
Abstract
Belgium’s first euthanasia criminal trial was decided in 2020. Existing studies identify the implications of this trial for euthanasia provision for patients with mental disorder, but its broader influences have not been explored. We conducted semi-structured interviews with 14 health professionals who provide euthanasia in Belgium. We constructed themes describing the trial’s practitioner-level and system-level influences. These are (1) the trial prompted fear, insecurity, and a degree of reluctance to provide; (2) some providers adapted their euthanasia decision-making; (3) the trial exposed deficiencies with the Act; (4) the trial clarified some legal requirements; (5) added burdens were placed on health service providers owing to the ‘chilling effect’ of the trial on practice; and (6) the trial prompted changes to the euthanasia regulatory landscape. Participants reported that the trial has significantly influenced euthanasia practice including patient access and practitioner participation. Measures are needed to address these implications if they persist.
Introduction
In 2020, three physicians who were involved in assessing a patient for euthanasia were tried for murder by poisoning or cooperating in poisoning under the Belgian Penal Code. It was alleged that they had failed to comply with the requirements of the Belgian Act on Euthanasia of 2002 (the ‘Act’) when providing euthanasia for the patient, Tine Nys (‘TN’). TN was a 38-year-old woman with a long-standing history of mental illness and a diagnosis of Borderline Personality Disorder. 1 Her request for euthanasia was on the basis of mental disorder as the sole or underlying medical condition: this is legal in Belgium provided all the ‘due care’ criteria are met. 2 Although euthanasia was administered in 2010, it was not until 2019 that the physicians involved, two general practitioners and one psychiatrist, were formally accused. In January 2020, the judgement acquitting the three physicians was delivered by the Court of Assizes in Ghent, Flanders, the highest Belgian trial court with criminal jurisdiction.
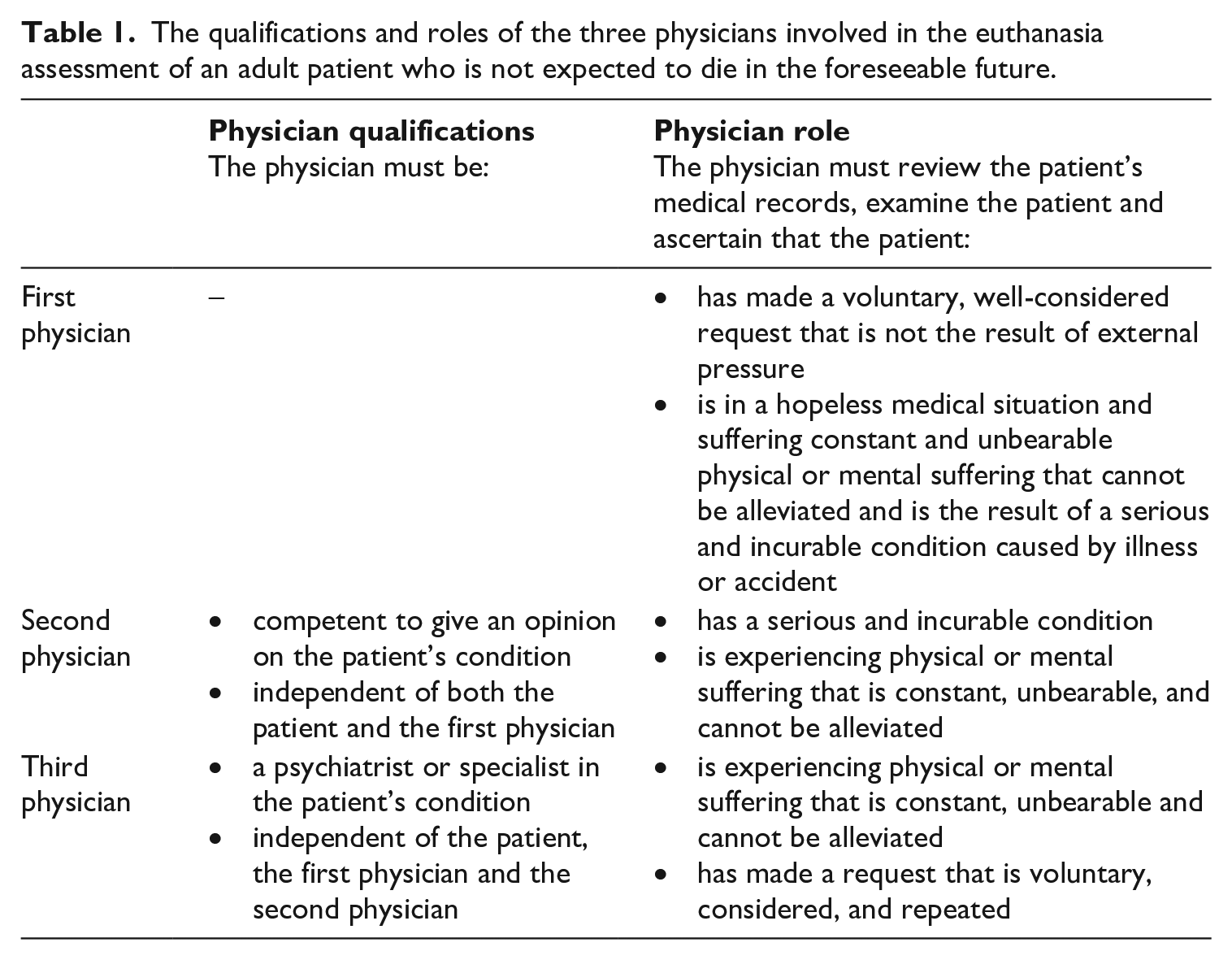
For patients whose request for euthanasia is based on diagnosed mental disorder as the sole or underlying illness (‘patients with mental disorder’), at least three physicians must assess the patient’s eligibility. 3 However, the assessments of the second and third physicians are not binding on the first physician’s decision. The requisite qualifications and roles of each physician is presented in Table 1. A minimum 1-month waiting period must be observed between the patient’s written request and the administration of the life-ending medication. All cases of euthanasia must be reported to the national oversight body, the Federal Control and Evaluation Commission on Euthanasia (‘FCECE’) within 4 working days. The FCECE can refer cases to the public prosecutor if it suspects non-compliance with the Act. 4
The qualifications and roles of the three physicians involved in the euthanasia assessment of an adult patient who is not expected to die in the foreseeable future.
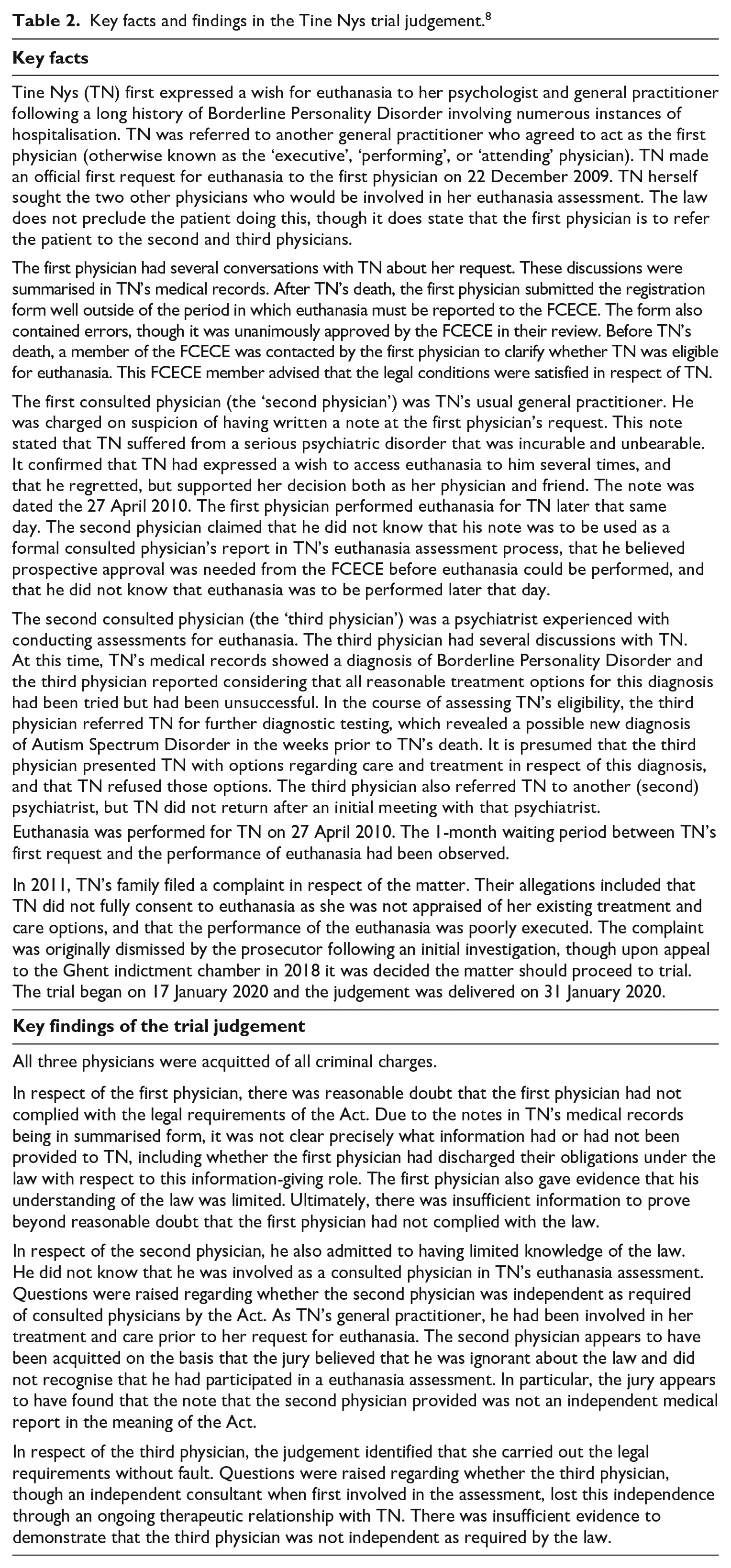
Detailed descriptions of the TN criminal trial (the ‘trial’) are provided elsewhere. 5 Table 2 provides a summary of the key facts and findings. The trial received significant attention in the Belgian media. 6 This was the first time physicians had been tried for alleged breaches of the Act. Prior to this, one other case had been referred for prosecution, though it was not ultimately prosecuted. 7
Key facts and findings in the Tine Nys trial judgement. 8
The trial has received limited attention in the literature. Some research identifies lessons from the trial to improve euthanasia assessments for patients with mental disorder. 9 Another study analyses the media coverage of the trial. 10 There has also been one qualitative interview study which explored the experiences of healthcare professionals and volunteers involved in providing euthanasia for patients with mental disorder. One article from this research identified that the trial caused legal uncertainty and a reticence among physicians to be involved in these assessments. This, in turn, contributed to an increased workload for end-of-life consultation centres, 11 with associated emotional and access-related burdens for patients. 12 The participants in that study also expressed uncertainty about the correct interpretation of the Act and reported considering altering their approach to assessments following the trial. Another article from this study found that mental healthcare workers considered the trial to reflect deficiencies with the Act. 13
Similar findings on the impact of prosecutions on euthanasia practice are reported in research from the Netherlands. The first prosecution of a physician in respect of the Dutch euthanasia law simultaneously frightened providers and clarified the legal requirements. In addition, it led to a decrease in willing providers and an increased number of requests made to the Dutch Centre for Euthanasia Expertise from both terminally ill and non-terminally ill patients. 14
This research employs regulatory theory as a useful lens for exploring this trial and its implications for practice. Regulatory theory focuses on identifying regulatory forces and exploring (empirically and otherwise) how they shape or steer the behaviour of regulated individuals. Recent regulatory empirical literature is also concerned with identifying the impacts or outcomes of regulation for behaviour and decision-making. 15 Regulatory theory suggests that legislation creates rules to control how euthanasia is practised. Criminal prosecutions are one way to formally enforce compliance with those rules. 16 Prosecutions seek to punish lawbreakers to prevent them from continuing to break the law and deter others from future law-breaking. 17 Prosecutions bring private behaviour into the public and political realms. Accordingly, they can expose and denounce conduct which does not align with the legal framework, and reinforce the authority and credibility of the criminal process. 18 In addition, prosecutions can seek to intimidate members of the targeted group and make them feel vulnerable to legal risks. 19 While these are the broad aims (and can be the consequences) of prosecutions, there may also be other outcomes, including those that may not be intended. For example, prosecutions can alienate previously law-abiding individuals if they perceive that the prosecution reflects a questioning of their willingness to comply with the legal framework. In such cases, they may attempt to avoid or thwart regulation by, for example, finding and exploiting loopholes. 20
In the healthcare context, criminal prosecutions might also foster ‘defensive medicine’. This refers to healthcare providers taking steps in their medical decision-making that are clinically unnecessary and that they would not normally take, but for the fact that they are now faced with the threat of legal action. These different or additional steps are taken by physicians to protect themselves from the risk of sanction. 21 Medical defensiveness, and the influential nature of prosecutions on physicians have been observed in US research on treatment decisions for terminally ill patients. One questionnaire study found that perceived vulnerability to legal sanction was one of the main reasons why respondents were reluctant to abate treatment for patients. In addition, though there had been just one prosecution for homicide in respect of abating treatment (which did not result in a conviction), some respondents incorrectly estimated that over 100 prosecutions for abating treatment had occurred. 22
This study seeks to advance existing evidence by examining the influence of the trial on individual health professionals’ euthanasia practice and on the euthanasia system. This includes an exploration of how the trial has affected euthanasia provision not only within the context of patients with mental disorder (the context of the prosecution) but also for patients seeking euthanasia generally. Regulatory theory is used to inform, but not limit, the investigation of these influences. As such, this study seeks to answer the research question: how has the first Belgian euthanasia criminal trial influenced providing health professionals’ euthanasia practice and the Belgian euthanasia system?
Methodology
This semi-structured interview study is part of a larger qualitative investigation into the nature and influence of euthanasia regulation in Belgium. 23 In this study, we adopt a critical realist approach. 24
Eligibility to participate and recruitment
Health professionals were eligible to participate if they were a physician or nurse who spoke English or Dutch and had been involved in the euthanasia assessment of at least two patients in the past year. We imposed this latter requirement to ensure participants had been involved in providing euthanasia recently, and since the trial, and to include both more and less experienced health professionals. Both physicians and nurses were included in the study as both are involved in providing euthanasia, though in different ways. Physicians alone can undertake eligibility assessments and administer the life-ending medication. However, nurses play an important role in exploring patients’ requests for euthanasia, supporting patients and physicians in the euthanasia assessment process, assisting with the administration of the life-ending medication, and in some cases, they participate in euthanasia decision-making. 25
We recruited participants through the professional networks of the research team, advertisements disseminated by relevant organisations, and snowball recruitment. We selected participants purposively to access health professionals with varied personal and professional backgrounds and to identify individuals who also held a role in regulating euthanasia (a ‘regulatory role’). 26 Participants’ informed consent to participate was obtained prior to the interview.
Data generation
We conducted interviews with eligible health professionals from September 2022 to March 2024 over Microsoft Teams. Some of the health professionals interviewed held a regulatory role such as being a current or former member of the FCECE or a professional association which has released guidelines on euthanasia.
Participants were able to indicate whether they would prefer to participate in Dutch, English or be supported to speak English. MA led the interviews in English (LW co-interviewed in several of these) and where the participant was supported to speak in English (KC and LD supported the participant to participate in English). KC led the interviews conducted in Dutch.
If the health professional also had a regulatory role in relation to euthanasia this was recorded as relevant to their ability to identify the influences of the trial on the euthanasia system.
We developed an interview guide which sought to lead the participant through the euthanasia process and identify how euthanasia regulation influences their behaviour and decision-making at each stage of the process (Supplementary File 1). 27 The interview guide contained an optional prompt which was: ‘how, if at all, have any court decisions impacted your decision-making about euthanasia?’ Insights that participants shared on the trial were explored further as they were centrally relevant to the overarching study which considered how euthanasia regulation influences health professionals’ euthanasia practice.
Interviews were recorded and transcribed verbatim in the language used in the interview. Participants were given the opportunity to review, edit, and add further reflections to their transcript. 28 The Dutch transcripts were then translated into English for analysis by a translator with experience conducting research on the topics of end-of-life and euthanasia.
Data analysis
MA preliminarily analysed 10 transcripts as part of the wider study on Belgian euthanasia regulation. During this preliminary analysis, the significance of the trial became apparent, with most although not all participants discussing it. All data pertaining to the trial was extracted, and a reflexive approach to thematic analysis, facilitated by NVivo software (QSR International, Release 1.6.1) was used. 29 This approach facilitated the inductive generation of semantic and latent themes based on participants’ lived experiences, reflecting the study’s exploratory research question and regulatory theoretical framework. 30 First, MA read this data in full and made notes to ensure data familiarisation. Second, MA read the data two further times simultaneously with coding. Throughout this process initial codes were generated, adapted, and removed. The interview guide was adapted after this preliminary analysis to ensure that all subsequent participants were specifically asked to share their insights on the trial.
The preliminary analysis of the 10 transcripts facilitated analysis of the remaining transcripts, which were coded following the same steps described above. In this process, codes generated in relation to the 10 transcripts analysed first were revised and adapted. Interviews for the overarching study (of which this study was a part) ceased when sufficient information power had been reached. 31 The authors made this determination reflecting the study’s specific research question and basis in regulatory theory, heterogenous selection of participants (including some participants with considerable knowledge of euthanasia regulation and the trial) and preliminary analysis.
Once all interviews were coded, MA generated themes which were adapted and ultimately settled following discussions within the research team. 32 Participant quotes are provided below to illustrate these themes. Some of these quotations have been modified slightly to reflect participants’ intended meaning in English and to preserve participant anonymity, but in so doing their meaning has not been altered.
Researcher reflexivity
MA maintained a reflexive journal throughout the coding and theme development processes. 33 The subject-matter of entries was wide-ranging and included MA’s reflections on the influence of the characteristics of the research team on the research. In particular, MA reflected on the influence of her underlying assumptions and beliefs about assisted dying practice emanating from living and researching in Australia. Other entries reflected on the influence on the research of some members of the research team being embedded in Belgian linguistic and medical culture. Reflections in the reflexive journal informed code development and theme generation.
Ethical approval and reporting of the study
Ethical approval was obtained for the study from the Medical Ethics Committee of the University of Brussels Hospital (BUN 1432022000043) and the Human Research Ethics Committee of the Queensland University of Technology (reference 2000000270).
This study is reported in accordance with the Consolidated Criteria for Reporting Qualitative Studies (‘COREQ’) (a completed COREQ checklist is presented in Supplementary File 2). 34 It is also reported in accordance with Braun and Clarke’s Reflexive Thematic Analysis Reporting Guidelines (‘RTARG’). Further reflections on the RTARG as they apply to the conduct and reporting of this research are provided in Supplementary File 3. 35
Results
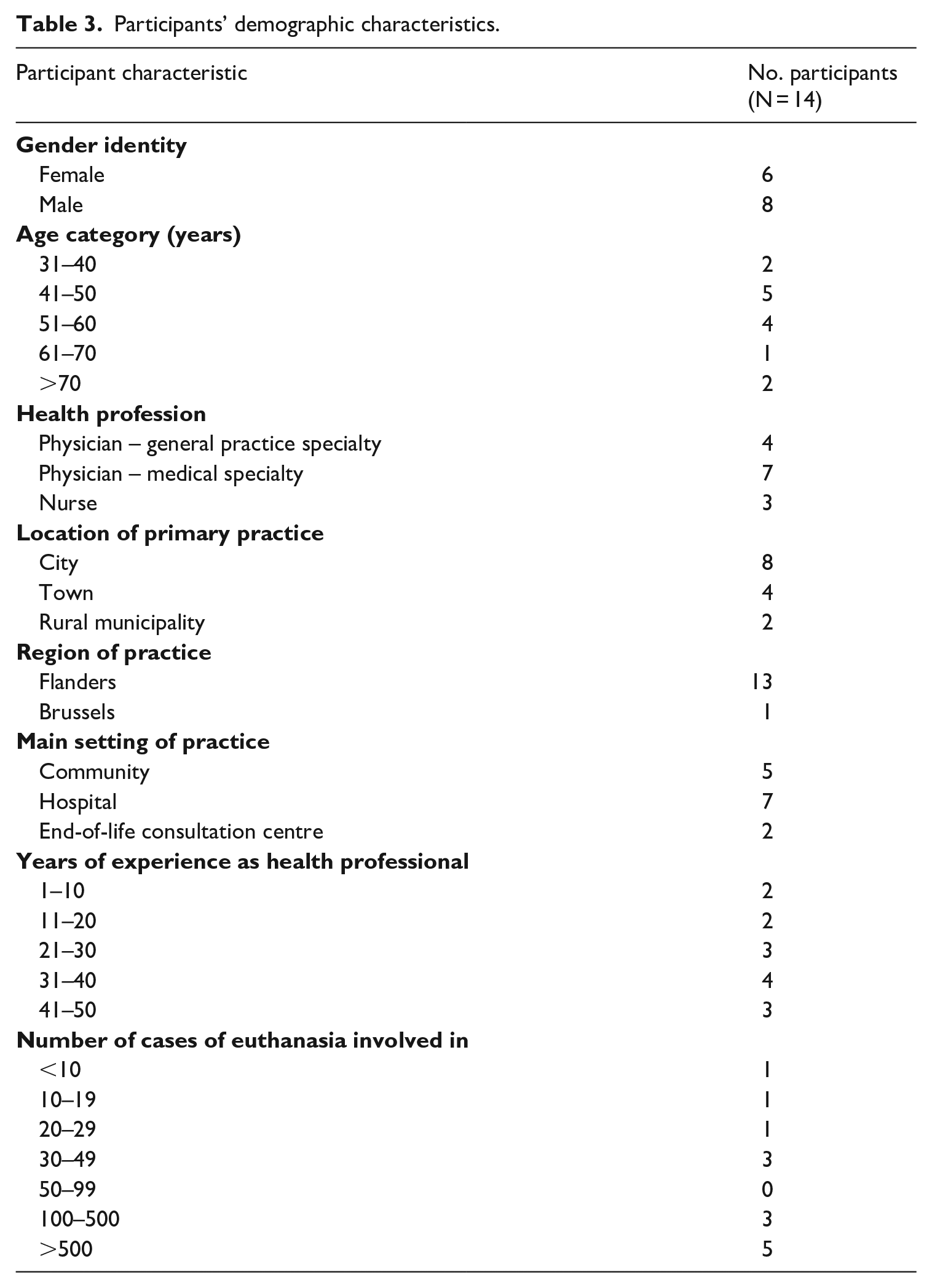
Twenty health professionals were interviewed, 14 of whom discussed the trial and therefore comprise the selection of participants included in this study (Table 3). The median interview length was 97 minutes (range: 65 to 111 minutes). Five of these 14 participants also had one or more regulatory roles in the broader Belgian euthanasia system, namely, previously or currently: having an organisational role in an end-of-life consultation centre (n = 2), being a member of a professional association which released guidelines on euthanasia (n = 3) or being a member of the FCECE (n = 2).
Participants’ demographic characteristics.
While we purposively selected participants to include individuals with diverse backgrounds and experiences, all participants reported having a Dutch-speaking cultural background. Most participants participated in the interview in English (n = 9), and fewer were supported to participate in English (n = 3) or participated in Dutch (n = 2).
The trial was significant for participants with most initiating the discussion of it without being prompted (n = 10). We generated four themes describing the practitioner-level influences of the trial and two themes describing its system-level influences.
Themes describing the practitioner-level influences of the trial
Theme 1: The trial prompted fear, insecurity, and a degree of reluctance to be involved in providing euthanasia
Most participants indicated that the trial has caused them to feel more fearful, exposed, vulnerable, or insecure in their euthanasia practice. Some reported that this fear has manifested in a reluctance to take a central role in the euthanasia assessment process (and be the first physician), as distinct from having a supportive role (as, for example, the second or third physician). Some reported that they now perceive continuing to provide euthanasia as legally risky, as they fear facing legal sanction for making a mistake. To illustrate, one physician participant described a distressing case in which they experienced problems with cannulation when administering the life-ending medication to an eligible patient with mental disorder. They described that they needed technical support to navigate this stressful event, but that they did not feel as though they could call for support without alerting the patient and others present during administration to the problem. They expressed,
. . . that situation itself is terrible, but the next month I am like really, really, really afraid that these people are going to sue me. (Participant identification number withheld to preserve anonymity)
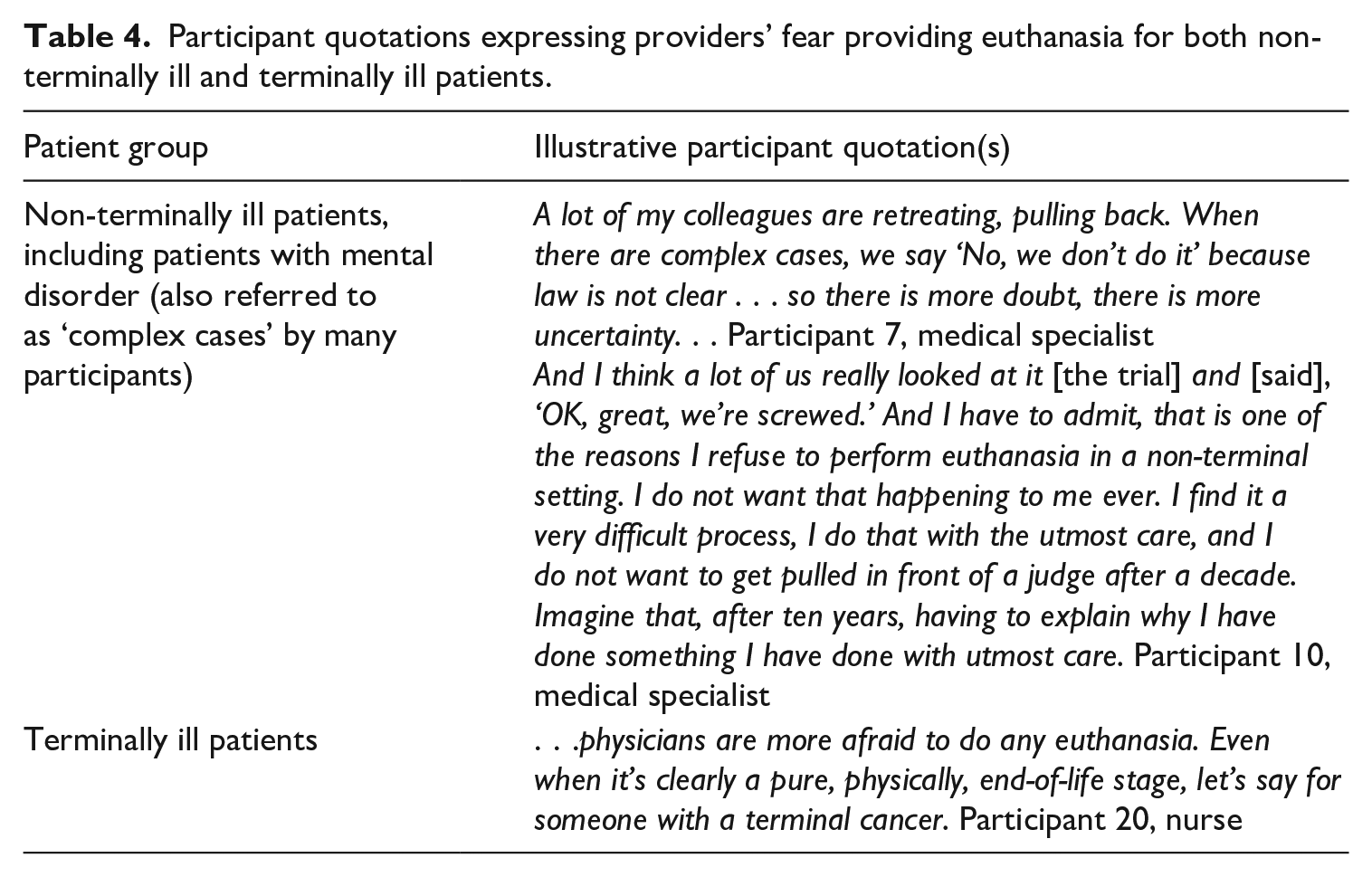
Many participants identified that this fear has permeated euthanasia provision across all patient types: patients who are not terminally ill, including patients with mental disorder, and patients who are terminally ill (see Table 4 for illustrative participant quotations). Several participants described that this fear has culminated in some providers ceasing to provide euthanasia for non-terminally ill patients. By contrast, one participant expressly reported that they did not think that terminally ill patients had been affected by the trial.
Participant quotations expressing providers’ fear providing euthanasia for both non-terminally ill and terminally ill patients.
One participant described having observed physicians employing strategies which they considered to reflect an avoidance of having to provide euthanasia (given their anxiety following the trial). They described that, at one point, some physicians in their facility claimed that they could not provide euthanasia due to the unavailability of a medicinal product used in administration. This product was available, however, only in ampules in a larger quantity than that specific amount needed for administration. Although the correct amount could still have been administered from the larger ampule with the intended effect, these physicians instead cited product unavailability as a reason for not providing. This participant considered that the product was available, notwithstanding that some of the medication would not need to be administered, and that this would have been obvious to those physicians.
Theme 2: Some providers adapted their euthanasia decision-making
Some participants expressed that the trial has prompted them to be more careful or thorough in their euthanasia decision-making. Four illustrations were provided by these participants (see Table 5 for illustrative participant quotations).
Participant quotations illustrating how, if at all, participants have altered their euthanasia decision-making following the trial.

First, some participants identified that they would be more likely to obtain further independent consultations on the patient’s eligibility in cases where the second physician disagreed with their assessment. In addition, a participant described that they would seek further independent consultations where the patient’s family members were not supportive of the patient accessing euthanasia, or where family members unsupportive of the patient’s decision to access were not involved in the assessment process.
Second, one participant identified that they have been more fulsome in the information they report to the FCECE following euthanasia, which has involved reporting information that the form does not require, expressly to ‘cover’ themselves.
Third, almost all participants reported that they are now placing increased importance on involving the patient’s family members in the euthanasia process and are going to greater lengths to engage them. Some expressed that prior to the trial, involving the family members was merely encouraged. They now adopt a firmer stance and wish for them to be involved unless this is inappropriate or impossible. Participants reported that the trial emphasising the importance of doing this has been a positive development and reflects best-practice. It has drawn their attention to the significant difficulties family members experience when they are not included and allows important discussions to take place before the patient has died.
Some participants’ increased awareness of the patient’s family members also appeared to have been motivated by risk-management considerations. For some participants, the trial demonstrated the harms for providers where family members complain about the euthanasia process, so measures to include them in the process, aside from reflecting best-practice, may more effectively protect them from legal sanction.
Fourth, some participants reported that following the trial they have adopted the recommendations in a guideline which was developed to assist providers to assess patients with mental disorder. 36
By contrast, some participants expressly reported that the trial has not altered their euthanasia decision-making. These participants referred to having confidence in their existing decision-making processes, which means that they have not needed to change their approach.
Theme 3: The trial exposed deficiencies with the Act
Many participants reported that the trial has prompted them to reflect that the Act does not adequately protect health professionals or their patients regarding the non-terminally ill assessment trajectory.
Intersecting with Theme 2, described above, some participants described perceiving a disconnect between the trial and the Act’s provision that a patient can legally exclude their family members from the euthanasia process. They described that the Act places providers in an untenably vulnerable situation; they cannot legally insist upon familial involvement in the procedure, however, their lack of involvement can expose them to possible legal sanction after the patient’s death:
. . . before the Tine Nys case, I always felt protected by the law. Before the Tine Nys case, I thought, ‘OK, fine, we have this law, it is quite clear on what is allowed and what is not allowed. You get checked by either one or two colleagues, highly educated, intelligent people who also know what they’re doing. You file your paperwork with the Commission, also intelligent, well-educated people who review this. And yes, job well done. Everyone has checked everything, it’s OK, there is no problem anymore’. And all of a sudden there was the Tine Nys case, and I was like, huh? Lovely surprise that this is possible. Because they didn’t win, but they didn’t lose either. So yeah, and that is, of course, the thing. Because it’s the patient who asks for euthanasia, not the family. So as for the policy in our [facility]. . . we try to involve the family as much as possible. But even if the entire family disagrees and the patient insists on euthanasia and is allowed to get it according to the law, they get it. (Participant 10, medical specialist)
For some participants, the trial has highlighted deficiencies with the legal requirements that apply for non-terminally ill patients. Their statements reflect that following these legal requirements does not furnish providers with sufficient guarantee that the euthanasia has been performed in accordance with the authorities’ views on this. Implicit in their statements was that the Act needs to be clearer and open to fewer interpretations if accusations are to be made that it was not adhered to in a given case.
Some participants considered that parts of the Act were not followed in TN’s assessment process. These participants empathised with the accused physicians and considered that they should never have been prosecuted. They identified that their mistakes were not intentional but, largely, were caused by a lack of clarity in the Act or a lack of knowledge about the Act. However, for these participants, the outcome of the trial (all three physicians were acquitted) highlights that a legal euthanasia assessment process does not equate to a best-practice euthanasia assessment process. In other words, mistakes and omissions can be made in euthanasia assessments, which may negatively influence the quality of care that a patient receives, but which are still permitted under the law (according to the trial). Accordingly, some participants identified that simply following the Act for non-terminally ill patients (including patients with mental disorder) does not guarantee that the experience reflects high-quality care from the patients’ perspective, nor that of their family members:
For complex [non-terminally ill] cases, the framework of the law and the evaluation of the law nowadays is not sufficient to promote good quality of care. But also to give professionals who want to perform euthanasia in these cases, to give them enough legal certainty. And, for instance, the trial we had is a good illustration of that. It should never have come to a trial, but these healthcare professionals should have been warned before they performed euthanasia that what they were doing was not right at all. (Participant 3, general practitioner)
Given these perceived deficiencies with the legal framework, several participants identified ways in which the Act or practice should adapt to afford sufficient protection to patients and providers. Several participants identified that prospective oversight is needed to give providers sufficient legal certainty to provide euthanasia in these ‘complex’ cases, namely, when patients are not terminally ill. Some also referred to the need to apply measures, in addition to the legal requirements, to better protect patients and providers.
Two recommendations made in the Flemish Association for Psychiatry’s (‘VVP’) guideline on assessing patients with mental disorder were highlighted by participants as being particularly important. One participant referred to the ‘two track’ approach the guideline recommends for assessing these patients. 37 This involves pursuing equally but separately a ‘life’ track, which aims at treating a patient’s mental disorder(s), and the ‘death’ track of the request for euthanasia. The participant described that this approach contributes to a more considered or rigorous decision-making process than that reflected in the Act alone, and therefore better protects providers and patients. Another participant emphasised the importance of the recommendation in the guideline of ensuring that the second and third physicians in the euthanasia assessment process agree with the first physician’s assessment before proceeding. They described that a prudent physician would no longer provide euthanasia if those second and third physicians considered that the patient was not eligible.
Theme 4: The trial clarified some legal requirements
Some participants identified that the trial has clarified some parts of the Act and assisted them to better understand their legal obligations. For example, the term ‘independent’ is used in the Act to refer to the second and third physicians’ relationship with the patient and with the first physician (see Table 1). A participant reported that the trial judgement clarified the meaning of this term:
They say, ‘Look, if you treat a patient as a specialist for one or two times, then you’re still independent. But if you’re an oncologist, and following your patient for two, three, four, five years, you’re not independent to that patient’. That’s what they say. (Participant 4, general practitioner)
Themes describing the system-level influences of the trial
Theme 5: Added burdens were placed on health service providers owing to the ‘chilling effect’ of the trial on practice
Many participants reported that health service providers were required to compensate for the reduction in the euthanasia workforce following the trial (illustrative participant quotes are presented in Table 6).
Participant quotes describing the chilling effect of the trial on euthanasia provision and how health service providers were required to compensate.
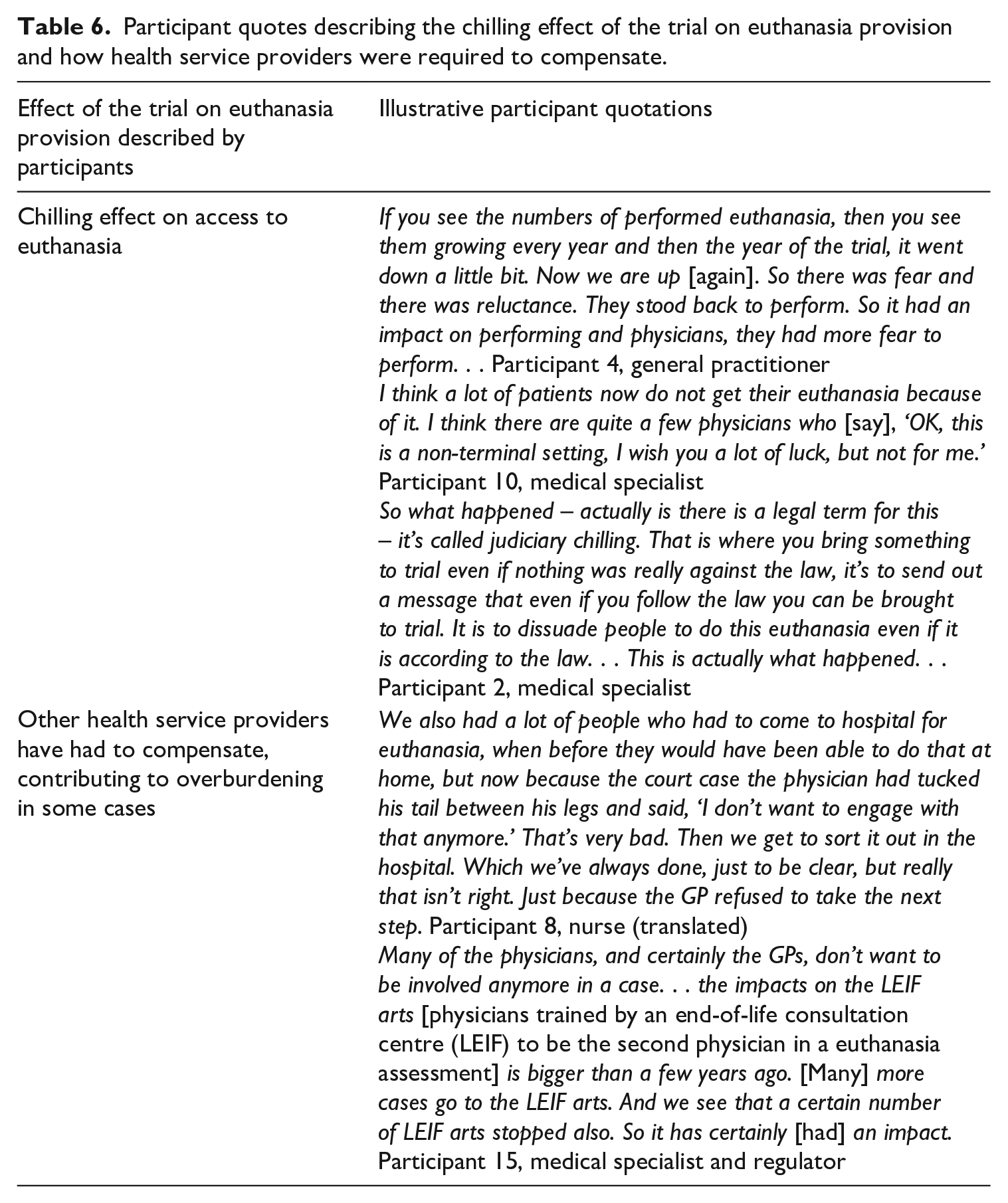
Several participants reported that the trial had a chilling effect on euthanasia provision at the system level. They reported that this contributed to an overall decrease in providers willing to provide euthanasia for patients with mental disorder in particular, but for terminally ill patients as well. In this way, this theme is a system-level corollary of providers having a degree of reluctance to provide (Theme 1).
Participants reported that certain areas of the euthanasia system had to compensate for the overall decrease in willing euthanasia providers. Some participants reported that this decrease contributed to added burdens for end-of-life consultation centres. Some also identified that it contributed to hospitals, particularly palliative care teams within them, receiving an increase in referrals to assess terminally ill patients for euthanasia, as their general practitioners had not wanted to be involved.
Theme 6: The trial prompted changes to the euthanasia regulatory landscape
One participant expressly reported that the trial prompted changes to the Belgian euthanasia regulatory landscape. They identified that the trial spurred the production of guidelines seeking to assist providers to carefully and thoroughly conduct euthanasia assessments for patients with mental disorder. Both guidelines, authored by the VVP and the National Order of Physicians (‘NOP’) respectively, recommend applying a process that exceeds the required legal provisions. The participant identified that the NOP guidelines draw heavily on the VVP’s guidelines by endorsing its requirements and adding more of its own. Several participants acknowledged the existence of these guidelines and, as discussed above (in Theme 2), some have adopted their recommendations.
Discussion
Summary of themes
This study investigated the influence of the first Belgian euthanasia criminal trial on providing physicians and nurses and the broader euthanasia system. At the practitioner level, themes generated are that the trial: prompted fear, insecurity, and a degree of reluctance to provide; caused some providers to adapt their euthanasia decision-making; exposed deficiencies with the Act; and clarified some legal requirements. The themes describing the system-level influences of the trial are that: added burdens were placed on health service providers owing to the ‘chilling effect’ of the trial on practice, and the trial prompted changes to the euthanasia regulatory landscape.
The themes generated in this study are linked. Health professionals having some reluctance to provide euthanasia (Theme 1) resulted in added burdens for other health service providers (Theme 5). While the trial has clarified some, specific provisions of the Act (Theme 4), it has simultaneously exposed deficiencies in the Act (Theme 3) and as a result, regulatory guidance has been produced (Theme 6). Some providers have altered their euthanasia decision-making (Theme 2) in order to lessen their fear in providing euthanasia (Theme 1).
Interpretation of the analysis
Participants in this study reported that the trial has had a significant impact on Belgian euthanasia practice, despite the accused physicians ultimately being acquitted. Participants reported the trial having affected euthanasia provision in relation to patients with mental disorder as well as other patients including patients who are terminally ill (owing to a perceived decrease in the Belgian euthanasia workforce). Data from the FCECE’s ninth and 10th biannual reports show a decrease in performed euthanasia cases between 2019 and 2020, at odds with the general upward trend in the number of performed euthanasia cases (which resumed subsequent to 2020). 38 This decrease was commented upon by the FCECE in its 10th and 11th reports; it noted that the trial may have played a role in relation to the decrease in cases (in addition to COVID-19). 39 The 10th report also referred to a survey published by LEIF which evidences a reticence among doctors ‘since the Tine Nys trial’ to ‘carry out euthanasia themselves, even in the case of terminally ill cancer patients’. 40 Although the number of reported, performed euthanasia cases has again increased since this trough, it is not clear whether this reflects that previously reticent practitioners have returned to euthanasia provision, or whether a reduced pool of practitioners have increased their workload. The FCECE does not report information on the number of participating physicians, only information in relation to physicians consulted. Quantitative research is needed to explore the link between the trial and evidence of the subsequent decrease in the euthanasia workforce (including whether that impact is still being observed in 2025 and beyond).
The extensive reporting of the trial by the media may have contributed to the trial’s impact. Local media outlets’ coverage of the trial was generally neutral, though there is evidence of selective reporting and the making of value judgements. 41 In addition, several media reports suggest that the trial had underlying political or religious motivations. 42 This too may have influenced participants’ perceptions of the trial and the integrity of its legal process, and the extent to which it deterred providers’ engagement in euthanasia for patients with mental disorder.
As described in Table 2, the trial was initiated by TN’s family members, who were upset that (and with how) euthanasia had been provided. This likely accounts for the considerable extent to which the study participants discussed the role of patients’ family members in the euthanasia process. Providers, naturally, seek to avoid complaints from the patient’s family members once the patient has died (this is discussed further below), so involving them in these decisions is one way to manage this risk. Simultaneously, the trial appears to have highlighted for participants the role that relational autonomy should have in the euthanasia process. 43 It is well understood that access to euthanasia is premised on notions of personal autonomy, and this is confirmed in the Belgian legislation. However, the trial has prompted some providers to reflect that relational autonomy should temper the primacy given to patients’ self-determination and decision-making in the confines of the colloque singulier (the physician–patient relationship). 44 Most participants acknowledged and empathised with the significant, negative, and lasting impacts that family members can experience if excluded from the euthanasia process. Existing research supports that end-of-life decision-making should reflect relational autonomy (in addition to personal autonomy). 45
Situating the themes in the context of existing empirical and regulatory literature
These results advance existing Belgian and Dutch literature exploring the influence of the first euthanasia trial in practice. 46 This research suggests that the trial has caused reticence among some physicians to provide euthanasia in its specific context (euthanasia for mental disorder) and provided evidence of a subsequent decrease in the pool of willing providers and increased referrals to already overburdened end-of-life consultation centres. 47 However, this study goes further by illustrating the ways in which some physicians have altered their euthanasia decision-making generally as a result of the trial. In addition, it demonstrates that the influence of the trial has not been confined to patients with mental disorder, that it prompted regulatory guidance, clarified some of the legal requirements, and exposed deficiencies with the Act. This study further demonstrates that the trial’s influence was not limited to the period immediately following the judgement; impacts were still being reported four years later (when data generation in this study concluded).
The finding in this study that participants do not necessarily equate quality euthanasia practice and decision-making with legal euthanasia practice and decision-making has also been identified in the literature. De Hert and colleagues’ analysis of this case concluded that more is needed in the euthanasia assessment of non-terminally ill individuals to ensure that ‘due care’ is truly exercised. They support the development of the VVP’s guidelines which seek to improve the quality of the euthanasia assessment of persons with mental disorder, in particular, the additional processes it recommends assessing practitioners include in the process. 48 Empirical research also demonstrates that euthanasia providers consider the legislation to reflect the ‘bare minimum’ for euthanasia practice, and fill gaps in the law in several, varied ways to ensure they are exercising due care when providing euthanasia for their patients. 49
The analysis also supports the regulatory literature which suggests that criminal prosecutions serve a deterrence purpose. Many participants in this study perceived the symbolic nature of the trial in its denunciation of euthanasia for patients with mental disorder (whether intended or not).
With respect to defensive medicine, this has been demonstrated insofar as participants adapted their euthanasia decision-making, motivated by risk avoidance and ‘legal self-interest’. 50 As observed in this study, research describes physicians engaging in ‘positive’ defensive medicine where they add excessive or unnecessary information to official documents, only because of fear of legal repercussions. 51 Also as observed in this study, research shows that ‘negative’ defensive medicine includes physicians avoiding patients and cases they perceive as ‘high risk’. 52 However, the trial prompted many participants to deeply reflect on best-practice or optimal euthanasia care. Often, it was a focus on best-practice that motivated providers’ decisions to alter their euthanasia decision-making. These changes were not solely driven by participants seeking to protect themselves against legal risks, but the need to enhance the quality of the euthanasia process. To this end, these alterations are not demonstrative of defensive medicine, which by definition involves taking actions which do not reflect a focus on patient safety and care. 53 To illustrate, research has identified that making unnecessary referrals to other practitioners is demonstrative of defensive medicine. 54 In this study, participants did not perceive these additional consultations as unnecessary, rather, important for accurately verifying the patient’s eligibility for euthanasia.
Implications for policy and research
Should further research demonstrate that the pool of willing providers is still reduced, measures are needed to address this to ensure the sustainability of the euthanasia workforce and end-of-life consultation centres. This should include sharing accurate information with providers about the trial and its implications. So doing may allay fears, enhance providers’ confidence, and correct any exaggerated or missing information included (or not included) in media reports. 55 The feasibility and value of the suggestion from some participants about implementing prospective approval in complex euthanasia cases should be considered (including an exploration of providers’ attitudes towards such prospective approval). 56
Reconnecting with regulatory theory, the findings in this study also point to the need for further research on the effectiveness of various forms of euthanasia regulation in steering the behaviour of participating health professionals towards desired conduct. Research on the Belgian euthanasia regulatory framework has shown that this framework includes a range of mechanisms used to control euthanasia practice. This includes prescribing desired conduct prospectively, for instance, through publishing policies and guidelines, and prescribing conduct retrospectively, for instance, by punitively sanctioning illegal conduct (such as occurred in this trial). 57 The findings in this research suggest that securing Belgian providers’ continued participation in euthanasia may rest on the prioritisation of ‘educative’ as opposed to ‘punitive’ approaches. It follows that an emphasis on educative approaches may also be more effective than punitive approaches in securing compliance with the legal requirements. For instance, though the educative approach reportedly taken by the FCECE in response to minor or procedural transgressions of the law are often criticised in the literature, 58 this approach may be more effective than prosecutorial referrals in securing compliance with the obligation to report cases.
Research on Australia’s voluntary assisted dying regulatory framework supports that educative approaches are generally more effective in relation to a ‘minor error or non-serious breach’. 59 Indeed, the installation of the FCECE as a buffer between the reporting physician and the criminal justice system was ‘based on the idea that a physician does not want to (nor should) be dealt with in an atmosphere of criminality’ with the intention of optimising compliance with the obligation to report cases. 60 Accordingly, future research should focus on this issue and explore the relative effectiveness of what might be characterised as ‘punitive’ as opposed to ‘educative’ regulatory mechanisms in the Belgian euthanasia system. This research may provide important evidence for Belgium and international jurisdictions considering reform about the function and utility of the regulatory approaches policymakers have available to them when attempting to shape the behaviour of euthanasia providers. In March 2024, amendments to the Act were passed which partly reflect this criminal trial and the Constitutional Court case which followed it. 61 Before these amendments, the Act provided for only one sanction attaching to a breach of the Act. This meant that any breach, however minor, could result in a charge for murder. The Belgian Constitutional Court found that this penalty regime was unconstitutional. Accordingly, one of the recent amendments establishes different sanctions that apply to a breach of a ‘basic’ as opposed to a ‘procedural’ condition of the Act. Future research should explore euthanasia providers’ perceptions of these amendments and identify how they may influence providers’ willingness to be involved in providing euthanasia.
Strengths and limitations
This study is the first to examine the wider impact of the first Belgian criminal trial on euthanasia practice. Strengths of the research include selecting participants with a diverse range of experiences providing euthanasia and wider system perspectives given their dual roles as regulators. The overall number of participants included in the study is relatively small which may mean that only individuals with strong views on euthanasia regulation (including the trial) were included, and which reflects limited cultural diversity between participants (and there were no Walloon participants included). One participant practising in the Brussels region (which is officially bilingual) provided some insights on the impact of the trial on French-speaking physicians. However, more research is needed to investigate the Brussels and Walloon experiences in greater depth (noting that there was likely less publicity of the trial outside of Flanders).
While most participants were interviewed in English (not their Dutch mother tongue), most participants were highly proficient speaking English and strategies were employed to ensure researchers and participants could communicate effectively. In addition, reflections about the role of language in the interviews made in MA’s reflexive journal entries informed the coding and theme generation processes. Because interviews for this study ceased when information power for the study as a whole had been reached, it is possible some influences of the trial may not have been included.
Conclusion
This study investigated the influence of the first Belgian euthanasia criminal trial on Belgian euthanasia practice. While previous research focused on the impact of the trial in the context of patients with mental disorder, this study had a broader focus, and investigated the influence of the trial on individual practitioners and the euthanasia system. On the practitioner level, themes generated are that the trial has prompted fear, insecurity, and a degree of reluctance to provide; caused some providers to adapt their euthanasia decision-making; exposed deficiencies with the Act; and clarified some legal requirements. On the system level, themes generated are that added burdens were placed on health service providers owing to the trial’s ‘chilling effect’ on practice, and regulatory guidance was produced. An important observation from participants is that the trial has not only affected euthanasia practice in the context of patients with mental disorder, but in relation to all patients, including those who are terminally ill owing to a decrease in the Belgian euthanasia workforce. Measures are needed to ensure the sustainability of the euthanasia workforce if this problem has persisted, which may include distributing accurate information to providers about learnings from the trial.
Supplemental Material
sj-docx-1-mli-10.1177_09685332251338659 – Supplemental material for Health professionals’ perspectives on the first Belgian euthanasia criminal trial: A qualitative study
Supplemental material, sj-docx-1-mli-10.1177_09685332251338659 for Health professionals’ perspectives on the first Belgian euthanasia criminal trial: A qualitative study by Madeleine Archer, Lindy Willmott, Kenneth Chambaere, Luc Deliens and Ben P White in Medical Law International
Supplemental Material
sj-docx-2-mli-10.1177_09685332251338659 – Supplemental material for Health professionals’ perspectives on the first Belgian euthanasia criminal trial: A qualitative study
Supplemental material, sj-docx-2-mli-10.1177_09685332251338659 for Health professionals’ perspectives on the first Belgian euthanasia criminal trial: A qualitative study by Madeleine Archer, Lindy Willmott, Kenneth Chambaere, Luc Deliens and Ben P White in Medical Law International
Supplemental Material
sj-docx-3-mli-10.1177_09685332251338659 – Supplemental material for Health professionals’ perspectives on the first Belgian euthanasia criminal trial: A qualitative study
Supplemental material, sj-docx-3-mli-10.1177_09685332251338659 for Health professionals’ perspectives on the first Belgian euthanasia criminal trial: A qualitative study by Madeleine Archer, Lindy Willmott, Kenneth Chambaere, Luc Deliens and Ben P White in Medical Law International
Footnotes
Acknowledgements
We would like to acknowledge the study participants who generously shared their insights and experiences with us for this research. We also acknowledge and thank Tessa Holzman for her work translating the Flemish interviews.
Data availability
The interview guide used in the study is contained in Supplemental File 1. The data generated and analysed in this study are not publicly available consistent with the study’s ethical approval and the need to ensure participant confidentiality. Queries regarding the availability of data should be directed to the corresponding author.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: B.P.W. and L.W. were engaged by the Victorian, Western Australian and Queensland state governments in Australia to develop the legislatively mandated training for health professionals who provide assisted dying. M.A. is or has been employed on these projects. L.W. is a member of the oversight body for assisted dying in Queensland, the Voluntary Assisted Dying Review Board. The other authors have no potential conflicts of interest to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was funded by the Australian Research Council Future Fellowship project entitled ‘Enhancing End-of-Life Decision-Making: Optimal Regulation of Voluntary Assisted Dying’ (project number FT190100410). The funder had no role in the study design, data collection, data analysis, data interpretation or writing of the manuscript.
Ethical considerations
The study was reviewed and approved by the Medical Ethics Committee of the Brussels University Hospital with reference BUN 1432022000043 and the Queensland University of Technology Human Research Ethics Committee with reference 2000000270.
Consent to participate
All participants in this study provided written consent to participate (which was confirmed verbally during the interview).
Supplemental material
Supplemental material for this article is available online.
1.
M. De Hert, S. Sterckx, and K. Van Assche, ‘Due Care in the Context of Euthanasia Requests by Persons with Psychiatric Illness: Lessons from a Recent Criminal Trial in Belgium’, in M. Cholbi and J. Varelius, eds., New Directions in the Ethics of Assisted Suicide and Euthanasia (Cham: Springer International Publishing, 2023), pp. 186–187.
2.
There is no official English translation of the Belgian euthanasia legislation published by Parliament, it is published only in Dutch and French. Accordingly, references to the legislation in this article are references to the English translation of the legislation contained in a Belgian Constitutional Court judgement: Judgement 153/2015 [2015] Constitutional Court (Belgium).
3.
Op. cit., p. 5.
4.
Op. cit., pp. 7–10; Note that some of the provisions of the Belgian Act on Euthanasia (‘the Act’) were amended in a 2024 amendment to the legislation. The legal requirements referred to in this section were not altered in this amendment: Loi portant dispositions en matière de digitalisation de la justice et dispositions diverses II [Law on the digitisation of justice and miscellaneous provisions], Belgian Official Gazette, 15 May 2024.
5.
De Hert et al., Due Care in the Context of Euthanasia Requests by Persons with Psychiatric Illness; M. De Hert, S. Loos, S. Sterckx, E. Thys, and K. Van Assche, ‘Improving Control over Euthanasia of Persons with Psychiatric Illness: Lessons from the First Belgian Criminal Court Case Concerning Euthanasia’, Frontiers in Psychiatry, 13 (2022), p. 933748.
6.
M. De Hert, E. Thys, K. Catthoor, K. Van den Broeck, F. Matthys, K. Vansteelandt, and J. Detraux, ‘Media Coverage of Belgium’s First Criminal Case Concerning Euthanasia for Psychiatric Patients: A Content Analysis of Flemish Newspapers and Magazines’, Frontiers in Psychiatry, 13 (2023), p. 1050086.
7.
G. Huysmans, ‘Hoezo, Geen Euthanasie Maar “hulp Bij Zelfdoding” [Why, Not Euthanasia but ’Assisted Suicide’]’ (in Dutch), De Standaard (Brussels, 30 April 2019); VRT, ‘Arts niet vervolgd voor hulp bij zelfdoding [Doctor not prosecuted for assisting suicide]’ (in Dutch), De Standaard (Brussels, 26 April 2019); F. Schweitser, J. Stuy, W. Distelmans, C. Lemmens, and J. Braeckman, ‘This Is Not an Act of Euthanasia: Legally Correct but Ethically Problematic?’, Medical Law International 24 (2024), p. 8. Regarding another relevant, yet distinct case (because it did not involve prosecution based on a suspected breach of the conditions of the euthanasia law), see also: T. Vansweevelt, ‘Medical Confidentiality and (Un)lawful End-of-Life Decisions: The Case of the ‘Deacon of Death’, Medicine and Law, 37 (2018), pp. 1–17.
8.
De Hert et al., ‘Improving Control Over Euthanasia’; De Hert et al., ‘Due Care in the Context of Euthanasia Requests by Persons with Psychiatric Illness’; YH. Leleu, ‘L’euthanasie des patients psychiatriques au banc des accuses’ (in Dutch), Revue de Jurisprudence de Liège, 23 (2020), p. 1095; M. De Hert, ‘Drie euthanasie-artsen vrijgesproken voor moord door het hof van assisen [Three euthanasia doctors acquitted of murder by the Assize Court]’ (in Dutch), Tijdschrift voor Gezondheidsrecht, (2021), p. 334; Judgement 134/2022 [2022] Constitutional Court (Belgium); R. Watson, ‘Assisted Dying: Belgian Doctors Stand Trial in Landmark Case’, BMJ (Clinical research ed.), 368 (2020), p. m259; door Belga, ‘Arts die euthanasie Tine Nys uitvoerde, maakte geen fout [Doctor who performed euthanasia of Tine Nys made no mistake]’ (in Dutch), De Specialist, 24 October 2023, available at ![]() (accessed 13 June 2024).
(accessed 13 June 2024).
9.
De Hert et al., Due Care in the Context of Euthanasia Requests by Persons with Psychiatric Illness.
10.
De Hert et al., ‘Media Coverage’.
11.
End-of-life consultation centres have been established in Belgium with the aim of supporting patients to access euthanasia assessments. Many of these centres receive referrals from patients’ treating medical practitioners and provide euthanasia assessments and support for patients seeking to access euthanasia. These centres often have expertise in conducting euthanasia assessments in ‘complex cases’, particularly assessing patients whose sole or underlying condition is mental disorder: M. Archer, L. Willmott, K. Chambaere, L. Deliens, and B. White, ‘Mapping Sources of Assisted Dying Regulation in Belgium: A Scoping Review of the Literature’, OMEGA – Journal of Death and Dying. Epub ahead of print November 2023. DOI: 10.1177/00302228231210146; M. Verhofstadt, K. Audenaert, F. Mortier, L. Deliens, A. Liégeois, K. Pardon, and K. Chambaere, ‘Concrete Experiences and Support Needs Regarding the Euthanasia Practice in Adults With Psychiatric Conditions: A Qualitative Interview Study Among Healthcare Professionals and Volunteers in Belgium’, Frontiers in Psychiatry, 13 (2022), p. 859745.
12.
Verhofstadt et al., ‘Concrete Experiences’.
13.
M. Verhofstadt, K. Van Assche, K. Pardon, M. Gleydura, K. Titeca, and K. Chambaere, ‘Perspectives on the Eligibility Criteria for Euthanasia for Mental Suffering Caused by Psychiatric Disorder under the Belgian Euthanasia Law: A Qualitative Interview Study among Mental Healthcare Workers’, International Journal of Law and Psychiatry, 93 (2024), p. 101961.
14.
E. Asscher and S. van de Vathorst, ‘First Prosecution of a Dutch Doctor since the Euthanasia Act of 2002: What Does the Verdict Mean?’, Journal of Medical Ethics, 46 (2020), p. 74.
15.
Elizabeth Baldwin, Andreas Thiel, Michael McGinnis, and Elke Kellner, ‘Empirical Research on Polycentric Governance: Critical Gaps and a Framework for Studying Long-Term Change’, Policy Studies Journal, 52 (2024), p. 319.
16.
K. Hawkins, ‘Law As Last Resort’ in R. Baldwin, C. Scott and C. Hood, eds., A Reader on Regulation (Oxford: Oxford University Press, 1998).
17.
I. Ayres and J. Braithwaite, Responsive Regulation: Transcending the Deregulation Debate (Oxford: Oxford University Press, 1992), pp. 35–38.
18.
Hawkins, Law as a Last Resort, p. 291.
19.
Op. cit., pp. 291, 295–6.
20.
Ayres and Braithwaite, Responsive Regulation, p. 26; Hawkins, Law as a Last Resort, pp. 295–296.
21.
S. Van McCrary, J. Swanson, H. Perkins, and W. Winslade, ‘Treatment Decisions for Terminally Ill Patients: Physicians’ Legal Defensiveness and Knowledge of Medical Law’, Law, Medicine and Health Care, 20 (1992), pp. 18–21.
22.
Op. cit.
23.
Archer et al., ‘Mapping Sources of Assisted Dying Regulation’; M. Archer, L. Willmott, K. Chambaere, L. Deliens, and B. P. White, ‘What Domains of Belgian Euthanasia Practice are Governed and by Which sources of Regulation: A Scoping Review’, OMEGA – Journal of Death and Dying, (2023).
24.
J. Maxwell, A Realist Approach for Qualitative Research (Thousand Oaks, CA: Sage, 2012). Consistent with this position, the authors have approached this research from the perspective that existence is separate from meaning. This means that individuals each have their own interpretations of experiences and events, and there is no such thing as an objective reality that research aims to find or uncover. Rather, research aims to illustrate and describe individuals’ unique perspectives which are their constructions of ‘reality’.
25.
E. Inghelbrecht, J. Bilsen, F. Mortier, and L. Deliens, ‘The Role of Nurses in Physician-Assisted Deaths in Belgium’, Canadian Medical Association Journal, 182 (2010), pp. 906–907; N. De Bal, C. Gastmans, and B. Dierckx de Casterlè, ‘Nurses’ Involvement in the Care of Patients Requesting Euthanasia: A Review of the Literature’, International Journal of Nursing Studies, 45 (2008), pp. 635–639.
26.
M. Patton, Qualitative Evaluation and Research Methods, 4th ed. (Thousand Oaks, CA: Sage, 2015).
27.
Archer et al., ‘Mapping Sources of Assisted Dying Regulation’.
28.
S. Tracy, ‘Qualitative Quality: Eight “Big-Tent” Criteria for Excellent Qualitative Research’, Qualitative Inquiry, 16 (2010), p. 844.
29.
V. Braun and V. Clarke, ‘Using Thematic Analysis in Psychology’, Qualitative Research in Psychology, 3 (2006), pp. 77–101; V. Braun and V. Clarke, Thematic Analysis: A Practical Guide (Thousand Oaks, CA: Sage, 2022).
30.
Braun and Clarke, Thematic Analysis: A Practical Guide, pp. 9–11.
31.
K. Malterud, V. Siersma, and A. Guassora, ‘Sample Size in Qualitative Interview Studies: Guided by Information Power’, Qualitative Health Research, 26 (2016), pp. 1753–1760.
32.
Braun and Clarke, ‘Using Thematic Analysis in Psychology’, pp. 91–92.
33.
Braun and Clarke, Thematic Analysis: A Practical Guide, pp. 19–22.
34.
A. Tong, P. Sainsbury, and J. Craig, ‘Consolidated Criteria for Reporting Qualitative Research (COREQ): A 32-Item Checklist for Interviews and Focus Groups’, International Journal for Quality in Health Care, 19 (2007), pp. 349–357.
35.
V. Braun and V. Clarke, ‘Supporting Best Practice in Reflexive Thematic Analysis Reporting in Palliative Medicine: A Review of Published Research and Introduction to the Reflexive Thematic Analysis Reporting Guidelines (RTARG)’, Palliative Medicine, 38 (2024), pp. 608–616.
36.
37.
Flemish Psychiatric Association ‘How to Handle a Patient Request for Euthanasia in Psychiatry under Current Law?’.
38.
Federale Controle- en and Evaluatiecommissie Euthanasie, ‘Negende verslag aan de wetgevende kamers 2018 - 2019’, Federale overheidsdienst, Volksgezondheid, Veiligheid van de Voedselketen en Leefmilieu 2019, available at https://overlegorganen.gezondheid.belgie.be/nl/documenten/fcee-euthanasie-verslag-2020 (accessed 24 January 2025); Federale Controle- en and Evaluatiecommissie Euthanasie, ‘Tiende verslag aan de wetgevende kamers (jaren 2020 - 2021)’, Federale overheidsdienst, Volksgezondheid, Veiligheid van de Voedselketen en Leefmilieu 2022, available at https://overlegorganen.gezondheid.belgie.be/nl/documenten/fcee-verslag-euthanasie-2022 (accessed 24 January 2025); Federale Controle- en Evaluatiecommissie and Euthanasie, ‘11de verslag aan de wetgevende kamers (jaren 2022-2023)’, 2025, available at ![]() (accessed 24 January 2025).
(accessed 24 January 2025).
39.
Federale Controle- en Evaluatiecommissie and Euthanasie, ‘Tiende verslag aan de wetgevende kamers (jaren 2020 - 2021)’, pp. 12, 25; Federale Controle- en Evaluatiecommissie and Euthanasie, ‘11de verslag aan de wetgevende kamers (jaren 2022-2023)’, p. 14.
40.
Federale Controle- en Evaluatiecommissie and Euthanasie. ‘Tiende verslag aan de wetgevende kamers (jaren 2020 - 2021)’, p. 24. Please note this has been translated into English. See also L. V. Casteele and W. Distelmans, ‘Is de houding van LEIFartsen veranderd na het euthanasieproces?’, Huisartsnu, [2022],
41.
De Hert et al., ‘Media Coverage’, p. 15; De Hert, ‘Three euthanasia doctors acquitted’, p. 334.
42.
De Hert et al., ‘Media Coverage’, pp. 13–14, 16.
43.
The notion of personal autonomy reflects a patient’s ‘personal self-governance’ and being able to choose for oneself: M. Sjöstrand, G. Helgesson, S. Eriksson, and N. Juth, ‘Autonomy-Based Arguments against Physician-Assisted Suicide and Euthanasia: A Critique’, Medicine, Health Care and Philosophy, 16 (2013), p. 226. The notion of relational autonomy reflects that autonomy ‘emerges within and because of relationships’. It emphasises that individuals make decisions in the context of their social environment and that decisions are characterised by interdependence and interconnection with others: A. Wand, C. Peisah, B. Draper, and H Brodaty, ‘The Nexus between Elder Abuse, Suicide, and Assisted Dying: The Importance of Relational Autonomy and Undue Influence’, Macquarie Law Journal, 18 (2018), p. 80; C. Ells, M. Hunt, and J. Chambers-Evans, ‘Relational Autonomy as an Essential Component of Patient-Centered Care’, International Journal of Feminist Approaches to Bioethics, 4 (2011), pp. 85–86.
44.
N. Hamarat, A. Pillonel. M. Berthod, D. Castelli Dransart, and G. Lebeer, ‘Exploring Contemporary Forms of Aid in Dying: An Ethnography of Euthanasia in Belgium and Assisted Suicide in Switzerland’, Death Studies, 46 (2021), pp. 1593–1607.
45.
C. Gómez-Vírseda, Y. De Maeseneer, and C. Gastmans, ‘Relational Autonomy in End-of-Life Care Ethics: A Contextualized Approach to Real-Life Complexities’, BMC Medical Ethics, 21 (2020), p. 50; C. Variath, E. Peter, L. Cranley, D. Godkin, and D. Just, ‘Relational Influences on Experiences with Assisted Dying: A Scoping Review’, Nursing Ethics, 27 (2020), pp. 1501–1516.
46.
Verhofstadt et al., ‘Concrete Experiences’.
47.
Op. cit.; Asscher and van de Vathorst, ‘First Prosecution of a Dutch Doctor’.
48.
M. De Hert, S. Sterckx and K. Van Assche, ‘Due Care in the Context of Euthanasia Requests by Persons with Psychiatric Illness: Lessons from a Recent Criminal Trial in Belgium’ in Michael Cholbi and Jukka Varelius, eds., New Directions in the Ethics of Assisted Suicide and Euthanasia (Cham: Springer International Publishing, 2023), p. 181.
49.
M. Archer, L. Willmott, K. Chambaere, L. Deliens and B. P. White, ‘How Does Regulation Influence Euthanasia Practice in Belgium? A Qualitative Exploration of Involved Doctors’ and Nurses’, Perspectives’ Medical Law Review, 33(1) (2025), p. fwaf003.
50.
M. Kapp, ‘Defensive Medicine: No Wonder Policymakers Are Confused’, International Journal of Risk & Safety in Medicine, 28 (2016), p. 213.
51.
M. Catino, ‘Blame Culture and Defensive Medicine’, Cognition, Technology & Work, 11 (2009), p. 249; S. Ramella, G. Mandoliti, L. Trodella, and R. D’Angelillo, ‘The First Survey on Defensive Medicine in Radiation Oncology’, La Radiologia Medica, 120 (2015), p. 423; N. Ries and J. Jansen, ‘Physicians’ Views and Experiences of Defensive Medicine: An International Review of Empirical Research’, Health Policy, 125 (2021), pp. 634–642.
52.
A. Shenoy, G. Shenoy, and G. Shenoy, ‘Patient Safety Assurance in the Age of Defensive Medicine: A Review’, Patient Safety in Surgery, 16 (2022), p. 10; Ramella et al., ‘First Survey on Defensive Medicine’, p. 423.
53.
Shenoy et al., ‘Patient Safety Assurance’.
54.
Ramella et al., ‘First Survey on Defensive Medicine’, p. 423; Ries and Jansen, ‘Physicians’ Views and Experiences of Defensive Medicine’.
55.
De Hert et al., ‘Media Coverage’.
56.
B. White and L. Willmott, ‘Evidence-Based Law Making on Voluntary Assisted Dying’, Australian Health Review, 44 (2020), pp. 544–546.
57.
Archer et al., ‘Mapping Sources of Assisted Dying Regulation in Belgium’.
58.
See, eg, K. Raus, B. Vanderhaegen and S. Sterckx, ‘Euthanasia in Belgium: Shortcomings of the Law and Its Application and of the Monitoring of Practice’, Journal of Medicine and Philosophy 46 (2021), p. 80.
59.
B. P White, C. M. Haining, and L. Willmott, ‘How Best to Regulate Voluntary Assisted Dying: A Qualitative Study of Perceptions of Australian Doctors and Regulators’, Medical Law Review, 33(1) (2025), p. fwae045.
60.
H. Nys, ‘A Discussion of the Legal Rules on Euthanasia in Belgium Briefly Compared with the Rules in Luxembourg and the Netherlands’, in David Albert Jones, Chris Gastmans and C MacKellar, eds., Euthanasia and Assisted Suicide: Lessons from Belgium (Cambridge: Cambridge University Press, 2018), p. 23.
61.
See M. De Hert, S. Loos, and K. Van Assche, ‘The Belgian Euthanasia Law Under Scrutiny of the Highest Courts’, The Lancet Regional Health, 24 (2023), p. 100549.
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.