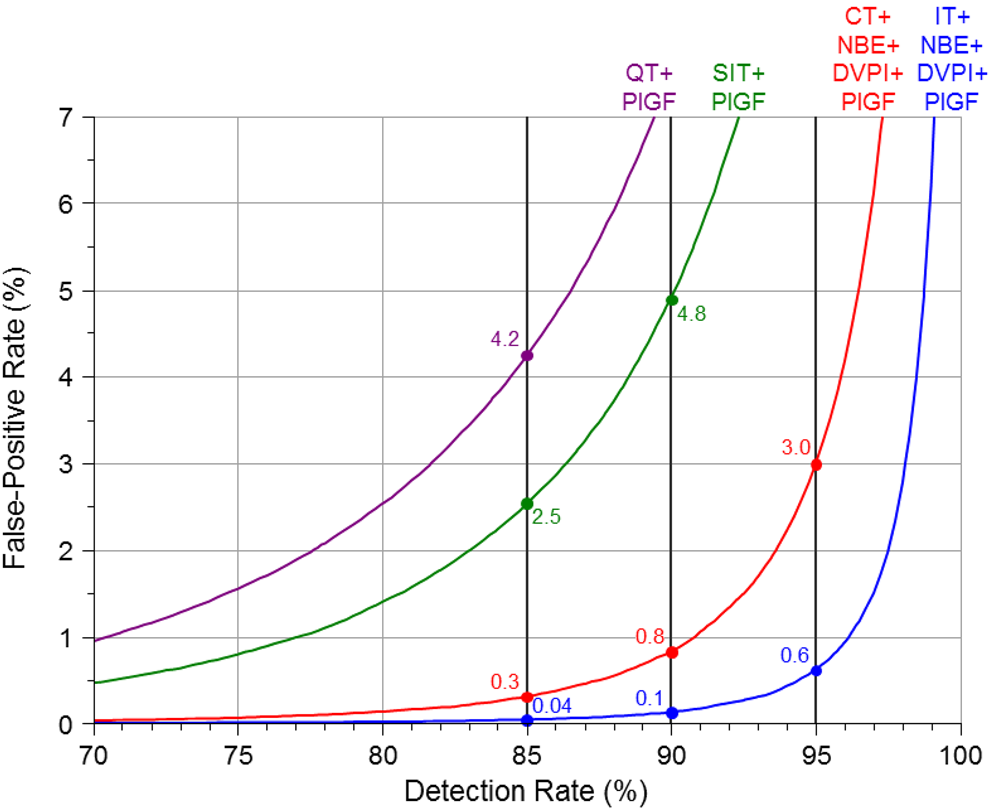
Figure 5 shows the overlapping
distributions of risk of having a Down's syndrome pregnancy in affected and unaffected
pregnancies for the Combined and Integrated tests with and without the addition of DVPI,
NBE and PlGF (first trimester measurements at 11 completed weeks’ gestation). For the
Combined test the median risk in affected pregnancies is 1:3 and 1:7800 in unaffected
pregnancies. With the addition of DVPI, NBE and PlGF the median risks are 3:1 and
1:49,000 respectively. For the Integrated test the median risk in affected pregnancies
is 4:1 and 1:32,000 in unaffected pregnancies. With the addition of DVPI, NBE and PlGF
the median risks are 42:1 and 1:230,000 respectively. Distributions of risk of a Down's syndrome pregnancy in affected and unaffected
pregnancies for the Combined and Integrated tests with and without first
trimester ductus venosus pulsatility index (DVPI), nasal bone examination (NBE)
and placental growth factor (PlGF). First trimester markers measured at 11
completed weeks' gestation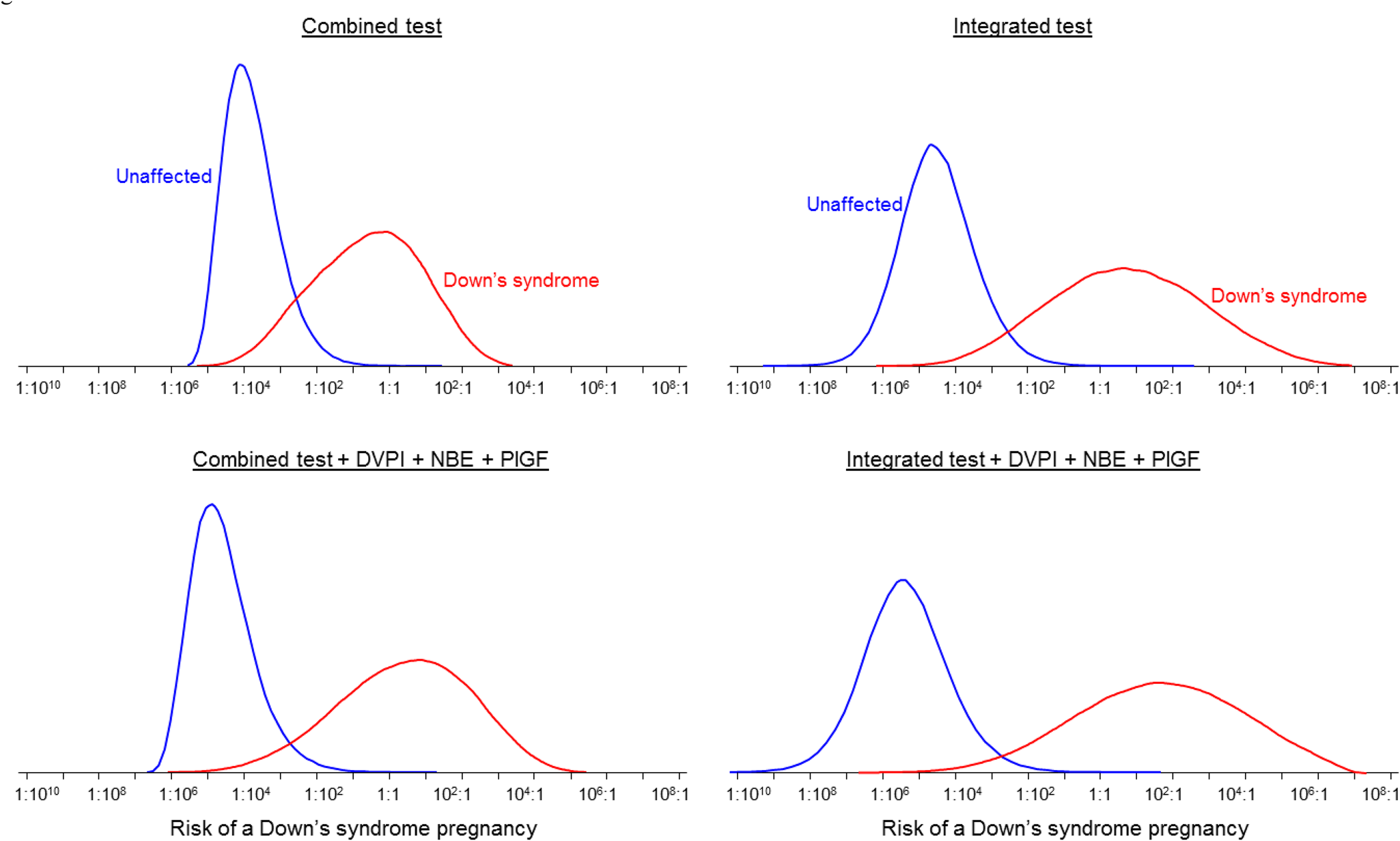
DISCUSSION
Our results show that the addition of DVPI, NBE and PlGF significantly improves the screening performance of the Combined and Integrated tests, with false-positive rates about 80% lower for the same detection rate. The Integrated test achieves significantly improved screening performance compared with the Combined test, and the Integrated test with DVPI, NBE and PlGF achieves significantly improved screening performance compared with the Combined test with DVPI, NBE and PlGF. The Integrated test without the addition of the three markers has a false-positive rate about five times lower than the Combined test for the same 90% detection rate (1.2% versus 6.8%). Similarly with the three additional markers the Integrated test has a false-positive rate five times lower than the Combined test for the same 95% detection rate (3.0% versus 0.6%).
The incremental benefits of adding NBE and DVPI measurements are useful. In experienced hands these measurements can usually be performed within 5–10 minutes, at the same time as an NT measurement. 13,14 The cost of the ultrasound component of the Combined or Integrated tests is enormously variable between centres, but the additional cost of measuring NBE and DVPI in the same ultrasound examination used for NT measurement should not be great. PlGF is of little value at about 11 weeks’ gestation, but is useful in those pregnancies seen later in the first trimester, and the contribution to the overall cost of testing is relatively small.
These estimates of screening performance are close to those recently reported for maternal plasma DNA sequencing methods. These can achieve detection rates of about 98% or more with false-positive rates of about 0.2% or less with test failure rates between 3% and 7%. 15–17 At present, the main concern with DNA testing is this failure rate, the cost of the test and the need to send samples to specialist DNA sequencing laboratories. If a DNA result is not available, the pregnancy would either have to be regarded as screen-positive, and an amniocentesis offered, or screen-negative, and an amniocentesis not offered. If regarded as screen-positive, the overall false-positive rate would be about 3.2% or more. For the same 98% detection rate, the false-positive rate of the Integrated test with DVPI, NBE and PlGF is 2.7% (Table 1). Screening using biochemistry, ultrasound and maternal age may also lack one or two markers (e.g. a nasal bone result), but unlike DNA testing, a result can still be given based on markers for which results are available, and such occasional missing data have little effect on overall screening performance.
So, while screening performance with non-DNA methods is less than that reported for DNA methods, the difference is small and the method of choice uncertain. Comparisons between non-DNA screening methods and DNA methods need to take account of several factors, including cost, simplicity and provision of other clinical information that might be of relevance to the pregnancy, such as screening for pre-eclampsia. It would be useful if DNA sequencing screening methods were introduced in selected centres together with the best available non-DNA methods so that experience and data with both methods are gained in the same pregnancies to compare their screening performance, cost, ease of use and incidental clinical benefits in the same women.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.