
Abstract
This article assesses the regulatory framework relating to over-the-counter (OTC) sales of antibiotics for human use in India. The OTC sale of antibiotics is recognised as a pathway for the emergence of antimicrobial resistance (AMR); a serious public health challenge in need of urgent regulatory responses. Analytically, this article identifies opportunities within existing laws in India and highlights gaps that need to be filled by modifying existing laws or developing new ones. Conceptually, it suggests a need to reflect on the limits of traditional, top-down, ‘command-and control’ regulation and to think about alternative approaches. The article therefore advocates for an approach to regulation that incorporates two elements. First, it argues for a broader concept of regulation that encompasses binding as well as non-binding regulatory instruments and initiatives aimed at influencing stakeholder behaviour (including soft regulation, economic incentives, information campaigns and uses of technology). Second, it makes the case for enhanced stakeholder participation in regulatory design. The article will be relevant for health policy and drug regulators in India and other low- and middle-income countries, as well as legal scholars, social scientists and others interested in the regulation of OTC sales of antibiotics for AMR containment.
Introduction
Antimicrobial resistance (AMR), which refers to the ability of a microorganism to resist an antimicrobial drug (such as an antibiotic), is a very serious global public health challenge. 1 The 2016 review on AMR, commissioned by the UK government and chaired by economist Lord O’Neill, estimates that AMR will pose a risk to 10 million lives a year and a cumulative 100 trillion USD of economic output by 2050 if we do not act now. 2 A major contributing factor, particularly in low-income and middle-income countries (LMICs), is widespread inappropriate use of antibiotics together with lack of knowledge about responsible use among many stakeholders. 3 The World Health Organization’s Global Action Plan on Antimicrobial Resistance (WHO GAP), 4 adopted by the World Health Assembly in 2015, recognises the need for regulation to optimise the use of antibiotics. WHO member states have created national action plans (NAPs) that align with the WHO GAP and have begun to put these into effect. 5
Against this backdrop of ongoing activity, it is appropriate to take stock of the challenges that LMICs face in effective design and implementation of AMR NAPs, as well as to consider possibilities for improving regulatory systems. The global academic community, policymakers, regulators and other stakeholders could all engage in this process by sharing knowledge, ideas and insights. Case studies can form a useful starting point for analysis and discussion. To this end, this review article examines the regulatory architecture for over-the-counter (OTC) sales of antibiotics for human use in India.
LMICs are important to study for several reasons. Although AMR emergence is a concern in all countries regardless of income level, LMICs bear a heavier burden. 6 Contributory factors include high levels of antibiotic use and misuse, poor access to quality healthcare, inadequate safe water and sanitation services and high loads of infectious disease in the general population. 7 Studies have also shown that LMICs, especially those in Africa and Asia, have weak AMR surveillance systems due to lack of appropriate laboratory facilities, gaps in quality assurance, skilled personnel, laboratory supplies and management of lab services. 8 South East Asia is estimated to have the highest risk of AMR emergence and spread (e.g. New Delhi metallo-β-lactamase-1). 9 Among LMICs, India is of particular interest because it accounts for one-fourth of the global incidence of multidrug-resistant tuberculosis 10 and has one of the highest rates of antibiotic resistance in bacteria that cause common infections in the community and healthcare facilities. 11 It is also one of the largest producers 12 and consumers of antibiotics for human use 13 and has a high level of mortality due to drug-resistant pathogens. 14
Despite being illegal, OTC sales of antibiotics by pharmacies without a valid prescription from a registered medical practitioner (RMP) appear widespread in India, highlighting serious problems around the regulation of this pathway for emergence of AMR. A number of socio-economic and structural drivers common to India and other LMICs have been identified. 15 As a general background factor, the implementation of national medicines regulations is poor. India has a legal framework that requires a valid prescription as a condition for the sale of antibiotics, but compliance is low and regulatory enforcement is patchy. 16 On the supply side, pharmacies – as businesses – are subject to commercial pressures. The desire to maximise profits and concerns about losing a sale or a customer to a rival pharmacy motivate the dispensing of antibiotics without a valid prescription. 17 Pharmaceutical companies’ drug promotion programmes may also influence dispensing practices by making it more profitable to sell certain newer, branded antibiotics. 18 Additionally, while regulations require the presence of a qualified pharmacist on-site during opening hours, in practice, pharmacy owners do not always adhere to this rule; nor is it enforced rigorously by government agencies. 19 As a result, antibiotics are often dispensed by staff who lack medical qualifications and have inadequate knowledge of drug safety and efficacy.
On the demand side, a range of factors prompt patients to seek antibiotics from pharmacists directly. 20 Patients in remote, rural areas may not be able to access a doctor easily to obtain a diagnosis and prescription, so turn instead to a pharmacy as their first point of medical care. 21 Although patients in urban areas are in closer proximity to physicians, they may also choose to seek medication at pharmacies to avoid lengthy waiting times in the overstretched public health system. 22 Poorer patients may be unable to afford both medicines and doctors’ consultation fees, so have little choice but to obtain their medicines from pharmacists without a prescription. 23 Self-medication is therefore commonplace. Patients’ choices about which antibiotics to take may be based on previous prescriptions given to them by doctors or on recommendations from pharmacy staff (who are thought to possess good medical knowledge). 24 Members of the public may also believe mistakenly that it is appropriate to use antibiotics to treat non-bacterial infections, such as viral fevers. 25 Finally, both pharmacy staff and their customers may have low awareness of AMR and be ambivalent about the health risks posed to themselves and the wider community by the inappropriate and unnecessary use of antibiotics. 26
The current regulatory framework governing the sale of antibiotics in India and any upcoming reforms will need to grapple with all these contextualised factors and behaviours to be effective. With this goal in mind, this review article adds to the growing body of literature by providing an up-to-date map of the Indian regulatory landscape for OTC sales of antibiotics. Analytically, it identifies opportunities for ensuring responsible antibiotic use within existing laws relating directly or indirectly to OTC sales of antibiotics for human use. It also highlights gaps that need to be filled by modifying existing laws or developing new ones. The initiatives set out within India’s National Action Plan on Antimicrobial Resistance (NAP-AMR) (2017-2022) – and the way it conceptualises regulation more generally – are also presented and discussed.
In terms of historical context, it is important to note that the current Indian NAP-AMR follows an earlier proposed National Antibiotic Policy that was shelved due to difficulties of implementation. 27 This suggests a need to reflect on the limits of traditional, top-down, ‘command-and control’ regulation in this context and consider alternative approaches. Lessons from other countries also suggest that stricter enforcement of current regulation alone may not be effective. 28 This review article therefore advocates for an approach to regulation that incorporates two elements: first, a broader concept of regulation that encompasses binding as well as non-binding regulatory instruments and initiatives aimed at influencing stakeholder behaviour (including soft regulation, economic incentives, information campaigns and uses of technology); 29 and second, enhanced stakeholder participation in regulatory design. Incorporating these two elements could help produce a regulatory framework that is better suited to the realities on the ground in India and therefore more effective. Ideally, robust stakeholder consultation would be used as an opportunity to understand stakeholders’ interests and the likely impact of regulatory changes. The suitability of transplanting regulatory initiatives used in other countries into the Indian context could also be assessed, or novel interventions co-designed in an iterative way through stakeholder input. We anticipate that the review article will be of interest and relevance for health policy and drug regulators in India and other LMICs, as well as legal scholars, social scientists and others whose work intersects with the regulation of OTC sales of antibiotics for human use as an aspect of AMR containment.
‘Regulation’, regulatory actors and instruments
Before exploring the regulatory architecture concerning OTC sales of antibiotics for human use in India in detail, it is useful to set out the understanding of ‘regulation’ adopted in this review article, the relevant actors/institutions and types of binding and non-binding government-led regulatory instruments, and to highlight the role of courts.
‘Regulation’ is a term that lacks a single unifying definition and has been used in a variety of contrasting ways. 30 If we consider the traditional, narrow perspective on regulation as ‘the promulgation of a binding set of rules to be applied by a body devoted to this purpose’, 31 the actors involved in the regulation of OTC sales of antibiotics for human use in India are the national and state governments, and authorities constituted under the Drugs and Cosmetics Act, 1940 (DCA) and the Drugs and Cosmetics Rules, 1945 (DCR) on the one hand (the regulators), and dispensers of antibiotics such as drug stores, chemists or druggists and pharmacists on the other (the regulated entities discussed in the second section).
By contrast, if we adopt a broader view of regulation as ‘all mechanisms affecting behaviour – whether these be state-based or from other sources (e.g. markets)’, 32 we find that a wide array of actors/institutions influence, and are affected by, the regulation of OTC sales of antibiotics for human use in India. These include e-pharmacies and their associations, medical practitioners in government and private hospitals and clinics and their associations, councils established pursuant to legislation at the central and state levels to regulate the education and practice of pharmacists and medical practitioners, consumers, non-governmental organisations, community-based organisations and religious organisations, as well as unregistered pharmacists and medical practitioners. In addition, pharmaceutical manufacturers, sellers, distributors and wholesalers could influence antibiotic prescribing/dispensing behaviour as well as disposal practices of pharmacists.
The main sources of government-led regulation that apply to several of the above-mentioned actors are the legislature and the executive. The former includes Parliament at the national level and state legislature at the state level, and the latter include government institutions at the central, state and union territory levels. The legislature enacts binding primary legislation (also known as a statute or an Act) and the executive enacts binding secondary legislation such as rules, regulations, notifications and orders. The executive also issues administrative instructions such as letters, circulars, orders, memoranda, pamphlets, public notices and press notices, as well as policies, programmes and campaigns. In terms of the force of these regulatory instruments, administrative instructions may or may not be legally binding depending on whether or not they have statutory backing, and policies, programmes and campaigns are not legally binding.
Focusing on the executive branch at the national level, the Ministry of Health and Family Welfare is the primary source of many of the binding and non-binding regulatory instruments that concern OTC sales of antibiotics for human use in India. The Directorate General of Health Services (DGHS) is responsible for the provision of evidence-based technical support for policy formulation and programme implementation in matters of public health, healthcare and medical education to the Ministry of Health and Family Welfare. Under the auspices of the DGHS, the Central Drugs Standard Control Organisation (CDSCO) is the national regulatory authority responsible for the DCA and the DCR. The Drugs Controller General of India (DCGI) heads the CDSCO and sets quality standards for the import, manufacture, distribution and sale of drugs in India. In addition, the Department of Pharmaceuticals within the Ministry of Chemicals and Fertilisers is responsible for the formulation and implementation of policies relating to drugs, especially drug prices and access.
The judiciary plays a significant role in enforcement in India. In addition to issuing fines or other penalties for violation of the laws relating to the sale of antibiotics without a valid prescription, courts have also ordered the executive branch to fulfil the duty to implement these laws when efforts have been lacking. 33 In some instances, judicial activism led to the modification of existing laws or the development of new laws relating to the sale of antibiotics. 34 In general, however, the judiciary is reluctant to interfere with the policymaking powers of the executive. 35 Court decisions are often mandatory and legally binding but sometimes they may be declaratory instead.
Overview of the regulatory framework
This section examines laws that have a bearing on OTC sales of antibiotics for human use in India. Some of these laws concern actors including pharmacists as the dispensers of antibiotics. Others relate to the education and practice of pharmacists and some to the manufacturers of antibiotics.
The DCA and the associated DCR are key pieces of legislation that regulate the import, manufacture, distribution and sale of drugs in India. They inter alia govern the dispensing practices of pharmacies. Schedule H of the DCR lists 521 drugs (including antibiotics) that can only be sold against a prescription from a registered medical practitioner (RMP). Nevertheless, there has been a long-standing and widespread practice of OTC sales of antibiotics without a valid prescription. As an early response to the need to address the challenge posed by AMR, the Government of India introduced the National Policy for Containment of Antimicrobial Resistance 2011. 36 This policy proposed some actions to monitor the sale of antibiotics such as the development of a separate list of OTC drugs including the quantity to be dispensed. In 2014, this led to the addition of Schedule H1 to the DCR, which listed 48 drugs as of 2020; the majority of which are antibiotics.
It is worth noting that the initial plan to give Schedule H1 an exclusive focus on antibiotics became somewhat weakened; drugs other than antibiotics, such as habit-forming medicines, also came to be included in the approved, final version. 37 Furthermore, while the requirements for Schedule H1 drugs are more burdensome than Schedule H, they are less onerous than those stipulated in Schedule X (which deals with drugs including narcotics and sedatives and mandates duplicate prescriptions to be retained for 2 years). The discussion in this section focuses on Schedule H and Schedule H1.
Dispensers of antibiotics
The DCA prohibits the sale of all drugs including drugs listed in Schedule H and Schedule H1 of the DCR without a licence. 38 The DCR sets out the general conditions of the licence for dispensers of antibiotics in both schedules. 39 Drugs included in Schedule H and Schedule H1 are to be sold on the written prescription of an RMP and only by or under the personal supervision of a registered pharmacist. The RMP must sign and date the prescription, specify the patient’s name and address and indicate the total amount and dosage of the medicine to be supplied on the prescription. The DCR and the Pharmacy Act, 1948 define the terms RMP and ‘medical practitioner’ respectively, 40 and the Pharmacy Practice Regulations, 2015 define a ‘registered pharmacist’ and ‘prescription’. 41
Broadly, the DCR identifies three categories of licensees. 42 These are pharmacy/pharmacist/dispensing chemist/pharmaceutical chemist; chemists; and druggists and drugstore. The first two categories require the services of a registered pharmacist. This means that drugstores cannot dispense antibiotics included in Schedule H and Schedule H1. The DCR also imposes several conditions on the licensees who can supply the drugs listed in Schedule H and Schedule H1, including antibiotics. 43 They must enter certain details in a separate prescription register or a cash or credit memo book specifically maintained for the purpose. Further, the person dispensing a prescription must follow the prescriber’s directions as stated on the prescription. There are some concerns, however, in terms of inadequacy or absence of relevant provisions. For example, the dispenser is not required to stamp the prescription, 44 or to retain it, 45 which would prevent its subsequent reuse.
For Schedule H1 drugs, the DCR imposes some additional conditions. 46 The supplier of a drug is required to record the supply in a separate register. They are also required to maintain these records for 3 years and the records are open for inspection. By contrast, the licensee is required to preserve all registers and other records in respect of other drugs including those in Schedule H for just 2 years. Although the government had initially planned to require double prescriptions for Schedule H1 drugs, as is the case with Schedule X drugs, this proposal was dropped following opposition from industry associations and medical practitioners concerned about the practicalities of implementation and potential loss of revenue. 47
Scholars have questioned the underlying rationale for listing certain antibiotics within Schedule H as opposed to the somewhat more demanding Schedule H1. 48 There is also a degree of uncertainty as to whether all antibiotics are indeed covered comprehensively within either Schedule H or Schedule H1. Line 32 of Schedule H lists ‘antibiotics’ in broad terms in a single line. Yet in addition to this, some antibiotics are given separate, individual listings in either Schedule H or Schedule H1, but other commonly used antibiotics (including gentamicin and tigecycline) are not mentioned. 49 Arguably, if the individual listing of antibiotics within Schedule H and Schedule H1 serves a valid purpose and is not merely superfluous, then this raises scope for interpretation around the legal coverage of unlisted antibiotics, which may or may not be covered by the catch-all provision of line 32 in Schedule H. 50
Tandon et al. have recommended a thorough revision of the various drug classification schedules in the DCR, with all antibiotics being listed across two dedicated classes: a ‘regular’ group and another group for higher antibiotics reserved for the most serious infections. 51 In a similar fashion, the NAP-AMR has established a requirement to review the categorisation of high-end antimicrobials as well as new antibiotics in Schedule X and Schedule H1 of the DCR. An alternative approach would be to revise the listings of antibiotics in the schedules (and perhaps the relative strictness of the legal requirements for sale) so as to reflect the WHO Access, Watch and Reserve categories. 52 This classifies antibiotics into three stewardship groups according to the importance of their optimal uses and potential for AMR. 53 Additionally, Tandon et al. have also suggested that sales of antibiotics should be recorded on a portal-based monitoring system. These reforms would offer advantages in terms of giving a clearer symbolic focus on antibiotics and the possibility of easier monitoring by regulators; assuming that transactions for antibiotics would indeed be recorded on the portal.
Enforcement of the DCA/DCR in relation to pharmacies
The provisions of the DCA/DCR have the potential to deter activities that lead to misuse or overuse of antibiotics. Within Indian states, it is the duty of state drug inspectors to inspect all premises licensed for the sale of drugs and to satisfy themselves that licensees are observing the conditions of the licence. 54 They are also empowered to conduct searches and seize drugs. 55 Further, the concerned licensing authority could suspend or cancel the licence where the licensee fails to comply with any of the conditions of the licence to sell or distribute drugs or with any provisions of the DCA/DCR. 56 The Central Licensing Approving Authority could also direct the licensee to stop the sale or distribution of the drugs and order their destruction. 57 The DCA specifies penalties (imprisonment and/or fine) in respect of certain first and subsequent offences, including the sale of any drug without a valid licence or of any other drug in contravention of the DCA/DCR. 58 It further provides for confiscation of the stock of the drug in respect of which a court has convicted a person. 59
Ultimately, however, the effectiveness of these provisions is contingent upon their active and effective enforcement by statutory authorities and compliance by regulated entities. Inspectors can check the details of antibiotics sold by pharmacists in the Schedule H1 register, but they will not have an accurate picture of antibiotic sales if these transactions go unrecorded. Further, the DCA/DCR do not provide for approaches to influence behaviour besides sanctions (in the forms of suspension/cancellation of licences, fines or imprisonment).
The CDSCO, however, recognises the important role of awareness in its advisories to different stakeholders seeking compliance with provisions relating to OTC sales of antibiotics under the DCA/DCR. It has advised all state drug controllers and pharmaceutical and consumer associations to comply strictly with the statutory requirements including stringent regulatory action on OTC sales without prescription of antibiotics. 60 According to CDSCO, stakeholders should raise awareness through consumer associations about the side effects of taking antibiotics without prescription to avoid AMR for the safety, well-being and protection of patients’ health. In addition, the DGHS/DCGI released an advisory on rational use of antibiotics for limiting AMR and provided details of regulatory steps taken by the Ministry of Health and Family Welfare to curb and control indiscriminate use of antibiotics. 61 The DGHS/DCGI also recommended that all state drugs controllers sensitise their enforcement officials to be vigilant in ensuring that such drugs are not sold by retail without a prescription from an RMP. This approach to raising awareness among regulators and stakeholders will be important to consider alongside any measures aimed at stricter enforcement of the existing laws. A further specific concern, however, is that the dispensing of drugs (including antibiotics) is often conducted by people who lack the relevant educational qualifications. This issue is discussed in the following subsection.
Education and practice of pharmacists
Compliance with existing or revised laws is contingent, among other factors, on the awareness and education of pharmacists about rational use of antibiotics and AMR. 62 There is also a correlation between comprehensive and relevant education and training of pharmacists on the use of antibiotics and AMR and change in the behaviour of consumers regarding antibiotic consumption. 63 The Pharmacy Council of India (PCI) is a statutory body incorporated under the Pharmacy Act, 1948 to regulate pharmacy education and the profession of pharmacy in India. The discharge of its statutory mandate could therefore influence the regulation of OTC sales of antibiotics.
The minimum standard of education required for qualifying and registering as a pharmacist and the curriculum norms are set out in different regulations made under section 10 of the Pharmacy Act. The norms do not include AMR as a separate/core component of any subject. Similarly, the Indian Medical Council Act, 1956 and the regulations made thereunder govern the education and practice of medical practitioners, but they do not incorporate specific provisions in respect of education and training on the rational use of antibiotics as well as AMR that could influence prescription practices. An amendment to these laws and the regulations made thereunder, which govern the education and practice of medical practitioners and pharmacists, respectively, could incorporate specific provisions in respect of education and training on the rational use of antibiotics as well as AMR. Such measures would be consistent with the steps outlined in the NAP-AMR regarding the improvement of professional education and training (see the third section).
Chapter IV of the Pharmacy Act requires the registration of pharmacists by state pharmacy councils. According to the Act, only a registered pharmacist shall dispense a medicine on the prescription of a medical practitioner. 64 The Pharmacy Practice Regulations 2015 also provide for dispensation of medicine against prescription of an RMP by a Registered Pharmacist. 65 There is some room for confusion here because the DCR offers wider scope; providing that a drug shall be supplied on the prescription of an RMP only by or under the personal supervision of a registered pharmacist. 66 In chapter 2 of these regulations, the PCI prescribes a code of ethics for its members, which includes several provisions that are applicable to OTC sales of antibiotics for human use. Of course, the ability and willingness of pharmacists to discharge these obligations is contingent upon their awareness of issues relating to OTC sales of antibiotics for human use and AMR, as well as their commercial interests. 67
Continuing pharmacy education programmes could provide an avenue for the dissemination of information relating to OTC sales of antibiotics for human use and AMR among pharmacists. Some provisions of the Pharmacy Practice Regulations are relevant here. First, for renewal of registration, the pharmacist is required to attend a minimum of two refresher courses in pharmacy, having a minimum of 1-day duration each within a span of five years. 68 These courses are organised by the PCI, state pharmacy councils, Central Government, state governments or a professional body recognised by the PCI. Second, a registered pharmacist shall participate in professional meetings as part of Continuing Pharmacy Education programmes organised by reputed professional academic bodies or any other authorised associations/organisations and regularly inform the PCI or the state pharmacy council of compliance. 69 Third, to promote rational use of drugs, the pharmacist shall be involved in activities such as updating the knowledge of drugs through continuing education programmes. 70 In practice, most dispensers obtain their information or update their information in informal ways such as through sales representatives, peers or physicians. 71 In an evolving regulatory environment, drug inspectors could appraise pharmacists of legal requirements and any changes thereto. 72
At present, there are no binding laws to govern the manufacturers, sellers and distributors of antibiotics who seek to influence dispensing practices of pharmacists through various forms of inducements. 73 However, the Pharmacy Practice Regulations provide that registered pharmacists/ pharmacy shall not (or not offer to) give, solicit or receive any gift, gratuity, commission or bonus in consideration of or return for referring, recommending or procuring of any patient for sale/dispensing of medicines. 74
Under the Pharmacy Practice Regulations, it is the duty of registered pharmacists to disseminate advice on public health issues, enforce the laws of the country and cooperate with the authorities in the administration of sanitary/public health laws and regulations. 75 However, awareness and education by themselves may not necessarily lead to voluntary compliance with laws. For instance, a study of pharmacists in Goa found that they are aware of Schedule H and Schedule H1 of the DCR but they do not follow the legal requirements in respect of record-keeping. 76 Current enforcement mechanisms should therefore be re-examined.
Enforcement of the Pharmacy Act and related instruments
The Pharmacy Act empowers state pharmacy councils to appoint pharmacy inspectors, with the previous sanction of the state government and sets out their powers and functions. 77 These inspectors can inspect any premises where drugs are dispensed and submit a written report to the Registrar (who is the Secretary of the state pharmacy council), enquire whether a person who is engaged in dispensing of drugs is a registered pharmacist, investigate any complaint made in writing in respect of any contravention of the Pharmacy Act and report to the Registrar, and institute prosecution. However, failure to monitor compliance and non-enforcement is widespread, due to reasons that include the failure of state pharmacy councils to appoint pharmacy inspectors. 78
To promote compliance with the above-mentioned provisions of binding regulatory instruments, the CDSCO also relies on certain softer instruments. For instance, it released an advisory asking the All India Organisation of Chemists and Druggists, a representative body of pharmaceutical retail and wholesale traders, to educate its members to follow conditions of licence for sale of drugs strictly and cooperate with regulatory authorities to prevent such sale of drugs, and the pharmaceutical industry to use their well-developed marketing network to discourage pharmacists from selling antibiotics without prescription. 79 The CDSCO also requested different statutory councils including the PCI to sensitise their members about the rational use of antibiotics. 80 In addition, it advised the supply chain system once again to comply strictly with the statutory requirements. 81
The Pharmacy Act also creates sanctions for certain offences such as falsely claiming to be registered in the state register, dispensing by unregistered persons, failure to surrender a certificate of registration and wilfully obstructing an inspector in exercise of statutory powers. 82 The Act also identifies the relevant adjudicatory authorities. Yet the reality is that non-state, autonomous bodies such as the PCI and state pharmacy councils are reluctant to take action against their own members. 83 In any case, the low likelihood of prosecution and level of fines are unlikely to have a significant deterrent effect.
Violations of the code of conduct set out in the Pharmacy Practice Regulations constitute professional misconduct and render the registered pharmacist liable for disciplinary action by the PCI. The regulations do not elaborate on the nature of the penalty but temporary or permanent removal from the register of pharmacists is a possibility. These provisions, however, remain unenforced because several states are yet to implement these regulations.
Manufacturers of antibiotics
The DCR prohibits the sale or distribution of the antibiotics included in Schedule H and Schedule H1 without a label and sets out labelling requirements. The label of the innermost container of a medicine for internal use containing these drugs and every other covering in which the container is packed must be labelled with the symbol Rx and conspicuously displayed on the left top corner of the label. The container must also be labelled with a specific caution, in legible black coloured font size in a completely red rectangular box, without disturbing the other conditions printed on the label.
As in the case of licensing requirements, there are some differences in the labelling requirements for Schedule H drugs and Schedule H1 drugs. For Schedule H drugs, there is no requirement in respect of the colour of the symbol Rx, and the caution reads as follows: ‘SCHEDULE H PRESCRIPTION DRUG – CAUTION. Not to be sold by retail without the prescription of a Registered Medical Practitioner’. By contrast, for Schedule H1 drugs, the symbol Rx must be red in colour and the caution shall read: ‘SCHEDULE H1 PRESCRIPTION DRUG – CAUTION. It is dangerous to take this preparation except in accordance with the medical advice. Not to be sold by retail without the prescription of a Registered Medical Practitioner’.
These labelling requirements emerged following the ‘Medicines with the Red Line’ campaign, developed by the Ministry of Health and Family Welfare along with the Organisation of Pharmaceutical Producers of India, which represents the research-based pharmaceutical companies in India, to create public awareness on rational use of antibiotics, and launched in February 2016. 84 A vertical red line on the packaging indicated to the dispensing pharmacist as well as patients that these medicines are dispensed only on prescription. The campaign had several key messages: learning how to identify prescription drugs, curbing self-medication and becoming more aware of the dangers of misusing antibiotics. 85 The Red Line campaign also illustrates the influence of non-binding regulatory measures on the development of binding regulatory provisions.
Regulatory instruments in the pipeline
So far, we have focused on existing binding regulatory instruments. Clearly, this regulatory framework does not address all aspects of OTC sales of antibiotics for human use in India. Regulatory instruments are in the pipeline to address gaps relating to e-pharmacies and the promotion and marketing of pharmaceutical drugs by pharmaceutical companies before healthcare professionals.
First, in recent years, e-pharmacies or Internet pharmacies have emerged as an alternative, quick and easy source of access to antibiotics for consumers in India. They operate, however, within a regulatory grey area. 86 In August 2018, the Ministry of Health and Family Welfare circulated a draft amendment to the DCR for the insertion of a new ‘Part VIB – Sale of Drugs by E-Pharmacy’ to regulate online sale of medicines. 87 This part will include provisions for registration of e-pharmacies, maintenance of record of cash or credit memo against which any drug is supplied, inspection every 2 years and monitoring. In February 2019, the Central Government sought a 6-month extension from the Mumbai High Court to publish the final rules. 88 At the time of writing, the draft rules are still pending approval.
Second, there is currently no regulation of promotion and marketing of pharmaceutical drugs by pharmaceutical companies before healthcare professionals. The Central Government was contemplating introduction of the Draft Essential Commodities (Control of Unethical Practices in Marketing of Drugs) Order, 2017, which would be legally binding. The Ministry of Law and Justice, however, rejected the proposal of putting the draft under the Essential Commodities Act 1955 in December 2018 (perhaps because it is outside the core objectives of the Act; which is to control production, supply and distribution of essential commodities). 89 The National Institute for Transforming India (NITI Aayog), the Government of India’s premier think tank, has taken up further drafting. 90
Reflections on the current regulatory framework and its enforcement
We have seen that the DCA and Schedules H and H1 of the DCR establish that antibiotics can only be sold by or under the personal supervision of a registered pharmacist against a valid prescription from an RMP. State drug inspectors are responsible for enforcement of the DCA/DCR. Penalties for violations include fines, imprisonment and the suspension or cancellation of a pharmacy licence. Another important source of legal norms is the Pharmacy Act. This specifies that pharmacists must be registered with state pharmacy councils. The Pharmacy Practice Regulations stipulate that antibiotics can only be dispensed by a registered pharmacist against a valid prescription. State pharmacy councils can appoint pharmacy inspectors to enforce these regulations. Penalties can be issued for offences including falsely claiming to be registered in the state register or unlawful dispensing by unregistered persons.
On their face, the above regulations governing OTC sales of antibiotics in India seem reasonably comprehensive in terms of their scope and content and set out mechanisms for enforcement and sanctions for non-compliance. It is difficult, however, to construct an accurate and comprehensive picture of the current state of enforcement. This is because official data in forms such as recorded numbers of pharmacy inspections and prosecutions across the country or on a state-by-state basis are not readily available. Analysis of pharmaceutical sales data in Indian private sector retail pharmacies between 2008 and 2018 indicates a reduction in sales volume of the antibiotics covered under Schedule H1 of the DCR after 2014 (i.e. when Schedule H1 came in to force). 91 This suggests that Schedule H1 has had some impact on sales of the listed antibiotics. Nevertheless, mystery/simulated/standardised client methodology, observational studies and interviews with pharmacists offer a different perspective of the situation on the ground.
For example, a simulated client study conducted in Bangalore, Karnataka, showed that 174 of 261 pharmacies (66.7%) provided antibiotics without prescription in two simulated scenarios: an adult complaining of upper respiratory tract infection and a request for medication for a child who was likely suffering from acute gastroenteritis. 92 These conditions do not generally require antibiotic therapy. 93 Similarly, in Tamil Nadu, observations and interviews with pharmacists at 24 pharmacies revealed that 78.7% of antibiotics sold within the study period were given without a prescription. 94 A focus group study by Kotwani et al. reported that of 40 New Delhi pharmacists, none said they refused to sell antibiotics without prescription. 95 By contrast, a standardised patient study conducted in Udupi district, Karnataka, found considerably lower rates of antibiotic dispensing without a prescription. 96 The results of this latter study offer an important counter-point and indicate there may be significant variation in pharmacy practice geographically. Yet overall, the picture across India appears to be one of widespread flouting of the regulations governing the sale of antibiotics. 97
The way we frame and understand this state of affairs will likely influence our choice of solutions. If viewed as a straightforward problem of regulatory enforcement, then traditional and familiar regulatory options will naturally present themselves. A first step might be to close any gaps in the current regulatory framework (such as the lacunae relating to e-pharmacies and promotion and marketing by pharmaceutical companies) through appropriate reforms. Next, we might explore strategies to improve compliance. One approach would be to enhance surveillance measures. This could include more frequent inspections of pharmacies and their prescription and sales records. Drug inspectors might also adopt simulated client methodology to check pharmacists’ adherence to the rules. Another tactic would be to strengthen the sanctions in place to increase their deterrent effect. This could involve issuing more pharmacy licence suspensions and increasing the levels of fines for regulatory violations.
Yet although the widespread non-compliance with the regulations for OTC sales of antibiotics in India is indeed in part a problem of regulatory enforcement, it is important to recognise that the situation has additional complex dimensions. Behaviours and practices on both the demand and supply sides that appear ‘irrational’ have emerged as responses to the economic and structural factors associated with fragile public healthcare systems. 98 Stakeholders’ health and economic and interests may also be impacted profoundly by changes to the status quo. Arguably, regulatory reforms will need to take account of root causes and anticipate practical ramifications in order to be effective.
This is a prominent motif within the Chennai Declaration of 2012; a plan formulated by a consortium of Indian medical societies to tackle AMR. 99 Stressing the need for practical and realistic solutions within the Indian context, the Declaration asserts that overzealous enforcement of the ban on OTC sales of antibiotics will likely be unhelpful. The Declaration therefore called for more nuanced and sophisticated approaches to regulatory enforcement.
These concerns have been borne out by subsequent developments in India, which appear to show that regulatory crackdowns may be counterproductive. 100 Contestation of regulations by stakeholders (particularly pharmacists) remain a foreseeable outcome. 101 Furthermore, studies assessing the impact of regulatory interventions in other LMICs highlight that law enforcement measures by themselves might not be effective. 102 Approaches that combine law enforcement with measures to increase awareness about appropriate use of antibiotics and encourage stakeholder participation are more likely to be fruitful. The following section examines the Indian NAP-AMR and the extent to which it engages with these themes and ideas.
The National Action Plan on Antimicrobial Resistance
Following the World Health Assembly’s adoption of the WHO GAP on AMR in 2015, many countries have formulated their own related national action plans. The Indian NAP-AMR (2017–2022) was published by the Ministry of Health and Family Welfare in 2017. 103 It represents India’s strategic response to the AMR challenge and is aligned clearly with the WHO GAP on AMR. 104 It incorporates all five of the WHO GAP ‘objectives’ (though these are renamed as ‘strategic priorities’ in the NAP-AMR) and also adds a sixth strategic priority; namely, to strengthen India’s leadership on AMR (see Table 1, below). Details are provided through the ‘objectives’, ‘strategic interventions and activities’ and ‘key outputs’ listed under the six strategic priorities headings.
Strategic priorities outlined in the NAP-AMR.
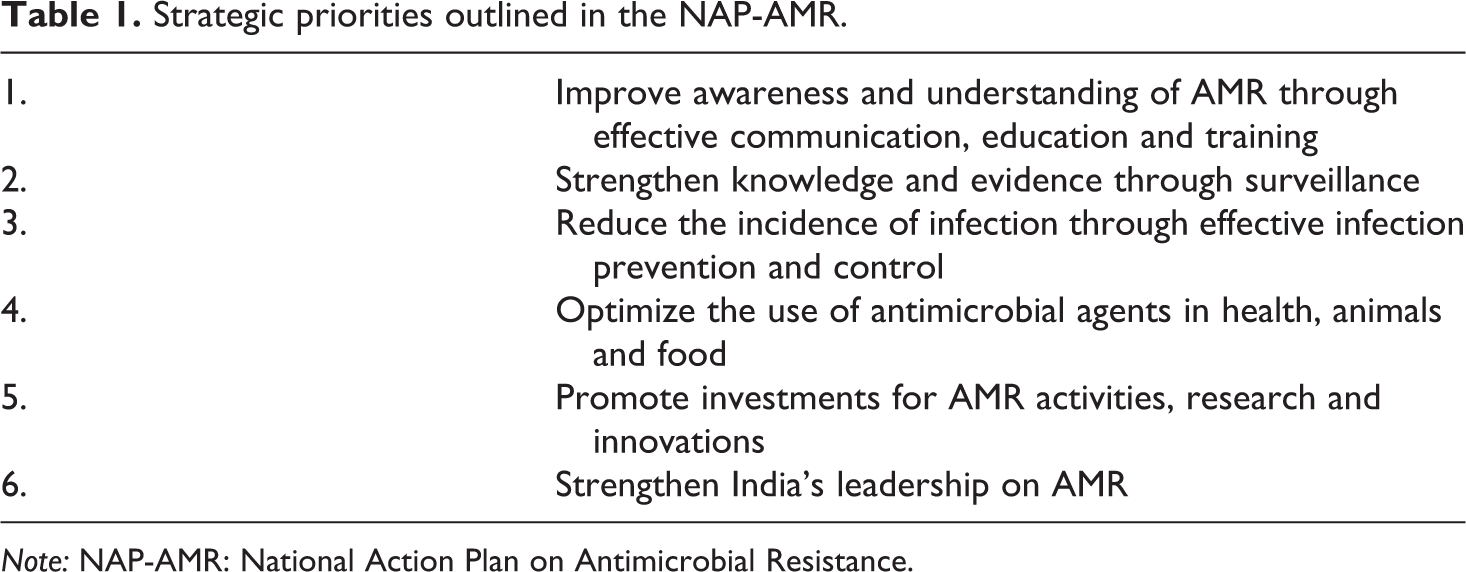
Note: NAP-AMR: National Action Plan on Antimicrobial Resistance.
Two of the strategic priorities set out in the NAP-AMR are particularly relevant to the regulation of OTC sales of antibiotics for human use in India. Strategic priority 1 is entitled: ‘Improve awareness and understanding of AMR through effective communication, education and training’. Work under this heading will include assessing the current level of understanding of AMR and antimicrobial use among key stakeholders. It will offer communication programmes on AMR (e.g. through information campaigns) to the general population and health professionals. It also proposes revising the curricula for professionals working in the human health sector and offering training modules to strengthen capabilities and skills. While increasing awareness of AMR among Indian stakeholders is a vital step for tackling AMR, education does not always result in behavioural change. Interventions designed to suit the Indian context will therefore also be necessary. 105
Strategic priority 4 is entitled: ‘Optimize the use of antimicrobial agents in health, animals and food’. Objective 4.1 aims to: ‘Ensure uninterrupted access to high-quality antimicrobial medicines’. As part of this, the government proposes to strengthen the national regulatory authority and regulations regarding use and access to antibiotics. To enhance regulatory enforcement prohibiting OTC sales of antibiotics under the DCA/DCR, government bodies will identify unlicensed pharmacies and unqualified medical practitioners and prescribers. They will also organise studies on antibiotic sales to understand incentives to sell or buy antibiotics. Also planned is a review of the categorisation of high-end antimicrobials as well as new antibiotics in Schedule X/H1 of the national regulations. The key output under this objective is to strengthen the national regulatory system and better implement regulations.
Objective 4.4 aims to ‘Improve appropriate use of antimicrobials in the community’. It proposes that agencies should develop awareness campaigns targeted at prescribers, providers and dispensers regarding existing rules and laws and appropriate use of antimicrobials. Awareness campaigns will also be developed that address consumers and the community, including schools and colleges, focussing on the risks to patients of inappropriate use.
Under objective 4.5, the government plans to ‘Strengthen the legislation regarding various facets of antimicrobials’. Strategic interventions and activities will include organising a consultation with regulatory bodies to review current legislation on antimicrobial prescription and the feasibility of strengthening existing legislation and introducing new legislation. Agencies will also be tasked with identifying additional regulatory interventions or support needed to effectively implement Schedule H1 and Schedule X restrictions.
These proposals within the NAP-AMR appear positive and helpful. The planned review of the categories in Schedule H1 of the DCR and the strengthening of the national regulatory authorities both seem logical steps towards improving compliance. Nevertheless, the Chennai Declaration’s earlier advice that heavy-handed implementation that fails to take account of stakeholder interests will likely be unhelpful will be important to bear in mind when engaging in reforms. A further interesting aspect of the NAP-AMR is that the Indian government acknowledges implicitly that laws and rules by themselves will probably be insufficient to engender widespread behavioural change. It therefore recommends the development of additional regulatory interventions or other measures to support compliance. It is also noteworthy that the government will organise studies to improve understanding of why people buy or sell antibiotics without prescription. However, it is not clear how the government will go about these tasks or whether or how stakeholder input will feed into any upcoming legal reforms or the design or adoption of interventions aiming to encourage compliance with the norms enshrined within legislation. There is therefore scope for further discussion on the optimum methodologies for achieving the objectives set out in the NAP-AMR.
Future directions for regulation
India stands at a crucial junction for modifying its regulatory landscape to tackle the OTC sales of antibiotics for human use. Following the analysis of the current legal framework and the proposals in the NAP-AMR, three key themes emerge for discussion on the best way forward.
Strengthening the regulatory framework
The NAP-AMR points to the need to revise and ‘strengthen’ the regulations and the national regulatory authority to improve implementation. On these points, it is useful to reflect on both the capacity of the regulator to enforce regulation and their willingness to do so. In 2012, a Parliamentary Standing Committee report on the functioning of the CDSCO highlighted inadequate staffing levels. 106 These would impact on the capacity of statutory authorities to undertake enforcement activities such as conducting regular/surprise inspections and imposing penalties in case of a breach; especially if there is a very large number of pharmacies 107 and other competing demands on resources. The willingness of the regulator to enforce laws could be influenced by several factors including corruption, prioritisation of resources and certain enforcement activities over others, and increased workload. Some regulators may be ambivalent about regulatory goals 108 and turn a blind eye where the consumers do not have access to a medical practitioner for obtaining a prescription. 109 Increased resources and further training for regulatory bodies, as well as enhanced cooperation among overlapping regulators, could begin to address these issues, but will not provide a complete solution.
Stakeholder engagement
It is encouraging that the NAP-AMR appears to signal a move away from a top-down, government-led regulatory reforms, which might fail to take account of the dynamics that influence behaviour at the community/individual level. 110 Robust stakeholder engagement will ensure that policymakers and regulators have a solid grasp of stakeholder interests and allow them to test the likely impact of reforms and anticipate levels of compliance. The insights gained should inform the development of regulatory initiatives.
Elements of this approach to stakeholder engagement are present in India’s NAP-AMR, for example, in relation to organising ‘studies on antibiotic sales to understand incentives to sell or buy antibiotics’. Arguably though, more emphasis could be placed on understanding the commercial and non-commercial interests of all relevant stakeholders. Improved awareness of how stakeholders interact and influence each other may also reveal further possibilities for meaningful regulation. For example, parties other than state agencies – such as private organisations – might be encouraged to develop roles as surrogate regulators.
Questions also emerge regarding the range of stakeholders included in consultations. In addition to e-pharmacies, other relevant potential actors include unlicensed medical practitioners and pharmacists, Ayurveda, Yoga and Naturopathy, Unani, Siddha and Homeopathy (AYUSH) practitioners and informal healthcare providers who lack formal medical qualifications/training but provide more than 70% of all primary care in rural India and poor urban areas such as slums. 111 It is not clear that the NAP-AMR acknowledges this latter set of actors as being among the key stakeholders who should receive AMR training. Non-binding regulation, including soft regulation, could be a way to recognise and engage with marginalised stakeholders such as alternative/unlicensed medicine practitioners within the scope of the overall regulatory system in a way that might be palatable to more formally recognised stakeholders, such as qualified physicians and pharmacists and their professional bodies. Of course, any regulatory initiatives targeting such stakeholders would need to be designed with sensitivity to political and policy concerns.
Novel regulatory interventions
The NAP-AMR seems to acknowledge the limits of law as a tool to effect social change. It therefore suggests that government agencies should identify additional regulatory interventions or support needed to effectively implement Schedule H1 and Schedule X restrictions. This opens an interesting opportunity to work with Indian stakeholders to co-design new types of interventions. The Indian government could also look for inspiration at approaches that have already been implemented in other LMICs (and even in high-income countries) and assess their adaptability for the Indian context.
Examples of such interventions can be divided into a number of categories. 112 Public awareness and information campaigns relating to rational use of antibiotics and AMR are widely recognised as an essential complement to binding regulations. Campaigns are envisaged within the NAP-AMR and have already been rolled out in India. Yet reports suggest a degree of confusion among members of the Indian public around some messages in the campaigns conducted to date. 113 Further media campaigns can be pursued on a sustained basis by relevant government agencies; perhaps in conjunction with NGOs and civil society organisations. Techniques and principles used successfully in other countries can also be considered and possibly applied in future campaign designs in India. 114
Other interventions implemented outside India have sought to ‘nudge’ stakeholders through forms of audit and feedback. 115 Adopting an approach grounded in behavioural science, 116 and following successful pilots in 2014–2015, the Chief Medical Officer for England sends an annual feedback letter to individual General Practitioners (GPs) in different GP practices with high antibiotic prescribing rates. 117 The letters are tailored according to GP practice prescribing rate, change in prescribing over time and whether they were previously sent feedback. The intervention has supported GPs to reduce their prescribing further by providing feedback on practice prescribing rates, offering encouragement and suggesting practical actions in a clear and succinct manner. 118 Governments may also introduce financial incentives to reduce prescription of antibiotics. For instance, in 2015, NHS England introduced rewards to clinical commissioning groups for a percentage reduction in antibiotic prescribing. 119
As the measures described above target inappropriate prescribing by physicians, they would not appear to be of immediate help in tackling situations where Indian patients are bypassing doctors and obtain antibiotics without a valid prescription from a pharmacy directly. Nevertheless, the general ideas behind these physician-centred approaches (i.e. the provision of targeted information, financial incentives, guidelines and advice) could be adapted and repurposed to influence pharmacists’ behaviour.
Bespoke interventions have sought to incentivise patients to visit physicians by building extra value into the process of physician diagnosis and prescribing. After receiving input from stakeholders in India and Kenya, a human-centred design approach led to the development of a digital platform called ‘Smart Prescription’. 120 This tool allows prescribers easy access to international antibiotic prescription guidelines and protocols. It was said to increase physicians’ confidence during the process of diagnosis. Further benefits are offered to patients by way of information on symptom management and reminders to take their medicine sent via text message, as well as an e-prescription that can be filled at supporting pharmacies. These features were said to improve patient understanding of their diagnosis and prescription and enhance the desire to obtain a prescription. 121
Advances in diagnostic technologies might also be utilised. There are several point-of-care (POC) approaches to diagnostic testing for bacterial infections in use or in development. For example, in 2014 and 2015, a sore throat ‘test and treat’ diagnostic service for streptococcus group A was piloted at community pharmacies in England. 122 Pharmacists who received additional training could conduct on the spot swab tests and were permitted to supply antibiotics according to predefined dosing schemes. Stakeholder engagement will help identify possible cost concerns and other barriers to uptake of POC diagnostic testing in the Indian context.
The Antibiotics Smart Use (ASU) Program was introduced in 2007 in rural Thailand to reduce unnecessary prescriptions of antibiotics for conditions that do not require antibiotic treatment. 123 Interestingly, one strand of the multifaceted Thai ASU, which engaged patients through a behavioural change intervention in situ at pharmacies, shows promise as a way to mitigate the financial disadvantages of AMR initiatives for pharmacists. Patients complaining of a throat infection were asked to self-diagnose by getting them to examine their own throat using a tongue depressor, mirror and white light illuminator. 124 Patients would compare their own throat to photographs of typical viral and bacterial throat infections with reference to four clinical criteria. If bacterial infections were not found, pharmacists would sell alternative treatments to alleviate symptoms. Further stakeholder engagement around these types of interventions can help quantify the financial interests at stake and encourage the transition to viable, alternative business practices.
Accreditation programmes may also help encourage behavioural change at pharmacies. 125 A public–private partnership in Tanzania sought to improve access to quality medicines and pharmaceutical services in rural areas. 126 Pharmacies that participated in the scheme received training and education on AMR and appropriate use in antibiotics, as well as benefits such as training in business skills and access to microfinance. 127 A key incentive for owners to become accredited was that they would be legally authorised to sell a limited number of antibiotics that would otherwise require a doctor’s prescription. A review of this intervention reported positive results, 128 but issues such as the retention of pharmacy staff who have undergone AMR training would need to be addressed to ensure long-term sustainability. 129
These kinds of initiatives could form the basis of interventions in India. Alternatively, original interventions could be developed alongside stakeholder input. The space opened by the NAP-AMR for innovative and imaginative design should be used to full advantage. Furthermore, and following the broader definition adopted in this review article, 130 it may be helpful to view resulting interventions as a form of ‘regulation’ in their own right, as opposed to mere measures that help support the legislative framework. Indeed, such interventions may have greater impact than legislation in promoting the internalisation of norms and behavioural change. Due care and attention should therefore be taken in their design and implementation and ongoing monitoring put in place to evaluate their effectiveness and detect any unintended consequences. 131 More generally, the sharing of information and experiences within and between countries will help governments and stakeholders resolve problems and adjust to using less familiar modes of ‘decentred’ regulation. 132
Conclusion
Misuse of antibiotics is one of the primary reasons for the emergence of AMR in LMICs including India, which is one of the world’s largest consumers of antibiotics. Misuse could result from the actions or inactions of different actors including pharmacists as dispensers of antibiotics, medical practitioners as prescribers (and sometimes dispensers) of antibiotics, consumers of antibiotics, as well as manufacturers, sellers and distributors of antibiotics who also seek to influence the practices and behaviour of the above-mentioned actors.
This article reviewed the existing binding and non-binding regulatory instruments relating to OTC sales of antibiotics for human use in India, directly or indirectly, that could contribute to the optimum use of antibiotics and address the AMR challenge. It found that the Indian government is currently working to close a gap in the regulatory framework for sales of antibiotics relating to e-pharmacies. Outside these specific areas, formal rules require a prescription from an RMP for sales of antibiotics and specify the regulatory actors charged with enforcement. In addition to considering proposals for revising the classifications of different antibiotics according to tiered schedules, the government could move to expand the scope of the regulatory framework governing the education and practice of pharmacists to incorporate provisions relating to sales of antibiotics specifically and AMR generally.
The article also emphasised the importance of including a broader range of stakeholders within the overall regulatory framework, the potential role of non-binding regulation and the need for stakeholder input into the design of regulatory initiatives. Both top-down and bottom-up approaches are needed in this context. 133 While the challenges for effective regulation in LMICs such as India are significant, they may be addressed if researchers, policymakers and regulators combine forces to advance knowledge and practice around AMR NAPs and their implementation.
Footnotes
Author’s note
Anita Kotwani is also affiliated with Department of Pharmacology, University of Delhi, India. Lovleen Bhullar is also affiliated with Birmingham Law School, University of Birmingham, UK. Jyoti Joshi is also affiliated with Amity Institute of Public Health, Amity University, India & Center for Disease Dynamics, Economics & Policy (CDDEP), India.
Acknowledgement
The authors would like to thank Dr. G. L. Singhal, Ex-Haryana State Drug Controller, for reviewing an earlier draft of this article and giving inputs regarding the DCA.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Economic & Social Research Council [grant number ES/S000321/1] and the Department of Biotechnology, Government of India [grant number BT/IN/Indo-UK/AMR/04/AK/2018-19]. The views expressed within this article do not necessarily reflect the views of the funders.