
Abstract
This article examines the role of patients and caregivers as ‘regulatory actors’ in healthcare. It uses and extends ‘regulatory space theory’ to argue that failing to consider the role of patients and caregivers as ‘regulatory actors’ in healthcare regulatory spaces misses a key piece of the regulatory puzzle. We argue that in assisted dying and other healthcare contexts, evidence shows that some patients and caregivers do behave as regulatory actors, engaging in sustained and focused attempts to alter behaviour. We then suggest a framework which explicitly incorporates notions of why patients and caregivers act in regulatory ways is helpful in understanding what the appropriate response to such actions should be. While the contribution of patients and caregivers to regulation is valuable and should be supported where desired by the person, if patients and caregivers are acting out of necessity to address system issues or ‘regulatory failure’, other regulatory actors (e.g. governments) should proactively respond and address these issues to reduce the burden on patients and caregivers of having to take regulatory action.
Keywords
Introduction
Patients and caregivers have historically been absent from discussions about who ‘regulates’ healthcare. 1 The way regulation has traditionally been conceived – as the promulgation of rules by the state, accompanied by monitoring and enforcement mechanisms 2 – leaves no room for patients and caregivers to be considered actors within the ‘regulatory space’. 3 There are many definitions of regulation, 4 ranging from traditional state-centric conceptions of regulation to very broad definitions that conceive of regulation as anything producing effects on behaviour. 5 In the healthcare context, as in other fields of regulation, it is increasingly recognised that regulation is decentred and polycentric, 6 meaning that many actors beyond the state influence behaviour (including by making sustained and focused attempts to alter behaviour) 7 and may be conceived of as ‘regulatory actors’. To date, and despite a vast literature discussing the importance of involving and engaging patients and caregivers in healthcare delivery and design, 8 the regulatory role of patients and caregivers in decentred and polycentric healthcare systems has been understudied or overlooked.
This article uses Hancher and Moran’s regulatory space theory, as well as the case study of assisted dying (‘AD’), to argue that overlooking the role of patients and caregivers as regulatory actors in healthcare is to miss a key piece of the regulatory puzzle. 9 The central premise of Hancher and Moran’s theory is that ‘regulation is best understood through the analytical device of “regulatory space”’: regulation is a product of the interactions between occupants (or ‘actors’) within a particular space (e.g. AD). 10 The boundaries of the regulatory space are determined by various factors, including the prevailing understanding of regulation as well as the national, political, legal, social, and cultural context. 11 Hancher and Moran suggest that considering regulation in terms of a regulatory space ‘encourages us to examine the characteristics of the excluded’. 12 Patients’ and caregivers’ historical exclusion or omission from healthcare regulatory spaces may be a product of the dimensions of power and politics, 13 and a remnant of more paternalistic conceptions of healthcare where patients were seen purely as passive recipients of care. 14 Interestingly, Hancher and Moran themselves argue that individuals generally have a limited regulatory role and one that is usually tied to an organisation. 15 In this article, we challenge and extend Hancher and Moran’s theory by arguing that patients and caregivers are capable of behaving as regulatory actors independently of organisational affiliations, including by acting to intentionally influence behaviour of others. 16 We draw on findings from empirical research in the AD context and on examples of actions by patients and caregivers in other healthcare contexts to argue that we must recognise that patients and caregivers can be regulatory actors in healthcare regulatory spaces more broadly. 17 However, we also agree with Hancher and Moran that organisations are important: patients and caregivers form connections or ‘networks’ with organisations which facilitates regulatory action, and the implications of this are also discussed in this article.
From our analysis of evidence of regulatory action by patients and caregivers in AD and other healthcare contexts, we observe that in healthcare contexts that are newer (such as AD in Australia and Canada) or where there are political dimensions, power imbalances, stigmatisation, or regulatory failure, 18 patients and caregivers often take on a regulatory role out of necessity to influence change. 19 An implication of this observation is that it is imperative to consider why patients and caregivers enter the regulatory space and seek to alter behaviour. Where they are required to enter into the regulatory space out of necessity to address system issues (such as barriers to access or gaps in regulation), we suggest this is problematic and that other actors in the regulatory space (e.g. government actors, healthcare institutions, and health professionals who are responsible for the delivery of healthcare) should act to address such issues. However, we also argue that it is important for patients and caregivers to be invited into and supported within the regulatory space if they wish to be, 20 because the value of involving patients and caregivers to improve healthcare systems is increasingly recognised, through democratic, 21 market-based/consumerist, 22 expertise, 23 and pragmatic lenses. 24
Drawing on our analysis of regulatory action by patients and caregivers in AD and other contexts, we propose a tripartite classification of patients and caregivers as regulatory actors, which captures why they are acting in regulatory ways: actors by nature, actors of opportunity, and actors of necessity. We use this tripartite classification to distinguish between when participating in regulatory action is perceived as positive by patients and caregivers who are provided with opportunities to do so, or do so because it is in their nature, and situations where regulation by patients and caregivers may be indicative of system issues, potentially arising from regulatory failure. Regulatory failure, as defined by Baldwin et al, 25 refers to when regulation fails to achieve its objectives or ‘mandates’ at a reasonable cost, which in the AD context could include a failure to meet the policy goals or principles contained in the law. 26 The purpose of distinguishing between these reasons for behaving as regulatory actors is to encourage other actors in the system to be aware of why patients and caregivers are acting in regulatory ways in order to determine the appropriate response (i.e. to support and facilitate the regulatory action, or to relieve the burden of having to take the regulatory action by addressing the issue through other means).
This article first outlines the significance of AD in providing rich context to understand the regulatory role of patients and caregivers in healthcare. Next, we outline how a range of definitions of regulation may be applicable to actions by patients and caregivers and consider how the few authors who have conceived of patients and caregivers having a regulatory role conceptualise this role. We argue that although the literature is scant, there is evidence that patients and caregivers do behave as regulatory actors in various healthcare contexts, including AD, and that we should therefore conceive of patients and caregivers as being capable of regulatory action. We then propose a new framework that incorporates notions of why some patients and caregivers behave as regulatory actors and, finally, we suggest implications of our proposed framework including how it might help to determine the appropriate response by other actors (e.g. governments, healthcare institutions, and healthcare professionals) within systems.
AD provides rich context for understanding patient and caregiver regulatory action
AD refers to a situation where a person seeks assistance from a health practitioner to receive medication that will end their life. 27 AD is permissible in a small but growing number of jurisdictions globally, including Australia, Canada, New Zealand, the Netherlands, Belgium, Spain, Colombia, and some states in the United States of America and its District of Columbia. 28 Much of this legalisation has occurred recently, since 2016, 29 meaning that in most jurisdictions AD is in the early phases of legalisation or implementation. AD is referred to using different terminology around the world, including voluntary assisted dying, medical assistance in dying, euthanasia, and physician-assisted dying. 30 Each jurisdiction has a different model of AD, including different eligibility criteria and procedural safeguards. 31 AD provides rich context for understanding the regulatory role of patients and caregivers because it is new, and also because it is a (for some) controversial, politicised, and highly regulated form of end-of-life care.
The controversial nature of AD is highlighted by the vast literature scrutinising the ethics of permitting AD. 32 AD proponents often highlight the importance of promoting a person’s right to make choices about their own healthcare (i.e. their autonomy) and how AD can relieve a person’s suffering. 33 These principles are sometimes explicitly outlined as the policy goals of AD legislation, for example, in the Voluntary Assisted Dying Act 2017 (Vic) in Victoria, Australia. 34 Others argue that doctors are bound to protect life rather than to end it, and highlight the potential for coercion of vulnerable individuals into accessing AD and raise concerns about ‘slippery slopes’. 35 Ethical debates have largely been resolved in favour of permitting AD in jurisdictions where it is legal for the more straightforward AD cases, 36 such as where a person with a terminal illness makes a request and takes medication while they have capacity. However, ethical debate continues to rage in many, though not all, jurisdictions in relation to access to AD for more complex cases, such as for minors, prisoners, those with mental illness as the sole underlying medical condition, dementia, and others who would need to request AD in advance. 37 AD also faces strong opposition from powerful institutions, including religious institutions, 38 which affects the nature of debate and legalisation, 39 as well as implementation. 40
AD is regulated in different ways in the various jurisdictions where it is legal. Across jurisdictions, though, AD is a highly regulated aspect of healthcare. Particularly stark examples of this are the AD models in Australia. For example, Victoria’s law (the Voluntary Assisted Dying Act 2017 (Vic)) is 127 pages, contains ‘68 safeguards’, and was touted as being ‘the safest, and most conservative, in the world’. 41 Despite a highly prescriptive central law, other sources of regulation are also critical in influencing how AD regulation operates in practice in Victoria, such as policy, 42 training, 43 and actions of patients and caregivers. 44 Other jurisdictions, such as Belgium, have a less prescriptive framework. Belgium’s AD regulatory system is nonetheless multi-faceted and involves law, policy, and other tools and organisations beyond the state. 45 Conceptualising what is meant by ‘regulation’ and understanding who takes part in it is an important exercise, because simply focusing on the state would miss a number of key actors that impact and influence behaviour. A holistic understanding of who regulates AD is necessary if it is to be regulated as effectively as possible, 46 and it is contended that this should include considering the regulatory role of patients and caregivers.
Another unique aspect of AD, which contributes to the richness of AD in understanding the role of patients and caregivers as regulatory actors, is that the intended outcome of the process is that the patient dies. This is unique for two key reasons. The first relates to the outcome itself: choosing to die is a significant decision. There are very few other healthcare contexts in which the death of a patient is the intended result of a medical decision; conversely, it would often represent an adverse event or poor-quality care. The fact that the outcome of AD is death means that considering how AD is regulated, and who regulates it, is important because the stakes are high. As Yeung says, ‘the consequences of ineffective regulation are fatal and irreversible’ 47 and understanding holistically how regulation occurs is therefore important. A second reason is that AD results in caregivers having a significant role to play in any regulatory action. After the patient successfully accesses AD and dies, caregivers are necessarily the ones who would take action that may be conceived of as regulatory as the patient is no longer able to do so. Regulatory action may include acting in peer support roles, providing information about AD to others, or creating grief-related resources. It may also include acting to improve barriers to access that arose during the patient’s experience of AD, even though they are no longer directly barriers for the patient or caregiver. 48 These examples will be considered further below.
Before turning to consider whether patients and caregivers meet definitions of regulation and outlining the proposed new conceptual framework, we note that this theoretical research draws on the empirical foundation provided by our research conducted in the AD context in Australia and Canada, as reported in two articles we have published elsewhere. 49 These two articles report on our findings from qualitative, semi-structured interviews we conducted with Australian and Canadian patients and caregivers, respectively. They examine how patients and caregivers in Australia and Canada take action which may be conceived of regulatory, what motivates them to take such action, outcomes of actions, and factors which impact on these other three themes (such as the nature of a person’s experience, their personality and supportiveness of AD, and connections to advocacy groups or high-profile individuals/media). 50 This theoretical article analyses our earlier empirical findings in light of broader regulatory scholarship on the role of patients and caregivers in healthcare regulation and examines whether patients and caregivers are capable of being regulatory actors in healthcare more broadly. This article then seeks to articulate a new conceptual framework for understanding patients’ and caregivers’ regulatory role in healthcare regulation.
Defining regulation: can patients and caregivers be ‘regulatory actors’?
There is no single authoritative and universally agreed definition of regulation. Conversely, there are a myriad of definitions of regulation ranging from narrower definitions of regulation to broader ones. 51 Koop and Lodge identify that, despite this diversity, there is a shared conception of regulation: it involves intervention in the behaviour or activities of individual or corporate actors. 52 Koop and Lodge also identify a number of conceptual questions where scholars differ, three of which are particularly relevant to our inquiry about the regulatory role of patients and caregivers. These are whether: (1) regulation must be intentional or non-intentional; (2) regulation can be carried out by non-state actors; and (3) the regulator and regulatee need to be separate actors. 53 These questions are answered in different ways by scholars who subscribe to narrower or broader definitions.
An example of a narrower definition is that regulation is the promulgation of rules by the state, accompanied by monitoring and enforcement mechanisms, or direct state intervention. 54 Selznick’s seminal definition of regulation as ‘sustained and focused control exercised by a public agency’ 55 is a prominent example. It is self-evident that if regulation is defined in this way, patients and caregivers could not be conceived of as regulatory actors. This would not be to say that their role is irrelevant, because it is patients and caregivers who elect state representatives who make law, who directly vote on matters affecting constitutions via referenda, and who bring litigation that may affect how law is interpreted and applied. But these actions, while an important foundation for state-centred regulation, would not be sufficient to frame patients and caregivers themselves as regulatory actors. Narrower definitions are arguably insufficient in the healthcare context where it has been demonstrated that factors beyond the state and formal rules influence behaviour. 56 In the end-of-life care context, for example, evidence shows that health professionals (as well as patients and families) may be unaware of the law, or even if they are aware, not follow it, which suggests that other forces beyond law must impact on behaviour. 57
These narrower definitions can be contrasted with broader definitions which envisage a role for non-state actors. Hancher and Moran’s regulatory space theory, which underpins (but is also extended and challenged by) the approach to regulation taken in this article, accepts a role for other actors beyond the state and focuses on the interactions and power relations between regulatory actors within the regulatory arena.
58
They do, however, argue that it is generally organisations, rather than individuals, who may take on a regulatory role and that usually an individual’s ability to influence regulation is tied to their affiliation with an organisation.
59
Black’s prominent definition of regulation is an example of a broader definition which contemplates a role for non-state actors:
. . . regulation is the sustained and focused attempt to alter the behaviour of others according to defined standards and purposes with the intention of producing a broadly identified outcome or outcomes, which may involve mechanisms of standard-setting, information-gathering and behaviour modification.
60
Importantly, Black’s definition focuses on the nature of the action itself and not whether a person achieves their intended outcome. This is because the outcome does not determine whether the act is in itself regulation, just whether it is effective regulation. 61 The broadest form of definitions conceive of regulation as anything producing effects on behaviour, which could include unintentional actions by individuals that may incidentally impact others’ behaviour, the incidental effects of tools, such as laws, policies, or training, that were not specifically intended to regulate a particular issue but nonetheless impact it, or broader factors like culture. 62 These two broader categories of definition allow scope for patients and caregivers to be conceived of as regulatory actors.
There is an emerging body of literature which applies conceptions of regulation to actions by patients and caregivers, or which frames patients and caregivers as having a potentially regulatory role. Wiig et al. describe this body of literature as being in its ‘infancy’. 63 A key author who argues patients engage in regulation is Healy. 64 Healy uses Ayres’ and Braithwaite’s definition of regulation as ‘steering the flow of events’ to map the ways in which patients may steer the flow of events using a responsive regulation pyramid model. 65 At the base of Healy’s pyramid is ‘informed patients’ and at the apex is ‘aggrieved litigants’ (Figure 1). 66
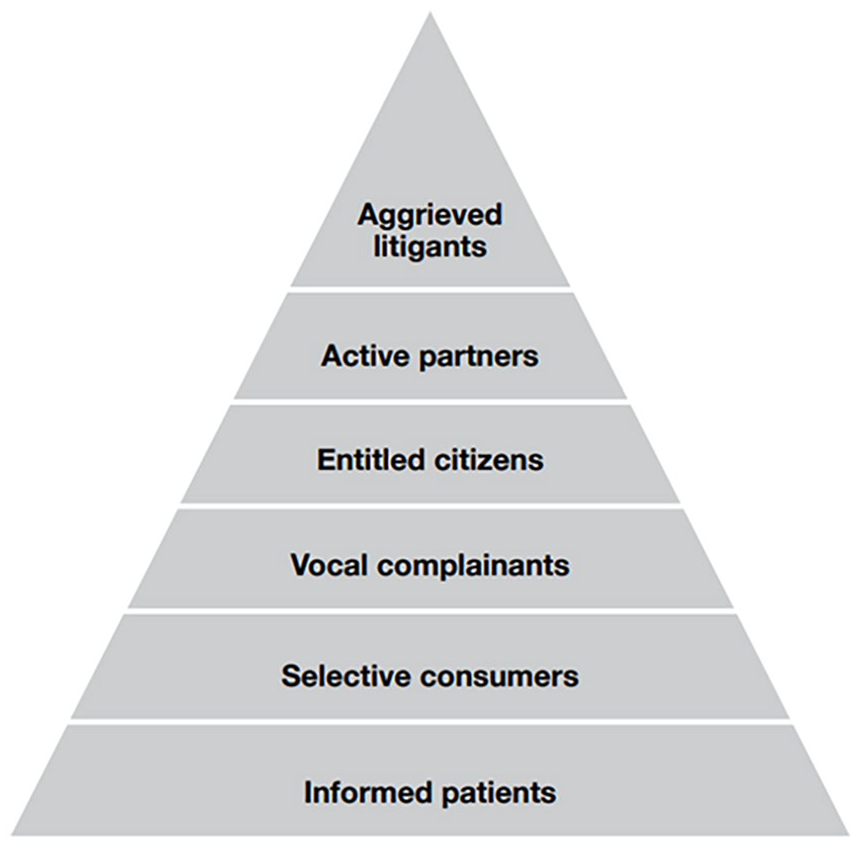
Healy’s pyramid of regulatory actions by patients and caregivers. 67
The pyramid highlights that more patients act as informed patients (this is often a legal and ethical requirement), whereas fewer would be willing to act as aggrieved litigants. 68 Our research in the AD context has found evidence of patients and caregivers being ‘informed patients’ through their knowledge about the AD system, exercising consumer choice (Healy’s ‘selective consumers’) to select individual doctors and institutions to assist them, and advocating in relation to both the AD process and their general care and treatment (Healy’s ‘active partners’). 69 Some of Healy’s categories such as ‘informed patients’ do not necessarily demonstrate intentional action to alter others’ behaviour, but Healy may consider these regulatory because these actions may nonetheless steer events or behaviour. For example, a patient providing informed consent to receive a particular treatment or to not receive it steers whether that person receives a particular treatment, and this information provision requirement may establish an extra layer of protection against adverse events meaning that an adverse event is avoided (i.e. the flow of events is steered). Other clearer examples of regulatory action by patients and caregivers in both Victorian and Canadian AD systems demonstrated by recent studies were that patients and caregivers made complaints and provided feedback (Healy’s ‘vocal complainants’), acted as consumer representatives or in consulting roles (Healy’s ‘active partners’), and undertook law reform efforts; actions which were intentionally directed at altering behaviour in AD systems more widely. 70
Another author who has considered the role of patients as regulators is Madison. 71 Madison uses a definition of regulation conceptualised specifically for the healthcare context by Mello et al., as the ‘organized and deliberate leveraging of power or authority to effect changes in the behavior of health care providers’. 72 Madison argues that the requirements of informed consent, the increasing emphasis on patient-centred care, and the rise of consumerism in healthcare provide ways in which patients can alter their relationship with their providers and systems as a whole. 73 While Madison argues that patients may resemble regulators, they are ‘not exactly’ regulators because they do not possess the same authority as a typical regulator or seek to implement broad societal goals through their actions. 74 Our recent empirical findings in the AD context challenge these conclusions in two ways. The first is that while patients and caregivers may lack the same type of authority as a typical regulator (e.g. the power to enforce sanctions), they have a different sort of authority stemming from their firsthand experience as users of systems which is also powerful and can prompt change. 75 The power of their actions is evidenced through advocacy efforts and litigation outcomes in Canada. 76 Because patients and caregivers are the central impetus for AD regulation specifically and healthcare more generally (i.e. there would be no need for healthcare without patients), their opinions on how it is working in practice matter. In addition, patients and caregivers form networks to overcome the limits of traditional notions of authority with more powerful actors, such as advocacy groups, in order to achieve their goals and can collectively exert authority in this way. 77 Although Hancher and Moran do not conceive of patients as regulators, this research supports their assertion that organisational affiliation is a powerful way for individual regulatory actors to have influence.
The second way in which recent research has challenged Madison’s conception of the role of patients and caregivers in regulation is that some patients and caregivers do seek to implement broad societal goals through their actions. Their actions in some instances related to the patient themselves and their own experience of healthcare, but often their actions were partly or wholly directed towards producing outcomes that were much broader than their own experience. 78 This is particularly obvious when considering regulatory action undertaken by a caregiver after a patient has died through AD, whose action necessarily relates to helping others beyond the patient they supported. A key motivation for patients’ and caregivers’ actions was to help others and make the system better, including by sharing information about AD so that more people know about it, helping to destigmatise it, and reducing barriers to access for others. 79 We argue that these are all clearly examples of broader societal goals. This is also reflected in other literature which reports that patients’ and caregivers’ main motivations for reporting adverse events, for example, are to improve safety and health outcomes. 80 A less common reason for making an adverse event report related to the person seeking a punishment of the health provider or compensation for themselves, 81 so the desire to address broader societal issues is not limited to the AD context.
Other scholars like Wiig et al., Adams et al., Richardson et al., and Bouwman et al. have studied the ways in which patients and caregivers are involved or engaged in regulatory processes by regulators. 82 Dolev and Benish, in their recent systematic literature review, describe this body of work as ‘participatory regulation’. 83 Participatory regulation scholars highlight the importance of patients and caregivers being involved or engaged in regulation, 84 including by being invited to make complaints, report adverse events, and be involved in investigation processes through interviews and other means. 85 Wiig et al., for example, map these methods in terms of individual versus collective, and proactive versus reactive involvement in regulation. 86 An example of an individual proactive involvement mechanism is patient surveys about recent healthcare experiences, and an individual reactive mechanism is a complaint to an ombudsman about a negative healthcare experience. 87 On the proactive collective level, Wiig et al. highlight the inclusion of patients and caregivers as consumer representatives or as part of research design. 88 An example of reactive collective response is to aggregate data from surveys or complaints. 89 It is positive that there are examples of the diverse ways in which patients and caregivers are involved in regulation by other regulatory actors. But this framing arguably separates patients and caregivers from regulators (i.e. patients and caregivers are not regulatory actors themselves but are involved in regulatory processes by regulators, such as investigators, researchers, and health organisations). We suggest that patients and caregivers can and should be conceived of as regulatory actors in their own right, not only through their participation in formal regulatory processes at the invitation of other regulators. To answer Koop and Lodge’s query about whether a regulatory and regulatee need to be separate actors, 90 we argue that a person can be both.
Like participatory regulation literature, scholarship on ‘deliberative regulation’ examines the use of methods to engage with and ‘bring people’s opinions and values into health policy processes’. 91 A scoping review by Degeling et al. found that deliberative regulation processes are common in public health and health policy research, and particularly used for assessing health technologies, resource allocation and priority setting, population health interventions, value-oriented questions, and other complex areas where there may be conflicting values. 92 Methods to engage citizens include citizens’ juries, townhall meetings, public forums, and workshops, among others, 93 which may be described as ‘regulatory actions’. However, as noted above, the framing of citizens being engaged in deliberative processes through the actions of researchers, funders, and governments arguably separates citizens and regulators, and does not highlight the ways in which citizens (including patients and caregivers) may themselves be conceived as regulatory actors. Another potential concern arising from this literature relates to who is engaged in deliberative processes. Degeling et al. found that ‘disinterested’ members of the public (i.e. people who are not personally affected by the topic of deliberation except to the extent that they are a member of the public) are more often involved in deliberative methods than experienced ‘service-users’ (i.e. patients and caregivers, or consumers of services). 94 Furthermore, the engagement of advocates, described as partisan members of the public, mostly occurred when the project related to policy discussions or decision-making bodies. 95 This preference for ‘disinterested’ members of the public stems from valid concerns about increasing legitimacy and avoiding regulatory capture. 96 However, treating individuals with personal experiences of services, such as patients and caregivers, as ‘inherently partial, situated and political’ 97 and involving them less frequently in deliberative methods may result in patients and caregivers ‘regulating’ through other, potentially more burdensome, means. The implications of this are discussed further later in this article.
Other authors have provided accounts of actions by patients and caregivers that may be conceived of as regulation, but without using the language of regulation.
98
For example, Hoffman et al.’s edited book investigates the extent to which health policy, a form of regulation, has been shaped from below as well as above, and the extent to which patient voices and actions directly influence health policy.
99
Hoffman et al. note there has been a lot of ‘lip service’ paid to the transformative power of patients, but their role and power to shape change has generally been understudied.
100
The book explores the ways in which groups of people in the United States have influenced change to health policy. These include individuals with brain injuries and their surrogate decision-makers, poorer people (and particularly, poorer Black women), pregnant women, individuals with mental illness, individuals with rare diseases, and caregivers of babies born with severe genetic abnormalities, among others.
101
In a chapter in this collection, Fairman suggests that
. . . patients can have a crucial influence on health policy on both a local and a broader national level – they can be essential actors – even when they are not acting with any notion of the public good in mind, even when they are not trying to influence policy making, and even when they are unaware of how their individual choices might impact the legitimacy of a profession.
102
A particularly striking example in Hoffman et al.’s edited book, which demonstrates that patients and caregivers do undertake significant regulatory action, is that of rare diseases. 103 Dockser Marcus describes that other regulatory actors in the rare diseases context (specifically, rare cancers) such as researchers or advocacy groups do not have incentives to become involved in finding cures or treatments for rare diseases, because it is not profitable and/or because the pool of people to benefit from such research or programmes are so small compared to other, more common disease. 104 The lack of research on treatment for rare diseases also means that people do not survive very long, resulting in an essential role for caregivers in undertaking advocacy, 105 akin to the AD context. There are examples in the rare diseases context of patients and caregivers, including the Kaufman family and the Sommers family, taking extraordinary, intentional action to prompt research into rare diseases which has had impacts such as establishing tissue and specimen banks, creating new cell lines for testing lead compounds, establishing patient registries, forming clinical trial networks, and raising significant funds. 106 This research resonates with Aymé et al.’s research into rare diseases, where the authors assert that patients in this context ‘are directly shaping their future’ including through establishing research policies and projects for rare diseases. 107 The small affected cohorts of people in the rare disease community, and the marginalisation of rare diseases, has resulted in patients and caregivers taking action to alter behaviour in the system because there is no one else with the motivation or impetus to do so. In this way, the rare diseases context is akin to AD where AD deaths represent a small number of total deaths (i.e. there is a relatively small, directly affected cohort). For example, AD represents a total of 0.65% of deaths in Victoria, Australia, 108 and 4.1% of all deaths in Canada. 109
Another example is the mental health context, where Tomes asserts that patients and caregivers have played a key role in spearheading an emphasis on recovery and rehabilitation. 110 Their actions have impacted the way that mental illness is approached, and individuals have sat on mental health councils, mental health agencies, and treatment policy committees. 111 Similarly, poorer Black women in the United States advocated for access to healthcare and told stories of the impact of poverty on their lives and medical treatment, which ultimately resulted in a bill of rights being introduced in the United States (though Hoffman asserts this was watered down, and then ultimately removed). 112 But despite the obstacles faced by poorer Black women, including lack of connections to powerful institutions and lawmakers, their activism ‘carried a particular kind of power . . . their voices could not be ignored’. 113
We argue that this evidence from a wide range of healthcare contexts, including our recent research on AD in Australia and Canada, 114 shows that patients and caregivers are indeed capable of being regulatory actors. The finding that patients and caregivers are capable of being regulatory actors holds across a myriad of definitions of regulation. Of course, it does not resonate with traditional state-centric conceptions of regulation, but there is evidence in AD and other healthcare contexts that suggests that patients and caregivers are capable of taking sustained, focused, and intentional action to alter behaviour; 115 steering the flow of events and behaviour; 116 producing effects on behaviour; 117 and acting as ‘informed patients’, ‘vocal complainants’, and ‘active partners’. 118 We must therefore recognise that some patients and caregivers are regulatory actors. To fully understand how regulation is functioning, patients and caregivers must be considered as potential regulatory actors in healthcare regulatory spaces; otherwise, a key piece of the regulatory puzzle is missed. We argue that patients and caregivers as individuals have influence beyond their affiliation with an institution (or at least is not entirely dependent on such an affiliation), and in this way, our argument extends Hancher and Moran’s regulatory space theory analysis which precludes a significant role for individual actors. 119 However, we also consider that networks of patients, caregivers, and organisations (which resonates with Hancher and Moran’s perspective on the importance of organisational affiliation) 120 are important and we discuss the implications of this in part 5.
A new framework for conceiving of why patients and caregivers behave as regulatory actors
Having argued that patients and caregivers are capable of being regulatory actors in AD and other healthcare contexts, this article now turns to consider why it is important to explicitly capture notions of why people are acting in regulatory ways in discussions of patients’ and caregivers’ regulatory role. Healy’s responsive regulation pyramid framework was a fundamental development in the literature on the regulatory role of patients and caregivers in healthcare contexts, 121 and other authors have contributed to this underdeveloped body of literature by describing what regulatory actions people may take and be involved in. 122 Existing literature also provides information about why patients and caregivers may act in regulatory ways. However, motivations for behaving as regulatory actors are not explicitly captured in existing frameworks for conceptualising their regulatory role. We argue that a framework that incorporates not only the ways in which patients and caregivers act that may be considered regulatory, but also why they act in those ways, is essential because it helps to determine the appropriate response by other regulatory actors, including state actors such as governments.
We propose a tripartite classification which explicitly incorporates notions of why people act in regulatory ways: actors by nature, actors of opportunity, and actors of necessity. We also note that some individuals may span multiple categories at once (or may shift from one category to another over time) and we refer to these individuals as hybrid actors. We describe each of these categories below and provide concrete examples of how we suggest they might apply in the AD context in Victoria, Australia. As outlined in part 2 of this article, the categories outlined below draw on the empirical research foundation provided by our research findings in the AD context, which are reported elsewhere. 123 These categories also draw on reasoning based on analysis of the wider regulatory scholarship considering the role of patients and caregivers in healthcare regulation that was outlined in part 3 of this article.
Actors by nature
The first category in our classification is ‘actors by nature’. By this, we refer to people who by their nature want to take action to influence behaviour (i.e. regulate). This category of actors by nature resonates with the evidence of individuals in the AD context acting in particular ways because it was inherent in their personality and values to do so. 124 For example, as reported in our recent research, an individual who had an experience of AD in Canada explained that being involved in activism and advocacy was ‘just who I am’, 125 and an Australian caregiver described wanting to be an ‘agent of change’ for AD in Australia. 126 Caregivers in the AD context have also self-described having personality characteristics such as being assertive, a ‘solver and a doer’, ‘a bulldog’, or being ‘outspoken’, and many reported a long-standing connection to an advocacy group as being reflective of their inherent values and personality. 127 For actors by nature, being involved in actions to improve the status quo is just who they are.
Actors of opportunity
The second category is ‘actors of opportunity’. Here, we refer to people who are engaged in regulatory action by the efforts of other regulatory actors in the system. For example, in the AD context, they may be asked to act as a consumer representative on a committee, asked by an advocacy organisation to speak about an issue publicly, or invited to provide feedback by an AD oversight body (e.g. in Victoria, Australia, the Voluntary Assisted Dying Review Board).
128
We also clarify that we do not just mean that a person has an opportunity to become an actor by virtue of having a particular experience, such as supporting someone to access AD, but rather that additional opportunities for involvement in regulatory action have been presented to them by other actors in the AD system (such as governments, healthcare institutions, or healthcare professionals), which they have taken. Actors in this category would not have initiated regulatory action themselves without the engagement of others: they are prompted into action. An example of this, reported in our recent research, is a person who undertook regulatory action in Australia after being prompted to do so by an AD advocate. The person’s family caregiver described, in relation to the patient undertaking advocacy, that ‘. . . she was also asked to speak to the [state] Parliament, which she did . . . How did that come about? Through [VAD advocate] I think’.
129
A second example of this in the Australian AD context, reported in our research, is a patient whose experience was reported in a newspaper article:
. . . the article that was printed in the [newspaper], that came about by [VAD advocate] in talking to me knew that a journalist was coming that wanted to interview him . . . to write an article because of the impending possible legislation in [another state] from VAD. He understood she wanted to write articles which would help them make the right sort of legislation and obviously particularly in relation to prognosis. It was through her coming down from [another state] to meet him that he got her to come out and meet me as what he saw as a typical case that would fall through the cracks because of the Victorian legislation with the prognosis problem.
130
In addition to evidence in the AD context of people responding to opportunities presented to them to undertake action, 131 this category also resonates with many of the examples provided by Wiig et al., Adams et al., Richardson et al., and Bouwman et al. of strategies for engaging patients and caregivers in regulatory processes, 132 described by Dolev and Benish as participatory regulation. 133 For example, Wiig et al. describe strategies such as sending surveys to people who have had a healthcare encounter, inviting people onto committees, or seeking their feedback on recent healthcare experiences. 134 Deliberative regulation methods, such as citizens juries or townhall meetings, provide other examples of patients and caregivers responding to opportunities to be involved in regulatory action. 135
Actors of necessity
The third category is ‘actors of necessity’. Here, we refer to people who take on a regulatory role out of necessity. This might be because they encountered barriers to access in their experience of healthcare, or there is a perceived gap in the system they are seeking to address. By ‘a gap in the system’, we refer to an issue that is not addressed through law or appropriately addressed through policy, or a resource or service that does not exist. People may also take on a regulatory role out of necessity because there is a barrier to access or a roadblock that a person experiences which they seek to address or resolve, such as an eligibility criterion that is perceived to be overly restrictive, a procedural safeguard which is perceived to hamper access but not increase safety, or a policy that is perceived to be a barrier, unjust or harmful. 136 These individuals may act to fill the gap or overcome the barrier for the benefit of the patient they support, themselves, or for the benefit of others. 137 We conceive of the term ‘necessity’ broadly and include actions taken by a caregiver after a person has died. While taking action to address barriers to access may no longer be necessary to achieve AD access (or access to another healthcare service) for the individual patient, barriers may remain for others and the notion of necessity therefore includes the goal of acting to reduce barriers or gaps for others in the future. This may be due to feelings of a ‘moral obligation’ to help others or to make the system better because they are aware of issues due to their experience as system users. 138
Although the concept of necessity implies a sense of compulsion to act, this is not to say that a person is not acting intentionally (and therefore does not meet definitions of regulation that include an intention to act, such as Black’s). 139 Schlesinger makes this distinction aptly in a chapter from Hoffman et al.’s edited collection, in which he draws an analogy between patients and canaries in a coalmine. He writes that canaries, after being faced with noxious gases, ‘didn’t decide whether to keel over – it just came naturally’. 140 However, in response to experiencing barriers to access or gaps in AD regulation, patients and families must actively ‘decide whether it’s worth the effort to voice their dissatisfaction . . . motivation will depend in part on their sense of connectedness and obligation to future patients’. 141 The choice to act in the face of system issues demonstrates intentionality of action.
We suggest that individuals are more likely to be drawn into this category of actors of necessity if their experience of healthcare relates to a healthcare service that is new, where there are political dimensions or power imbalances, where the illness or treatment/care is stigmatised, there is a small cohort affected or the affected cohort is marginalised, or where there is regulatory failure (i.e. regulation is not achieving its mandates, such as policy goals or principles).
142
This resonates in the AD context, which is a new healthcare service in Australia and Canada. For example, as reported in our recent research on AD in Australia, one participant stated the following:
. . . I’m hoping that people’s experiences [of institutional disorganisation] now will be nothing like what ours were, but it was purely and simply because of the maturity of the system that we were working within at that time . . . that’s probably why I participated in some of those media opportunities, was to try to get the people to be aware, to be thinking of it, to start those conversations so that it wasn’t . . . trying to sort through this murky system of ‘but I’ve asked three doctors’, ‘Oh, I’ve got to go home to get the medication. I’m not ready yet’. . . . all these little things I think was around the maturity of the VAD.
143
AD is also a controversial and politicised health service, with individuals reporting a need for AD to be destigmatised. 144 There are also power imbalances between individual patients (who are predominantly terminally or grievously and irremediably ill and experiencing intolerable suffering) and other actors in the AD system, over and above general power imbalances. For example, there is a power imbalance between individual doctors and patients due in part to the ‘esoteric nature of medical expertise’. 145 In addition, many healthcare organisations hold objections to AD on the basis of organisational values, such as faith or a palliative care philosophy, and prevent some or all aspects of AD happening on their premises. 146 As an example from our recent research, one Canadian family caregiver participant described efforts to alter the stance held by the long-term care facility where the patient resided about allowing AD onsite: ‘ . . . it was about making a path for people to be able to access this safe, comforting, incredibly helpful medical procedure. It wasn’t just about [patient] . . . .’. 147
This category of actors of necessity also resonates with other examples reported in Hoffman et al.’s edited collection where patients and caregivers have undertaken action to shape change. 148 For example, it resonates with the rare diseases context because the political dimensions mean that it may not be profitable for others to take action to address issues such as undertaking research, and the affected cohort is very small. 149 This creates a necessity for patients and caregivers to take action to generate progress into research and cures because no one else is doing so. Similarly, poorer people in the United States, particularly poorer Black women, needed to take action to draw attention to the impacts of poverty on healthcare due to the marginalisation they were experiencing, the stigmatisation of not being able to afford healthcare, and the political and power dimensions in American societies including systemic racism and inequality, 150 because if they did not these issues would not be on the political agenda. Tomes asserts that progress made by advocates in the mental health space has occurred despite mental illness being a highly stigmatised disability, 151 but perhaps it has occurred precisely because of this stigmatisation and the consequent necessity for those affected to take action to create change.
Hybrid actors
We also recognise that there may be examples of regulatory action occurring across more than one category. For example, we suggest that an individual may have initially started taking action because of opportunities presented to them but they may find it is part of their nature to advocate in relation to AD or they may seek out further opportunities to act on their own initiative. As an example from our AD research in Canada, one participant who was approached by the media to do a story about her experience of AD (i.e. an actor of opportunity) then became involved in providing information more broadly to many other people, participating in research projects, and joining networks of other advocates (arguably becoming an actor by nature). 152 A person may also cease to become a regulatory actor altogether. This may be for various reasons including that they have achieved their goals (e.g. if the legal barrier is lifted or the gap in the system is filled), that they have not achieved their goals despite concerted efforts and feel deflated about progress, because the emotional or financial burdens of acting in regulatory ways are too great, that they successfully access AD, or other reasons. As an example from our research in the Canadian AD context, one family caregiver noted that: ‘I really grappled with actually giving some pretty serious feedback . . . But . . . you’re emotionally drained . . . in the end you decide to just let it go’. 153 Another family caregiver in the Australian AD context described concerted advocacy efforts to change an eligibility criterion for AD access. The participant talked about wanting ‘get this monkey off my back’ so that they could move on with their life, 154 suggesting that their regulatory efforts were directed at, and would cease upon achievement of, a specific goal. There is therefore fluidity about exactly who is in the regulatory space at any given time and why they may be in the regulatory space.
Key implications of findings and proposed conceptual framework
There are two key implications of the findings in this article. The first relates to the role of patients and caregivers as regulatory actors in healthcare and the novel nature of such a claim. The second relates to the implications of the proposed conceptual framework outlined in part 4.
Patients and caregivers are capable of being regulatory actors
The framework proposed outlined in part 4 is premised on the finding that patients and caregivers are capable of being regulatory actors in healthcare regulatory spaces. This in itself is a novel claim to make, given that the body of scholarship on patients and caregivers as regulatory actors is scant as described in part 3, and that whether patients and caregivers are capable of having a regulatory role has been contested. 155 This article makes a novel contribution by drawing together theoretical literature and empirical research provided in relation to the AD context, 156 to argue that patients and caregivers are capable of being regulatory actors (both in AD and broader healthcare contexts) according to a range of decentred definitions of regulation, including through undertaking sustained and focused attempts to alter behaviour. 157
While our findings challenge Hancher and Moran’s assertions that individuals do not regulate, we also agree that organisations have an important role to play and can increase the influence of patients’ and families’ actions. Notwithstanding that patients and caregivers may act as regulatory actors independently of their organisational affiliation, networks of regulation formed by patients and caregivers with other actors, including organisational actors, are important. This is demonstrated in the AD context, with our previous findings demonstrating that having a connection to an advocacy group, high-profile individual, researcher or research group, or media is a key factor impacting patients’ and caregivers’ actions and motivations, as well as the outcomes they can achieve. 158 A concrete example of this in the AD context is the case of Audrey Parker who, together with her friends and Dying With Dignity Canada (a patient advocacy organisation), sustained a campaign which ultimately resulted in the Canadian AD law being changed. 159 This is reflected in the legal change being referred to commonly as ‘Audrey’s Amendment’. 160 Similarly, patients and caregivers have been key actors litigating to influence law reform about AD in Canada in several key cases. 161 While these individuals should be perceived of as actors in their own right who acted to ‘change the law of the land’ through litigation, 162 civil liberties organisations, advocacy groups, academics, and others were also key actors who joined with patients and caregivers to achieve this change. 163 This resonates with Hoffman et al.’s comments in relation to advocacy by poorer Americans. Hoffman et al. state that ‘without powerful allies, greater resources, or a long-term organizational strategy, their voice and influence could not be sustained’. 164 Therefore, while we assert that patients and caregivers are capable of being regulatory actors in their own right, this article also recognises the importance of organisational actors partnering with patients and caregivers to achieve change and continuing influence.
Implications of tripartite conceptual framework
A key implication of our proposed tripartite conceptual framework is that it helps to distinguish when undertaking regulatory action by a patient or caregiver is a positive reaction to their experience from when they may perceive it is required of them because the system is not working effectively or achieving its intended goals. This then determines what the response should be. If people are acting because it is their nature to do so and they want to, this is positive and it should be supported and appropriately responded to. By this we mean that other regulatory actors (e.g. governments, healthcare institutions, and health professionals) should facilitate continued regulatory action, and, where this action highlights aspects of regulation that are not functioning effectively, they should take steps to address this to ensure healthcare systems are meeting their intended goals. Grob argues that the health care system ‘badly needs patients’ to be part of health policy development and call for the system to be ‘responsive to those who have the courage to sacrifice harmony and give voice to both their experience and their convictions’.
165
Health systems should capitalise on existing opportunities to involve patients and caregivers in regulation.
166
Similarly, if people are acting because they are provided with opportunities and enthusiastically take on those opportunities, that is also a good thing, and should continue to be facilitated. However, we consider that other actors should go beyond this to proactively provide opportunities for patients and caregivers to be involved in regulation if they wish to be. We agree with Hoffman et al.’s call for further opportunities to be created for inclusion of patients and caregivers in regulation:
. . . the stakes for full inclusion of patients in policy making are so high that more must be done than to simply make room at the table for those who spontaneously move from service recipient or citizen to policy activist. Indeed, we must go beyond mere responsiveness . . . to proactive solicitation of broad and democratic participation. Put another way, those with the most power to shape health policy have a duty not only to listen to what they are being told but also to ask, in various ways, for the perspective of those who may not be first to voluntarily stand up and speak.
167
Notwithstanding the importance of engaging those who act because it is their nature and creating opportunities to act, we argue that where people are acting out of necessity to fill system gaps or address barriers to access, then this may suggest that the system is not working effectively. Other regulatory actors (e.g. governments, healthcare institutions, and healthcare professionals) need to not only listen to what patients and caregivers are saying, but to proactively solicit patient and family perspectives and act to address system issues (e.g. barriers to access or gaps in regulation). This would help to relieve the burden of patients and caregivers who act out of necessity to overcome identified system issues, such as access barriers or regulatory gaps. Literature which highlights the bases for involving patients and caregivers and the benefits of it may sometimes overlook that not all patients want to take on this role. 168 Regulation is not an easy role to undertake. It may be taxing, both emotionally and financially. It may also be a role that people, because of illness or other barriers, cannot take on. This may mean that they miss out on their chosen healthcare option or have a negative experience because of the gaps or barriers they face. It may also have a continuing negative effect for caregivers. For example, if they bring litigation after the person has died, this is likely to be financially costly and emotionally draining.
Where a person is acting out of necessity, this should be a red flag to other regulatory actors in the space and may suggest that they should step in to relieve the burden on patients and caregivers of having to undertake actions to address those barriers or gaps. This is not to suggest that patients and caregivers should no longer be involved in regulation at all – they should be involved if they wish to be – but that other regulatory actors should seek to reduce the necessity of regulation and instead provide opportunities. This may result in a person shifting from being an actor of necessity to an actor of opportunity. To provide a concrete example, governments and other organisational actors could reduce the burden of undertaking litigation from patients and caregivers by taking on the litigation themselves (i.e. acting as plaintiffs or applicants) and involving patients and caregivers as witnesses. While it is acknowledged that it would not be possible to respond to all patient and family suggestions for change, where patient and family action is necessitated because of system issues or regulatory failure (i.e. the healthcare system is failing to achieve its policy goals or principles), 169 it is incumbent on others to act. In the context of AD, key actors who must act to address gaps or barriers (or address regulatory failure) include government decision-makers who are responsible for the continued implementation and functioning of AD systems. It may also include healthcare institutions and organisational decision-makers, formal medical and nursing regulatory bodies or representative organisations, and individual healthcare professionals, who have the power to impact the delivery of AD. Therefore, we argue it is incumbent on other regulatory actors to examine why a person is acting, and where appropriate, other actors should address the barrier or gap themselves through other means.
Conclusion
This article makes two significant contributions. The first is that it demonstrates how patients and caregivers are capable of being regulatory actors, applying conceptions of regulation as defined by key scholars in the field. It also provides concrete examples of some of the ways in which they have behaved as regulatory actors in various healthcare contexts, including AD. Patients and caregivers have historically been excluded from being considered as regulatory actors within the various healthcare regulatory spaces. But overlooking the regulatory role of patients and caregivers is to miss a key part of the regulatory puzzle. Patients and caregivers are capable of being regulatory actors in their own right (though also as part of networks with organisations and other actors) and this is important to recognise. The second significant contribution of this article is the proposed framework for understanding why patients and caregivers behave as regulatory actors. It demonstrates that understanding why patients and caregivers behave as regulatory actors in healthcare regulatory spaces is key in distinguishing how systems should respond to their regulatory actions. Patients’ and caregivers’ voices and actions are valuable. Their actions should be supported and encouraged if a person wants to act in regulatory ways or it is in their nature to do so. Opportunities for involvement in regulation should be created by other actors within the system, such as government decision-makers. However, when patients and caregivers are in a regulatory space out of necessity, for example, because they are acting to address system issues or because there has been regulatory failure (i.e. a failure to achieve the goals of the system), other regulatory actors in systems – particularly governments and governmental decision-makers – should act to relieve the burden from patients and caregivers of acting to address system issues.
Footnotes
Acknowledgements
This research draws on the empirical foundation provided in other research articles, published elsewhere, which reported on qualitative interviews we conducted with patients and family caregivers in Australia and Canada about their experiences of assisted dying. We gratefully acknowledge the participants in those interviews and thank them for generously sharing their stories.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: L.W. and B.P.W. were engaged by three Australian state governments (Victoria, Western Australia, and Queensland) to develop the legislatively mandated training for providers of assisted dying in those states. R.J. and E.C. were employed on these projects. L.W. is a member of the Voluntary Assisted Dying Review Board, the oversight body in Queensland, Australia. B.P.W. is a member of the Queensland Civil and Administrative tribunal, which has jurisdiction over some matters related to assisted dying.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Australian Government, Australian Research Council Future Fellowship (project number FT190100410: Enhancing End-of-Life Decision-Making: Optimal Regulation of Voluntary Assisted Dying). The funder did not participate in or influence this research.
1.
As discussed further throughout this article, there is growing acknowledgement of the importance of eliciting patient and caregiver views on healthcare and health policy design and evaluation. For example, ‘deliberative regulation’ scholarship highlights the importance of engaging citizens in health policy design: see, for example, C. Degeling, Stacy. M. Carter and L. Rychetnik, ‘Which Public and Why Deliberate? A Scoping Review of Public Deliberation in Public Health and Health Policy Research’, Social Science & Medicine 131 (2015), pp. 114–121; J. Abelson, E. Blacksher, K. Li, Boesvel, and S. Goold, ‘Public Deliberation in Health Policy and Bioethics: Mapping an Emerging, Interdisciplinary Field’, Journal of Public Deliberation 29(1) (2013), Article No. 5.
2.
J. Black, ‘Critical Reflections on Regulation’, Australian Journal of Legal Philosophy 27 (2002), p. 11.
3.
L. Hancher and M. Moran, ‘Organizing Regulatory Space’ in L. Hancher and M. Moran, eds., Capitalism, Culture, and Economic Regulation (New York: Clarendon Press, 1989), pp. 271–299.
4.
Black, ‘Critical Reflections’, p. 15.
5.
R. Baldwin, C. Scott, and C. Hood, ‘Introduction’ in R. Baldwin, C. Scott, and C. Hood, eds., A Reader on Regulation (Oxford: Oxford University Press, 1998), p. 4.
6.
J. Healy, Improving Healthcare Safety and Quality: Reluctant Regulators (New York: Ashgate Publishing Ltd., 2011), pp. 59–96.
7.
Black, ‘Critical Reflections’, p. 26.
8.
See, for example, Degeling et al., ‘Which Public and Why Deliberate?’; Abelson et al., ‘Public Deliberation’; C. A. Vincent and A. Coulter, ‘Patient Safety: What about the Patient?’, Quality and Safety in Health Care 11(1) (2002), p. 76; A. H. Krist, S. T. Tong, R. A. Aycock, and D. R. Longo, ‘Engaging Patients in Decision-Making and Behavior Change to Promote Prevention’, Information Services & Use 37(2) (2017) pp. 105–122; E. Sutton, H. Eborall, and G. Martin, ‘Patient Involvement in Patient Safety: Current Experiences, Insights from the Wider Literature, Promising Opportunities?’, Public Management Review 17(1) (2015), p. 73; E. M. Castro, T. Van Regenmortel, K. Vanhaecht, W. Sermeus, and A. Van Hecke, ‘Patient Empowerment, Patient Participation and Patient-Centeredness in Hospital Care: A Concept Analysis Based on a Literature Review’, Patient Education and Counseling 99 (2016), p. 1924; J. Støren Sagen, G. Smedslund, A. E. Simonsen, A. Habberstad, I. Kjeken, H. Dagfinrud, and R. H. Moe, ‘Patient Engagement in the Development and Delivery of Healthcare Services: A Systematic Scoping Review’, BMJ Open Quality 12 (2023), p. 2; Y. Bombard, G. R. Baker, E. Orlando, C. Fancott, P. Bhatia, S. Casalino, K. Onate, J. L. Denis, & M. P. Pomey, ‘Engaging Patients to Improve Quality of Care: A Systematic Review’, Implementation Science 13(1) (2018), p. 2; V. Dukhanin, R. Topazian, and M. DeCamp, ‘Metrics and Evaluation Tools for Patient Engagement in Healthcare Organization- and System-Level Decision-Making: A Systematic Review’, International Journal of Health Policy and Management 7(10) (2018), p. 889; J. Ocloo and R. Matthews, ‘From Tokenism to Empowerment: Progressing Patient and Public Involvement in Healthcare Improvement’; BMJ Quality & Safety 25 (2016), p. 626.
9.
Hancher and Moran, ‘Organizing Regulatory Space’, pp. 271–299.
10.
Hancher and Moran, ‘Organizing Regulatory Space’, pp. 271, 277.
11.
Hancher and Moran, ‘Organizing Regulatory Space’.
12.
Hancher and Moran, ‘Organizing Regulatory Space’, p. 277.
13.
Hancher and Moran, ‘Organizing Regulatory Space’, pp. 277–278.
14.
B. Hoffman, N. Tomes, R. Grob, and M. Schlesinger, eds., Patients as Policy Actors: A Century of Changing Markets and Missions (New Brunswick, NJ: Rutgers University Press, 2011); Krist et al., ‘Engaging Patients’, p. 106; A. Lefkowitz, J. Vizza, and A. Kuper, ‘Patients as Experts in the Illness Experience: Implications for the Ethics of Patient Involvement in Health Professions Education’, Journal of Evaluation in Clinical Practice 28(5) (2022), p. 795; Vincent and Coulter, ‘Patient Safety’, p. 76; M. do Rosário Dias, ‘Is the Oncology Patient a Participant Actor?: Designing Psychosocial Profiles’, Psychology in Russia: State of the Art 7(3) (2014), pp. 50–65; E. M. Castro, T. Van Regenmortel, W. Sermeus, and K. Vanhaecht, ‘Patients’ Experiential Knowledge and Expertise in Health Care: A Hybrid Concept Analysis’, Social Theory & Health 17(3) (2019), p. 308; Bombard et al., ‘Engaging Patients’, p. 2.
15.
Hancher and Moran, ‘Organizing Regulatory Space’, pp. 286–287.
16.
R. Jeanneret, E. Close, L. Willmott, and B. White, ‘“Regulatory Action” by Patients and Family Caregivers to Overcome Barriers to Accessing Voluntary Assisted Dying: A Qualitative Study in Victoria, Australia’, University of New South Wales Law Journal 47(3) (2024), pp. 705–743. R. Jeanneret, E. Close, J. Downie, L. Willmott, and B. P. White, ‘“My Advocacy Is Not about Me, My Advocacy Is about Canadians”: A Qualitative Study of How Caregivers and Patients Influence Regulation of Medical Assistance in Dying in Canada’, Medical Law Review 32(3) (2024), pp. 301–335.
17.
Jeanneret et al., ‘Regulatory Action’; Jeanneret et al., ‘My Advocacy Is Not about Me’; Hoffman et al., Patients as Policy Actors; J. Healy, ‘Patients as Regulatory Actors in Their Own Health Care’ in P. Drahos, ed., Regulatory Theory (Canberra, ACT, Australia: ANU Press, 2017), pp. 591–609; Healy, Improving Healthcare, pp. 283–306; S. Wiig, S. Rutz, A. Boyd, K. Churruca, S. Kleefstra, C. Haraldseid-Driftland, J. Braithwaite, J. O’Hara, and H. van de Bovenkamp, ‘What Methods Are Used to Promote Patient and Family Involvement in Healthcare Regulation? A Multiple Case Study across Four Countries’, BMC Health Services Research 20(1) (2020), p. 616; R. Bouwman, M. Bomhoff, P. Robben, and Friele, ‘Patients’ Perspectives on the Role of Their Complaints in the Regulatory Process’, Health Expectations 19(2) (2016), pp. 483–496; S. A. Adams, H. van de Bovenkamp, and P. Robben, ‘Including Citizens in Institutional Reviews: Expectations and Experiences from the Dutch Healthcare Inspectorate’, Health Expectations 18(5) (2015), pp. 1463–1473; J. Case, M. Walton, R. Harrison, E. Manias, R. Iedema, and J. Smith-Merry 5, ‘What Drives Patients’ Complaints About Adverse Events in Their Hospital Care? A Data Linkage Study of Australian Adults 45 Years and Older’, Journal of Patient Safety 17(8) (2021), pp. e1622–e1632.
18.
R. Baldwin, M. Cave, and M. Lodge, Understanding Regulation: Theory, Strategy, and Practice, 2nd ed. (Oxford: Oxford University Press, 2011), pp. 68–82.
19.
Jeanneret et al., ‘Regulatory Action’; Hoffman et al., Patients as Policy Actors; S. Aymé, A. Kole, and S. Groft, ‘Empowerment of Patients: Lessons from the Rare Diseases Community’, The Lancet 371(9629) (2008), pp. 2048–2051; Jeanneret et al., ‘My Advocacy Is Not about Me’.
20.
Deliberative regulation processes, such as ‘citizens juries’ provide an example of how patients and caregivers (and other citizens) can be included in health policy design and evaluation. See, for example, Degeling et al., ‘Which Public and Why Deliberate?’; Abelson et al., ‘Public Deliberation’.
21.
Sutton et al., ‘Patient Involvement in Patient Safety’, pp. 73–74; Hoffman et al., Patients as Policy Actors; Lefkowitz et al., ‘Patients as Experts’, p. 795; K. H. Chuong and K. C. O’Doherty, ‘Participatory Governance in Health Research: Patients and Publics as Stewards of Health Research Systems’ in Graeme Laurie, Edward Dove, Agomoni Ganguli-Mitra, Catriona McMillan, Emily Postan, Nayha Sethi, Annie Sorbie, eds., The Cambridge Handbook of Health Research Regulation, 1st ed. (Cambridge: Cambridge University Press, 2021), p. 122; S. R. Arnstein, ‘A Ladder Of Citizen Participation’, Journal of the American Institute of Planners 35(4) (1969), pp. 216–224.
22.
Sutton et al., ‘Patient Involvement in Patient Safety’, p. 73; Hoffman et al., Patients as Policy Actors; Chuong and O’Doherty, ‘Participatory Governance’, pp. 121–122.
23.
Castro et al., ‘A Concept Analysis Based on a Literature Review’, p. 1924; Bombard et al., ‘Engaging Patients’, p. 2; Lefkowitz et al., ‘Patients as Experts’, pp. 794–800; Castro et al., ‘Patients’ Experiential Knowledge’, pp. 307–330; Aymé et al., ‘Empowerment of Patients’, p. 2048.
24.
Healy, ‘Patients as Regulatory Actors in Their Own Health Care’, p. 592; Lefkowitz et al., ‘Patients as Experts’, p. 795.
25.
Baldwin et al., Understanding Regulation, p. 69.
26.
See, for example, B. P. White, K. Del Villar, E. Close, and L. Willmott, ‘Does the Voluntary Assisted Dying Act 2017 (Vic) Reflect Its Stated Policy Goals?’, University of New South Wales Law Journal 43(2) (2020), pp. 417–451.
27.
See, for example, S. Mroz, S. Dierickx, L. Deliens, J. Cohen, and K. Chambaere, ‘Assisted Dying Around the World: A Status Quaestionis’, Annals of Palliative Medicine 10(3) (2021), p. 3541.
28.
J. Cohen and K. Chambaere, ‘Increased Legalisation of Medical Assistance in Dying: Relationship to Palliative Care’, BMJ Supportive & Palliative Care 13 (2022), p. 179.
29.
Cohen and Chambaere, ‘Increased Legalisation’, p. 179.
30.
Mroz et al., ‘Assisted Dying Around the World’, p. 3541.
31.
E. Buriticá-Arango and J. Guillermo Agón-López, ‘Eutanasia y Suicidio Asistido: Un Análisis de Derecho Comparado’, Boletín Mexicano de Derecho Comparado 164 (2023), pp. 37–61.
32.
See, for example, M. Cholbi and J. Varelius, eds., New Directions in the Ethics of Assisted Suicide and Euthanasia), vol. 64 (Cham: Springer, 2015); E. Jackson and J. Keown, Debating Euthanasia (London: Bloomsbury Publishing, 2011); B. Pesut, M. Greig, S. Thorne, J. Storch, M. Burgess, C. Tishelman, K. Chambaere, and R. Janke, ‘Nursing and Euthanasia: A Narrative Review of the Nursing Ethics Literature’, Nursing Ethics 27(1) (2020), pp. 152–167.
33.
Cholbi and Varelius, New Directions; A. Fontalis, E. Prousali and K. Kulkarni, ‘Euthanasia and Assisted Dying: What Is the Current Position and What Are the Key Arguments Informing the Debate?’, Journal of the Royal Society of Medicine 111(11) (2018), pp. 407–413.
34.
See, for example, Voluntary Assisted Dying Act 2017 (Vic), s 5; White et al., ‘Stated Policy Goals’, pp. 417–451.
35.
Jackson and Keown, Debating Euthanasia; J. Keown, Euthanasia, Ethics and Public Policy: An Argument against Legalisation, 2nd ed (Cambridge University Press, 2018).
36.
U. Schuklenk, ‘New Frontiers in End-of-Life Ethics (and Policy): Scope, Advance Directives and Conscientious Objection’, Bioethics 31(6) (2017), p. 422.
37.
See, for example, Cholbi and Varelius, New Directions; Special Joint Committee on Medical Assistance in Dying, Medical Assistance in Dying in Canada: Choices For Canadians (Final Report, 44th Parliament, 1st Session, February 2023), available at https://www.parl.ca/Content/Committee/441/AMAD/Reports/RP12234766/amadrp02/amadrp02-e.pdf; Expert Panel on MAiD and Mental Illness, Final Report of the Expert Panel on MAiD and Mental Illness (Final Report, May 2022), available at ![]() .
.
38.
I. Ciornei, E.-M. Euchner, M. Preisner, and I. Yesil, ‘Regulatory Intermediaries and Value Conflicts in Policy Implementation: Religious Organizations and Life-and-Death Policies in Belgium’, Regulation & Governance, 17(4) (2022), pp. 1076–1093.
39.
A. McGee, K. Purser, C. Stackpoole, B. White, L. Willmott, and J. Davis, ‘Informing the Euthanasia Debate: Perceptions of Australian Politicians’, University of New South Wales Law Journal 41(4) (2018), pp. 1368–1417.
40.
E. Close, R. Jeanneret, J. Downie, L. Willmott, and B. P White, ‘A Qualitative Study of Experiences of Institutional Objection to Medical Assistance in Dying in Canada: Ongoing Challenges and Catalysts for Change’, BMC Medical Ethics 24(1) (2023), p. 71; B. White, R. Jeanneret, E. Close, and L. Willmott, ‘The Impact on Patients of Objections by Institutions to Assisted Dying: A Qualitative Study of Family Caregivers’ Perceptions’, BMC Medical Ethics 24(1) (2023), p. 22.
41.
R. McDougall and B. Pratt, ‘Too Much Safety? Safeguards and Equal Access in the Context of Voluntary Assisted Dying Legislation’, BMC Medical Ethics 21 (2020), p. 1.
42.
E. Close, L. Willmott and B. P. White, ‘Regulating Voluntary Assisted Dying Practice: A Policy Analysis from Victoria, Australia’, Health Policy 125(11) (2021), pp. 1455–1474.
43.
44.
Jeanneret et al., ‘Regulatory Action’.
45.
M. Archer, L. Willmott, K. Chambaere, L. Deliens, and B. P. White, ‘Mapping Sources of Assisted Dying Regulation in Belgium: A Scoping Review of the Literature’, OMEGA–Journal of Death and Dying (2023) (early online), available at https://journals.sagepub.com/doi/full/10.1177/00302228231210146?rfr_dat=cr_pub++0pubmed&url_ver=Z39.88-2003&rfr_id=ori%3Arid%3Acrossref.org
46.
B. P. White, L. Willmott and E. Close, ‘Better Regulation of End-of-Life Care: A Call for a Holistic Approach’, Journal of Bioethical Inquiry 19 (2022), pp. 683–693.
47.
K. Yeung, ‘Regulating Assisted Dying’, King’s Law Journal 23(2) (2012), p. 166.
48.
Jeanneret et al., ‘Regulatory Action’; Jeanneret et al., ‘My Advocacy Is Not about Me’.
49.
Jeanneret et al., ‘Regulatory Action’; Jeanneret et al., ‘My Advocacy Is Not about Me’.
50.
Jeanneret et al., ‘Regulatory Action’; Jeanneret et al., ‘My Advocacy Is Not about Me’.
51.
Black, ‘Critical Reflections’; C. Koop and M. Lodge, ‘What Is Regulation? An Interdisciplinary Concept Analysis’, Regulation & Governance 11(1) (2017), pp. 95–108.
52.
Koop and Lodge, ‘What is Regulation?’, pp. 96–97.
53.
Koop and Lodge, ‘What is Regulation?’, p. 97.
54.
Black, ‘Critical Reflections’, p. 11.
55.
P. Selznick, ‘Focusing Organisational Research on Regulation’ in R. G. Noll, ed., Regulatory Policy and the Social Sciences (Berkeley, CA: University of California Press, 1985), p. 363.
56.
Healy, Improving Healthcare, pp. 59–96; White et al., ‘Better Regulation of End-of-Life Care’, pp. 683–693.
57.
White et al., ‘Better Regulation of End-of-Life Care’, pp. 683–693.
58.
Hancher and Moran, ‘Organizing Regulatory Space’, pp. 271–299.
59.
Hancher and Moran, ‘Organizing Regulatory Space’, pp. 286–287.
60.
Black, ‘Critical Reflections’, p. 26.
61.
Black, ‘Critical Reflections’, p. 26.
62.
Black, ‘Critical Reflections’, p. 11; Baldwin et al., ‘Introduction’, p. 4.
63.
Wiig et al., ‘What Methods Are Used to Promote Patient and Family Involvement’, p. 2.
64.
Healy, ‘Patients as Regulatory Actors in Their Own Health Care’, p. 594; Healy, Improving Healthcare, pp. 283–306.
65.
Healy, ‘Patients as Regulatory Actors in Their Own Health Care’, pp. 591–609.
66.
Healy, ‘Patients as Regulatory Actors in Their Own Health Care’, pp. 594.
67.
Healy, ‘Patients as Regulatory Actors in Their Own Health Care’, pp. 594.
68.
Healy, ‘Patients as Regulatory Actors in Their Own Health Care’, pp. 594–596.
69.
Jeanneret et al., ‘Regulatory Action’.
70.
Jeanneret et al., ‘My Advocacy Is Not about Me’.
71.
K. Madison, ‘Patients as “Regulators”?: Patients’ Evolving Influence Over Health Care Delivery’, Journal of Legal Medicine 31(1) (2010), pp. 9–34.
72.
Madison, ‘Patients as “Regulators”?’, p. 9.
73.
Madison, ‘Patients as “Regulators”?’, pp. 11–21.
74.
Madison, ‘Patients as “Regulators”?’, p. 34.
75.
Jeanneret et al., ‘Regulatory Action’; Jeanneret et al., ‘My Advocacy Is Not about Me’.
76.
Jeanneret et al., ‘My Advocacy Is Not about Me’.
77.
Jeanneret et al., ‘Regulatory Action’; Jeanneret et al., ‘My Advocacy Is Not about Me’.
78.
Jeanneret et al., ‘Regulatory Action’; Jeanneret et al., ‘My Advocacy Is Not about Me’.
79.
Jeanneret et al., ‘Regulatory Action’; Jeanneret et al., ‘My Advocacy Is Not about Me’.
80.
Bouwman et al., ‘Patients’ Perspectives on the Role of Their Complaints’, p. 491; S. Wiig, L. Schibevaag, R. Tvete Zachrisen, E. Hannisdal, J. E. Anderson, and C. Haraldseid-Driftland, ‘Next of Kin Involvement in Regulatory Investigations of Adverse Events That Caused Patient Death: A Process Evaluation (Part I–The Next of Kin’s Perspective)’, Journal of Patient Safety 17(8) (2021), pp. e1713–e1718; R. D. Friele, E. M. Sluijs and J. Legemaate, ‘Complaints Handling in Hospitals: An Empirical Study of Discrepancies between Patients’ Expectations and Their Experiences’, BMC Health Services Research 8(1) (2008), p. 2; R. Bouwman, M. Bomhoff, P. Robben, and R. Friele, ‘Is There a Mismatch Between the Perspectives of Patients and Regulators on Healthcare Quality? A Survey Study’, Journal of Patient Safety 17(7) (2021), p. 477.
81.
Bouwman et al., ‘Patients’ Perspectives on the Role of Their Complaints’, p. 477; Friele et al., ‘Complaints Handling in Hospitals’, p. 2.
82.
Wiig et al., ‘What Methods Are Used to Promote Patient and Family Involvement’; Wiig et al., ‘Next of Kin Involvement’; S. Wiig, P. D. Hibbert and J. Braithwaite, ‘The Patient Died: What about Involvement in the Investigation Process?’, International Journal for Quality in Health Care 32(5) (2020), pp. 342–346; Adams et al., ‘Including Citizens in Institutional Reviews’; E. Richardson, K. Walshe, A. Boyd, J. Roberts, L. Wenzel, R. Robertson, and R. Smithson, ‘User Involvement in Regulation: A Qualitative Study of Service User Involvement in Care Quality Commission Inspections of Health and Social Care Providers in England’, Health Expectations 22(2) (2019), pp. 245–253; Bouwman et al., ‘Patients’ Perspectives on the Role of Their Complaints’.
83.
H. Dolev and A. Benish, ‘Classifying Participatory Methods in Social Care Regulation’, Social Policy & Administration 58 (2024), pp. 1–17.
84.
There is a substantial body of literature which discusses the importance of patients and caregivers being involved in healthcare delivery and design, described variously as patient/consumer/public involvement/engagement/participation: see footnote 8 above. Because of this article’s focus on regulation, a closer examination of the patient engagement scholarship is outside the scope of this article, though it is noted that some actions described in this literature may be conceived of as regulation.
85.
Wiig et al., ‘What Methods Are Used to Promote Patient and Family Involvement’; Wiig et al., ‘Next of Kin Involvement’; Wiig, Hibbert and Braithwaite, ‘The Patient Died’; Adams et al., ‘Including Citizens in Institutional Reviews’; Richardson et al., ‘User Involvement in Regulation’; Bouwman et al., ‘Patients’ Perspectives on the Role of Their Complaints’.
86.
Wiig et al., ‘What Methods Are Used to Promote Patient and Family Involvement’, pp. 3–9.
87.
Wiig et al., ‘What Methods Are Used to Promote Patient and Family Involvement’, pp. 6–7.
88.
Wiig et al., ‘What Methods Are Used to Promote Patient and Family Involvement’, pp. 6–7.
89.
Wiig et al., ‘What Methods Are Used to Promote Patient and Family Involvement’, pp. 6–7.
90.
Koop and Lodge, ‘What is Regulation?’, p. 97.
91.
C. Degeling et al., ‘Which Public and Why Deliberate?’, p. 114.
92.
C. Degeling et al., ‘Which Public and Why Deliberate?’, p. 117.
93.
C. Degeling et al., ‘Which Public and Why Deliberate?’, p. 118.
94.
C. Degeling et al., ‘Which Public and Why Deliberate?’, p. 119.
95.
C. Degeling et al., ‘Which Public and Why Deliberate?’, p. 119.
96.
C. Degeling et al., ‘Which Public and Why Deliberate?’, p. 119.
97.
C. Degeling et al., ‘Which Public and Why Deliberate?’, p. 119.
98.
Hoffman et al., Patients as Policy Actors.
99.
Hoffman et al., Patients as Policy Actors.
100.
Hoffman et al., Patients as Policy Actors, p. 3.
101.
Hoffman et al., Patients as Policy Actors.
102.
J. Fairman, ‘Patients and the Rise of the Nurse-Practitioner Profession’, in B. Hoffman, N. Tomes, R. Grob, and M. Schlesinger, eds., Patients as Policy Actors (New Brunswick, NJ: Rutgers University Press, 2011), pp. 215–216.
103.
A. Dockser Marcus, ‘The Power of Us: A New Approach to Advocacy for Rare Cancers’, in B. Hoffman, N. Tomes, R. Grob, and M. Schlesinger, eds., Patients as Policy Actors (New Brunswick, NJ: Rutgers University Press, 2011), pp. 197–214.
104.
Dockser Marcus, ‘Power of Us’, p. 197.
105.
Dockser Marcus, ‘Power of Us’, pp. 197–214.
106.
Dockser Marcus, ‘Power of Us’, p. 210.
107.
Aymé et al., ‘Empowerment of Patients’, p. 2050.
108.
109.
110.
N. Tomes, ‘From Outsiders to Insiders: The Consumer-Survivor Movement and Its Impact on U.S. Mental Health Policy’ in B. Hoffman, N. Tomes, R. Grob, and M. Schlesinger, eds., Patients as Policy Actors (New Brunswick, NJ: Rutgers University Press, 2011), pp. 113–131.
111.
Tomes, ‘From Outsiders to Insiders’, p. 113.
112.
B. Hoffman, ‘“Don’t Scream Alone”: The Health Care Activism of Poor Americans in the 1970s’ in B. Hoffman, N. Tomes, R. Grob, and M. Schlesinger, eds., Patients as Policy Actors (New Brunswick, NJ: Rutgers University Press, 2011), p. 133.
113.
Hoffman, ‘Don’t Scream Alone’, p. 133.
114.
Jeanneret et al., ‘Regulatory Action’; Jeanneret et al., ‘My Advocacy Is Not about Me’.
115.
Black, ‘Critical Reflections’, p. 26.
116.
I. Ayres and J. Braithwaite, Responsive Regulation: Transcending the Deregulation Debate (Oxford: Oxford University Press, 1992).
117.
Baldwin et al., ‘Introduction’, p. 4.
118.
Healy, ‘Patients as Regulatory Actors in Their Own Health Care’, pp. 591–609.
119.
Hancher and Moran, ‘Organizing Regulatory Space’, pp. 286–287.
120.
Hancher and Moran, ‘Organizing Regulatory Space’, pp. 286–287.
121.
Healy, ‘Patients as Regulatory Actors in Their Own Health Care’; Healy, Improving Healthcare, pp. 283–306.
122.
Hoffman et al., Patients as Policy Actors; Wiig et al., ‘What Methods Are Used to Promote Patient and Family Involvement’; Adams et al., ‘Including Citizens in Institutional Reviews’; Richardson et al., ‘User Involvement in Regulation’; Bouwman et al., ‘Patients’ Perspectives on the Role of Their Complaints’; Madison, ‘Patients as “Regulators”?’
123.
Jeanneret et al., ‘Regulatory Action’; Jeanneret et al., ‘My Advocacy Is Not about Me’.
124.
Jeanneret et al., ‘Regulatory Action’; Jeanneret et al., ‘My Advocacy Is Not about Me’.
125.
Jeanneret et al., ‘My Advocacy Is Not about Me’, p. 319.
126.
Jeanneret et al., ‘Regulatory Action’, p. 720.
127.
Jeanneret et al., ‘Regulatory Action’, p. 730–732; Jeanneret et al., ‘My Advocacy Is Not about Me’, pp. 322–324.
128.
Jeanneret et al., ‘Regulatory Action’; Jeanneret et al., ‘My Advocacy Is Not about Me’.
129.
Jeanneret et al., ‘Regulatory Action’, p. 731.
130.
Jeanneret et al., ‘Regulatory Action’, p. 731.
131.
Jeanneret et al., ‘Regulatory Action’; Jeanneret et al., ‘My Advocacy Is Not about Me’.
132.
Wiig et al., ‘What Methods Are Used to Promote Patient and Family Involvement’, pp. 6–7; Wiig et al., ‘Next of Kin Involvement’, pp. e1713–e1718; Wiig et al., ‘The Patient Died’, pp. 342–346; Adams et al., ‘Including Citizens in Institutional Reviews’, pp. 1463–1473; Richardson et al., ‘User Involvement in Regulation’, pp. 245–253; Bouwman et al., ‘Patients’ Perspectives on the Role of Their Complaints’, pp. 483–496.
133.
Dolev and Benish, ‘Classifying Participatory Methods’, pp. 1–17.
134.
Wiig et al., ‘What Methods Are Used to Promote Patient and Family Involvement’, pp. 6–7.
135.
See, for example, C. Degeling et al., ‘Which Public and Why Deliberate?’.
136.
Jeanneret et al., ‘Regulatory Action’; Jeanneret et al., ‘My Advocacy Is Not about Me’.
137.
Jeanneret et al., ‘Regulatory Action’; Jeanneret et al., ‘My Advocacy Is Not about Me’.
138.
Jeanneret et al., ‘Regulatory Action’; Jeanneret et al., ‘My Advocacy Is Not about Me’.
139.
Black, ‘Critical Reflections’, p. 26.
140.
M. Schlesinger, ‘The Canary in Gemeinschaft’ in B. Hoffman, N. Tomes, R. Grob, and M. Schlesinger, eds., Patients as Policy Actors: A Century of Changing Markets and Missions (New Brunswick, NJ: Rutgers University Press, 2011), p. 151.
141.
Schlesinger, ‘The Canary’, p. 151.
142.
Baldwin et al., Understanding Regulation, p. 69.
143.
Jeanneret et al., ‘Regulatory Action’, p. 731.
144.
R. Jeanneret, E. Close, L. Willmott, J. Downie, and B. P. White, ‘Patients’ and Caregivers’ Suggestions for Improving Assisted Dying Regulation: A Qualitative Study in Australia and Canada’, Health Expectations 27(3) (2024), p. e14107.
145.
Healy, ‘Patients as Regulatory Actors in Their Own Health Care’, p. 592.
146.
Close et al., ‘Experiences of Institutional Objection to Medical Assistance in Dying’; White et al., ‘The Impact on Patients of Objections by Institutions to Assisted Dying’.
147.
Jeanneret et al., ‘My Advocacy Is Not about Me’, p. 320.
148.
Hoffman et al., Patients as Policy Actors.
149.
Hoffman et al., Patients as Policy Actors; Aymé et al., ‘Empowerment of Patients’, pp. 2048–2051.
150.
Hoffman, ‘Don’t Scream Alone’, pp. 132–147.
151.
Tomes, ‘From Outsiders to Insiders’, p. 113.
152.
Jeanneret et al., ‘My Advocacy Is Not about Me’, pp. 320 and 322.
153.
Jeanneret et al., ‘My Advocacy Is Not about Me’, p. 323.
154.
Jeanneret et al., ‘Regulation Action’, p. 722.
155.
Madison, ‘Patients as “Regulators”?’, p. 34. See also, in relation to the regulatory role of individuals: Hancher and Moran, ‘Organizing Regulatory Space’, pp. 286–287.
156.
Jeanneret et al., ‘Regulatory Action’; Jeanneret et al., ‘My Advocacy Is Not about Me’.
157.
Black, ‘Critical Reflections’, p. 26.
158.
Jeanneret et al., ‘Regulatory Action’, pp. 729–731; Jeanneret et al., ‘My Advocacy Is Not about Me’, pp. 323–324.
159.
A. MacLean, ‘Audrey Parker Remembered as Nova Scotia Updates Its Assisted-Dying Policy’, Global News (10 August 2022), available at https://globalnews.ca/news/9051131/audrey-parker-medically-assisted-death-nova-scotia-law/; Dying With Dignity Canada, Audrey Parker’s Last Message to Canadians (Video, 6 February 2019), available at ![]() .
.
160.
MacLean, ‘Audrey Parker Remembered’.
161.
Rodriguez v Canada (Attorney General) [1993] 3 SCR 519; Carter v Canada (Attorney General) [2015] 1 SCR 331; Truchon v Canada (Attorney General) [2019] QCCS 3792; Lamb and British Columbia Civil Liberties Association v Canada (Attorney General) [2016] Supreme Court of British Columbia, No S-165851.
162.
E. Bereza, ‘The Private and Public Deaths of Sue Rodriguez’, McGill Law Journal 39 (1994), p. 719.
163.
J. Downie, ‘From Prohibition to Permission: The Winding Road of Medical Assistance in Dying in Canada’, HEC Forum 34(4) (2022), pp. 321–354.
164.
Hoffman et al., Patients as Policy Actors, p. 110.
165.
R. Grob, ‘A House on Fire: Newborn Screening, Parents’ Advocacy, and the Discourse of Urgency’ in Hoffman et al., eds., Patients as Policy Actors: A Century of Changing Markets and Missions (New Brunswick, NJ: Rutgers University Press, 2011), p. 251.
166.
Adams et al., ‘Including Citizens in Institutional Reviews’, p. 1463.
167.
Grob, ‘A House on Fire’, p. 251.
168.
A. Cornwall, ‘Unpacking “Participation”: Models, Meanings and Practices’, Community Development Journal 43(3) (2008), p. 279.
169.
Baldwin et al., Understanding Regulation, p. 69.