
Abstract
Robert Hamilton (1749–1830) was born in Coleraine, Ireland, attended medical school in Edinburgh, Scotland, served in the British army and practised in South-East England. In order to differentiate him from his contemporary and namesake, Hamilton is identified by having worked in Ipswich, Suffolk and Colchester, Essex. This submission considers Hamilton's biography, his 1787 book on the British regimental surgeon and his ideas therein about professionalism. Central to his concept of professionalism is ‘tenderness’, a notion that broadly equates to empathy. He notes that tenderness brings improvement in clinical outcome and he has the foresight to recognise nurses as key to such care. The authors explore the concept of ‘consulting in the dark’, i.e. without access to clinical investigations. This is exemplified by doctors of the eighteenth century and earlier. Today general practitioners must still be comfortable ‘consulting in the dark’, e.g. when attending a patient's home. Hamilton's biography offers a further example of ‘consulting in the dark’: In later life, he lost his vision but continued to practise successfully. Central to his gift of consulting ‘in the dark’ was likely to be ‘tenderness’ for his patients, expressed through language and gentle touch. Hamilton's entreaty for ‘tenderness’ contrasts with modern medical education where reliance upon clinical tests, technology and pharmacology risksblinding young doctors towards patients and their lives.
Keywords
The role of empathy in clinical consultations has been the focus of much research over the past quarter century. 1 Compassionate and collaborative consultations have been found to be associated with better care, greater adherence to treatment, and improved clinical outcomes. 2 Doctor empathy is manifested in consultations in various ways including body language, facial expression and word choice. Examples of phrases that convey empathy in consultations are included in Table 1. 3 Enacting empathy serves to reflect the content of the patient's story, identify and calibrate the patient's emotion as well as to request and accept correction. 4 We believe that more about the notion and function of empathy might be learned through a historical perspective, in particular from when doctors had to consult in the complete absence of clinical tests and highly effective treatments.
Examples of phrases that convey empathy in a consultation. From the GP education website of Dr Damian Kenny (see references for source).
Summary of characteristics of ‘tenderness’ according to Hamilton.
Frontispiece to Hamilton's text. Image courtesy of the Wellcome Trust and Leeds’ University.
The Royal College of Physicians at Warwick Lane, London. Munk's Roll notes that Hamilton was ‘was admitted an Extra-Licentiate of the College of Physicians 8th January, 1784; and a Licentiate, 30th March, 1795’. Image courtesy of the Wellcome Trust.
Sir John Pringle. Stipple engraving by W. H. Mote after Sir J. Reynolds, 1774. Image courtesy of the Wellcome Trust.
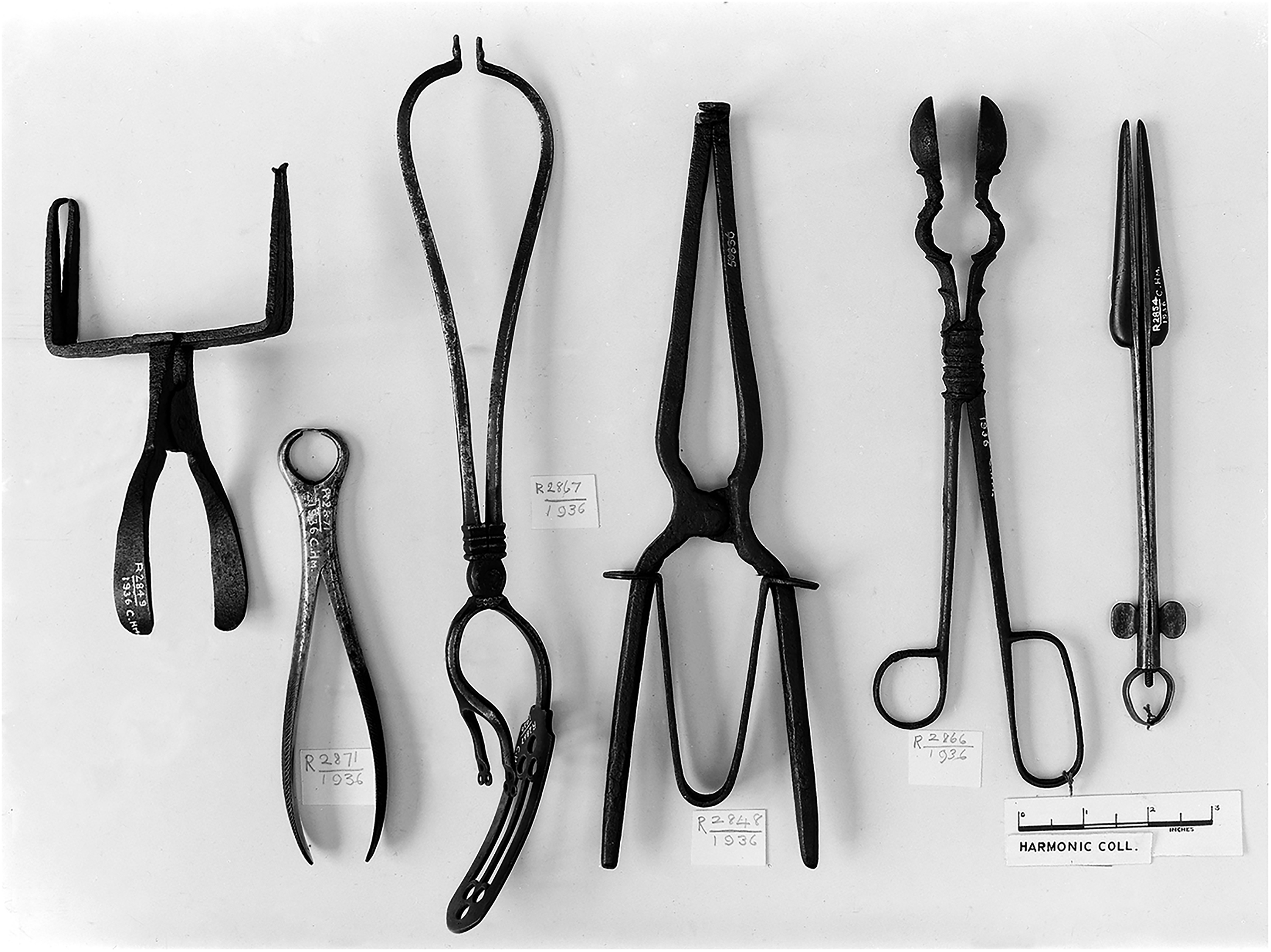
Surgical instruments from the fifteenth to eighteenth century including forceps, bullet forceps, surgical clamp and bivalve dilator. Image courtesy of the Wellcome Trust (Harmonic collection).
Modern doctors can learn from the experiences, challenges and skills of doctors of yesteryear whose practice was reliant upon their own communication and clinical skills. The absence of modern scientific medicine meant that their skill in consultation and observation was finely honed. This art was acquired through apprenticeship under the instruction of a master and practised regularly, not least inside patients’ homes on daily ‘rounds’. Key to this was attentive listening and constructive advice about rest, mobilisation, nutrition, fluids and basic medications. These often combined to take the form of a ‘regimen’ prescribed by the doctor (that also served to ‘buy time’ for the natural healing process to work). 5 Undoubtedly, doctors of yesteryear were also experts at promoting the placebo effect, including the notion of ‘doctor as drug’, 6 and ‘enacting the persona of the doctor’.7,8 This approach to consultation is something that we term ‘consulting in the dark’. Today ‘consulting in the dark’ may be illustrated by a general practitioner who attends a patient's home: in the absence of immediate access to clinical investigations the doctor must, instead, must find human-centred strategies to support the patient. 8 Consulting constructively ‘in the dark’ is in stark contrast to modern hospital medicine where tests, technology and medication abound. 8 One key strategy for consulting ‘in the dark’ is empathy.
Empathy describes the capacity to understand and share another individual's emotions and perspective. 9 Sympathy, on the other hand, is the ability to have an affective reaction to another person's suffering. 9 Despite much energy expended upon the study of empathy, it is a term that dates to only the beginning of the twentieth century. 1 Equally surprising perhaps is the apparent absence of enquiry into the historical origins of empathy in the clinical consultation. To that end, this article considers empathy within one early medical text and a clinical context where its presence might be least expected: guidance for the eighteenth-century regimental surgeon (see Figure 1). In this guidance, the term ‘tenderness’ appears key. The Oxford Learner's Dictionary defines tenderness as ‘the quality of being kind, gentle and loving’. 10 It also lists ‘toughness’ as an antonym, indicating another aspect of tenderness relevant to medical practice: softness in physical touch. From an analysis of Robert Hamilton's text, it can be concluded that as today's medical practitioners are familiar with the term ‘empathy’, their eighteenth-century surgical equivalents would have been aware of the concept of ‘tenderness’.
The role of the British regimental surgeon
The primary aim of the Army Medical Services was to maintain the health of the soldiery and, consequently, to conserve manpower through early return to military duty. In the Georgian era, many young doctors (especially those educated in Scotland) joined the British military services for opportunities to gain first-hand clinical experience, in particular surgery. A notable example was John Hunter (1728–1793) who served as staff surgeon to the 1761 expedition to Belle isle, Brittany.
11
Similar reasons for signing up continued into the Victorian era: so much so that the English explorer Sir Richard Francis Burton (1821–1890) noted how the ‘regularly graduated surgeons … start to “finish” themselves upon the frame of the British soldier’.
12
Other reasons for surgeons to join were regular pay that included furlough and a pension. Insight into the care provided to the British soldier might be gleaned from the following letter to the Examiner in 1816: ‘[The soldier's sister], on visiting him in the hospital, was told by him that he had received an injury in his arm, and that he should not see her any more. He died soon after. Previous to this, he had complained of severe pain in his arm, which he attributed to the extent of the incision made when he was bled, which is described… as being large enough to admit the first joint of the little finger…. It has been given out that hard drinking occasioned [the soldier's death] ; but this he strongly denies [sic] ; and he adds, that the Sister of the deceased was refused admittance to see the remains, till the body was so changed that she with difficulty recognized it to be her brother's, and the blood was oozing through the shroud’.
13
Upon the battlefield, conditions were even more basic. The surgeon's station was located close to the frontline and his duties harsh.
14
The period considered here pre-dates the advent of anaesthetics, sterile surgery and antibiotics. The role of regimental surgeon indeed came with no lack of practical experience: surgery (e.g., amputation) was plentiful and rapid, unpleasant for both parties, and lacking space for ‘tenderness’. The following insight into the battlefield duties of the eighteenth-century British army surgeon is offered by Harold Ellis: ‘Hunter was singularly unimpressed by his fellow surgeons on Belle Isle; the military surgeons of that period were for the most part ignorant, poorly trained and certainly badly paid. The standard treatment of war wounds was deplorable. It comprised wholesale blood-letting together with wide opening or brutal dilatation of the wound, extensive probing to search for the missile, and liberal recourse to amputation’.
11
Whilst the title ‘surgeon’ points to the undertaking of operations, the office extended more widely to include generalist treatment for soldiers: injuries, fractures, swellings and other external (often skin) conditions were the province of the surgeon. 15 Again, Hunter offers an example of the breadth of clinical activities undertaken by the eighteenth-century surgeon. Later interventions undertaken by surgeons also included procedures such as vaccination. 16 The present article highlights that the role of the military surgeon went beyond operative procedures and management of other physical conditions, to include caring for the psychological wellbeing of patients.
The text considered below was written in 1787 by Robert Hamilton (1749–1830) and entitled: The duties of a regimental surgeon considered: with observations on his general qualifications, and hints relative to a more respectable practice and better regulation of that department’. 17 The title points to the author's intention of highlighting medicine as a caring profession and the importance of self-regulation. In this Hamilton draws attention to many practical challenges facing the army surgeon, not least the need for soldiers to have proper accommodation and the surgeon's station to be well equipped. Central to his thesis, however, is the practice of ‘tenderness’, a notion that equates to today's term ‘empathy’.
Biographical summary: distinguishing between namesakes
Hamilton was born in Coleraine in County Londonderry, Ireland, and was of Scottish descent.
18
Hamilton qualified Doctor of Medicine at Edinburgh on 24 June 1780. Hamilton's entry in the Dictionary of National Biography records his military career: ‘on 27 July [1780]… he gained a warrant as surgeon's mate of the 10th foot. He first practised medicine at Dorchester, and thereafter, while serving as a surgeon's mate, at Luton. In 1784 he became a member of the Royal College of Physicians [see image 2], and about the time he left the 10th foot (1 May 1785) he established a practice in Ipswich. He returned to the service briefly in 1795 as physician to the forces in the West Indies, but failing eyesight, in the wake of a rheumatic affliction, forced him to resign’
19
His 1780 appointment is not recorded in The Roll of Commissioned Officers in the Medical Service of the British army. 20 It is important to note that the preface to Hamilton's book confirms that this Robert was indeed the same individual, i.e. who practised at Ipswich, Suffolk, and Colchester, Essex, and not his namesake (Robert Hamilton, 1721–1793) of King's Lynn (Norfolk). 21 This is of relevance because all these geographical areas are located in East Anglia. Indeed, the Wellcome Trust currently attributes the book considered here to Hamilton's namesake at King's Lynn. The entry for Robert Hamilton of King's Lynn notes that he was born in Edinburgh and appointed to the Royal Navy, with no mention of army service. 22
In 1782, Hamilton published an early text on influenza which was dedicated to Lieutenant Colonel Cathcart of the 10th Regiment of Foot. 23 It is of note that Hamilton (of Ipswich) also served as Physician to the Surrey Dispensary, London. 24 Hamilton's book records his affiliations in 1787: ‘Of the Royal College of Physicians, London; Member of the Medical and Physical Societies of Edinburgh; and of the Medical Society of London’ (see Figure 2). Works from Hamilton's pen on the welfare of soldiers’ sick wives and abolition of the slave trade testify to his humane character. 14 A final aspect of his later life lays bare Hamilton's mastery at communicating with patients: despite losing his eyesight and remaining blind for over 30 years, he continued successfully to practise medicine. 14
An entreaty for ‘tenderness’
In his preface, Hamilton shows that a key function of his book is to promote humanity in the regimental surgeon: ‘If novelty, therefore, be any recommendation, the following work has this to plead in its favour: but we hope it has more; its object is utility, while it inculcates humanity towards a class of men, whose situation, at best, is but comfortable, and yet to whom the community are under obligations. I mean the Soldiery…’ Chapter Three is entitled ‘Of the Surgeon's Qualifications; and of his Tenderness to the sick Soldiery’. This article examines chapter three (42 pages) to identify guidance related to consultation approach and management in the context of psychosocial illness.
Hamilton starts by highlighting the overarching challenge facing the doctor and the importance of one's reputation: ‘The situation of the medical man is of all others the most delicate; and as it is a public line of life, the world is ever ready to make free observations on the conduct of those engaged in the profession. If these were always the result of deliberation, it would be of less moment: but this is not, on all occasions, the case. A trifle may gain, as a trifle may often lose a practitioner a reputation….’ (p. 94).
The chapter proceeds to emphasise the need for measures to avoid such a reckoning. These preventive steps amount to an embryo of what today would be termed defensive medicine; the allusion to ‘all our actions’ echoes the modern scrutiny of doctors’ conduct and a focus on professionalism. 25 Central to Hamilton's reasoning is exercising ‘care we ought to observe, and the circumspection we should use in all our actions’ (p. 94). He goes on to illuminate some of these measures. For example, other chapters in the book highlight key pitfalls to avoid including the dangers of excessive socialising with fellow officers and vice arising from problem drinking as a particular issue for regimental surgeons.
Next, he offers the primacy of medical education and surgical training. The regimental surgeon's duty to study is emphasised and reinforced with a reminder of his responsibility for a battalion, i.e. more than 700 soldiers. What is more, he is answerable to ‘his country, his King, and his conscience’ (p. 95). Hamilton highlights the well-known notion that many British army surgeons of the day had received little training in military medicine. Indeed, he acknowledges that others received no medical education at all: ‘Many… who enter into the army in this line [i.e. surgery], never were at all within the limits of an university, nor ever had an opportunity of hearing, in any medical school a single lecture on the subject’ (p. 99). Although it is likely many assistants had previously been apprenticed to a surgeon or an apothecary, Hamilton suggests otherwise: even ‘a common soldier from the ranks’ (p. 100) might be appointed to a vacancy for a surgeon's assistant.
Hamilton acknowledges that the army is ‘a good place for improvement in medical knowledge’ (p. 101). He also recognises the value of clinical learning through first-hand experience. In so doing he quotes Sir William Temple (presumably the English diplomat, 1628–1699), stating that ‘though a man may grow learned by other men's thoughts, yet it is from his own thoughts, as well as experience, that he will grow wise’ (p. 101).
‘Tenderness’ towards patients and its benefit
The chapter constitutes an early attempt to promote what today would be called ‘psychosocial’ medicine in the army surgeon. It goes deeper, however, recognising the importance of personalised consultation skills in the care for sick soldiers. The account confirms that the contemporary army surgeon (in addition to consulting, dressing and operating on and off the battlefield) had to manage patients with physical and psychological illness. Hamilton highlights the importance of – and benefits for – the surgeon who cares for patients with humanity and that such an approach affords clinical benefits. Again, he suggests that this approach has its roots in education, such that it may ‘throw a lustre, and a kind of dignity around the [medical] service’ (p. 102). He highlights, in line with this age of medical enlightenment, the importance of the ‘scientific surgeon’ and advocates for ‘a liberal education’ to prevent ‘quackery [and] narrowness of thinking about medical subjects’ (pp. 102–3). As part of a desire for a move towards more scientific medicine, he commends Sir John Pringle (1707–1782, see Figure 3) – acclaimed today as the father of military medicine – to be the ‘true honour [of the] military medical profession’ (p. 104).
Through Hamilton's entreaty for ‘tenderness to the sick soldiery’ (p. 104) he asserts that ‘tenderness and humanity ought strongly to mark the character of every one engaged in the practice of physic’ (p. 104). As such, he is pointing to the importance of empathy as the hallmark of professionalism in the regimental surgeon. He also hints at humility. The ‘practitioner's sympathy’ should emerge from an ‘acquaintance with the frailty, and miseries that inevitably await the life of man’ (p. 104). He goes on to call for a ‘sympathetic disposition’ (p. 105) which constitutes ‘one step towards the cure’ (p. 105). As part of this appeal, certain consultations skills are mentioned. He advocates ‘a soft, and tender tone of voice’ (p. 109) and that the surgeon should visit his patient regularly (p. 113).
The surgeon should come across like ‘a friend interested in his recovery’ and that as a result ‘a calmness, quietude of mind, and confidence will follow [that is] essential to his future health’ (p. 105). The benefit of ‘those other little offices of attention which, if in reality they do not good, at least quiet the mind… and may even have their effects in co-operating with the doctor's advice’. What is more, the surgeon's ‘prescriptions will now … be more cheerfully and strictly complied with’ (p. 105).
By pursing the sympathetic approach above, he notes that ‘the noblest mind is always the most merciful, the most capable of ‘tenderness’ and pity’ (p. 107). The regimental surgeon must then seek the ‘approbation, and favour of the soldiery’ (p. 115). As a corollary, he cautions against the ‘brutal’ ‘roughness’ of surgeons who do not care for patients in this way and counsels against ‘harsh expressions (p. 107).
The importance of nurses in patient care
Hamilton was an early advocate of nursing care, recognising in his book the contribution of a tender and caring nurse in facilitating the recovery of a patient: ‘Another difficulty that the surgeon, perhaps, labours under, is the want of a good, careful, and tender nurse. A very great deal depends on this servant. it is altogether impossible for the surgeon to be present with his patient on all occasions, when he wants such assistance as nurse -tender can give; and, was it even convenient, and he willing, he cannot be so useful in this respect as a nurse. She ought to be with the patient on all occasions, and almost constantly; since it is her duty to administer both drink and medicines with care and punctuality…’ (p. 28).
Hamilton's perspective on nursing pre-dates the achievements of Florence Nightingale (1820–1910) and Mary Seacole (1805–1881) who cared for soldiers from the war in the Crimea (1853–1856). His ideas are in keeping with modern-day perceptions of nurses as skilled carers: ‘For this is more the nurse's than the surgeon's province, since it may not be in his power to visit him [the patient] above twice a day at most, while the nurse or orderly is, or ought to be, constantly present, and from habit, and practice in such sort of attendance, which, to some, may seem ‘trifles as light as air’, but, in reality, are of great moment in the recovery of health, she becomes far more expert in, and tender, than either the surgeon or others less accustomed to such things generally are’ (p. 31).
‘Chronic’ illness: a case of nostalgia
Hamilton then goes on to describe ‘chronic complaints, where the patients, though kept in the hospital, are not confined to bed’ (p. 115). From his descriptions, it soon becomes apparent that his advice relates to chronic psychological illness.
In a case of ‘nostalgia’, Hamilton goes on to advocate what he calls ‘a sort of deception’ that the surgeon may be called upon to practise (p. 120). The case relates to a Welshman called Edwards in barracks in the North of England in 1781. Having been a soldier only a few months, ‘a melancholy hung over his countenance, and wanness [sic] preyed on his cheeks. He complained of universal weakness, but no fixed pain. A noise in his ears, and giddiness in his head. Pulse rather slow than frequent… appetite was much impaired… slept ill, and started suddenly out of it, with uneasy dreams’ (p. 121). After a few weeks his situation had not improved. Edwards ‘scarcely took any nourishment… became indolent, seldom sat up at all, was constantly dozing .. sighed deeply and frequently; nor could his attention be diverted to any external object’ (p. 122). After three months of treatment failure, his face showed features of consumption. A nurse then mentioned that Edwards’ conversation was solely focused upon his family home. Intriguingly, Hamilton notes that he had never previously seen a case of homesickness. Hamilton's 'deception' lay in his offer to Edwards: ‘furlow’ [sic] at home of six weeks duration (that had yet to be approved by the senior officer). At this prospect, Edwards swiftly improved. The furlough was ultimately approved by the senior officer. Such ‘deception’ Hamilton notes was only indicated where ‘absolutely necessary’ in order ‘to allay inordinate action of the mind, raise the drooping spirits, and remove inquietude, by confirming the patient's hopes, and seconding his wishes, in promising something on which he may have riveted his affections, and placed his happiness’ (p. 120).
A case of a broken heart
In order to emphasise the impact of the mind on the body, Hamilton goes on to describe a case from the Dutch surgeon Nicolaes Tulp (1593–1674): ‘a young Englishman, who met with a refusal from a lady’ (p. 133). Presented as an example of ‘melancholy passions’ (p. 132), his symptoms included becoming ‘perfectly rigid, and motionless, sitting in the same attitude with his eyes open, and appeared rather like a statue’ (p. 133). This clinical presentation resembles catatonia but the remedy swiftly reveals the cause. When told that ‘his mistress yielded to his passion’ the patient recovered immediately.
In terms of managing patients with chronic symptoms of psychological illness, Hamilton hints at the importance of practical psychosocial solutions. He advocates that the surgeon should ‘grant them as much indulgence as possible, with safety’ (p. 115). Again, he points to the importance of maintaining morale in patients. Such acts may ‘really conduce to the cure, by keeping their spirits up’ (p. 115). In these cases, he urges: ‘exercise will keep up the languid secretions, induce cheerfulness, and render their situation more happy’ (p. 117).
Once more, Hamilton appeals for better communication with patients. Recognising that desertion may ‘sometimes follow too great a licence [i.e. from excessive flexibility on the part of the surgeon]’ (p. 115) he advocates that regarding refusals to leave the regimental hospital (e.g. requests for outdoor exercise among patients suspected of planning to abscond) ‘let it be done with a seeming concern and reluctance’ (p. 116).
Discussion
Hamilton's primary appeal is for greater professionalism among regimental surgeons. Within this, he calls for empathy, humanity and humility. Indeed, he effectively offers a definition of empathy: a ‘sympathetic disposition’ among practitioners as well as describing physical qualities such as a sensitive tone of voice. This is in stark contrast to the cold, clinical professionalism commonly associated with the efficient battlefield surgeon of the eighteenth century. As a former army surgeon, Hamilton must have witnessed examples of harsh practice and seen the clinical benefits earned by the caring doctor. It is of note that Hamilton's army service was only a small period in his life (about five years). Nevertheless, he is quick – indeed passionate – in his entreaty for regimental surgeons to ‘trial’ the approach of ‘tenderness’ in their practice: ‘I have seen the brutal, half-savage disposition [i.e., ‘the privates of real bad character” in the army] softened down into humanity, by tender and kind usage, or even expressions, in his illness. Let the trial be only made, and I will answer for its success’ (p. 111).
Hamilton's book may be the first in English to place empathy as core to professional medical practice. ‘Tenderness’ is presented as a virtue of the ‘good’ army surgeon and key to maintaining a positive reputation. He also recognises that the office of regimental surgeon can be harder for doctors with a soft disposition. One may extrapolate from this assumption that ‘tender’ doctors are more likely (in modern parlance) to ‘burn out’: ‘we shall now enquire a little into some of difficulties which a regimental surgeon has to encounter in the right discharge of his duty. These indeed we shall find by no means few, and if he be a man of a humane and tender disposition, are such as will cause him many hours uneasiness and disquietude’ (p. 14).
The key theme in his chapter on ‘tenderness’ is the importance of surgeons who care and express concern towards their patients. He offers a humane basis to his entreaty, concluding that ‘the more our minds are disposed to do good to mankind in general, the more will be inclined to exercise virtue of tenderness and care’ (pp. 135–136). Behind this, Hamilton makes clear links between practising empathy and a strong Christian faith: ‘[The regimental surgeon] should reflect on the nature of his charge, its great importance, and how culpable he must appear, both before God and man, in the neglect of any part of his duty’ (p. 95).
Hamilton also appears to be making a call for regimental surgeons to recognise that psychosocial illness is a common and important part of their caseload. He does not, however, attempt a numerical estimate of how common such patients were. Again, he calls for surgeons to respond in a humane way by offering psychosocial or lifestyle (e.g. exercise and schooling) measures. In so doing, Hamilton concludes that such cases prove the ‘vast influence the passions have over the body, and how much it is incumbent on the practitioner to study the springs of the mind… to deduce the causes of many diseases’ (p. 133). His work hints at later failings of the British army to care for psychologically unwell soldiers, for example those with ‘shell shock’ in the first world war.
Hamilton's wider appeal for ‘tenderness’ may also be interpreted as a call for better communication skills among army doctors. In the text, he urges regimental surgeons to engage with their patients, be observant, understand their perspective and be seen to compromise, even where that might mean breaking military rules. He clearly valued instilling positivity and hope in his patients. His call for ‘tenderness’ and for better care of psychologically unwell soldiers highlights the regimental surgeon's function as a clinical generalist and not just a high-speed amputator on the battlefield (see Figure 4 for examples of surgical instruments).
Hamilton appears to be drawing upon his own observations in an era that lacked modern clinical investigations and drugs. Nevertheless, he grapples with key challenges that doctors still face today: acting in the best interests of the patients (rather than resorting to purely defensive medicine), recognising that trust turns upon a ‘trifle’ (i.e. brief moments or actions), maintaining caring relationships, dealing with patients’ as people, and embracing social (rather than just technological) interventions. Hamilton's forward-thinking approach must be viewed in the context of the arduous circumstances in which he lived and practised. Soldiers faced hardship, privation and death. Civilian life was not necessarily much easier. Although figures are unclear, suicide (including in military surgeons 26 ) was not unknown at the time. What is more, the regimental surgeon could act with impunity towards the soldiery. In this testing landscape, Hamilton's work illuminates (not least for the medical student or trainee) important and timeless aspects of the what it means to be a doctor.
Conclusion
This article contributes to wider research into the importance of emotion in eighteenth-century surgery. 27 Robert Hamilton's life and book bespeak a caring clinician who recognised the centrality of empathy within medical professionalism. Unfortunately, his profession and region of residence overlap with another notable doctor of the same name. That coincidence has made it problematic to expand further upon his biography in this article.
Hamilton's call for compassion and care are far ahead of his time (see Table 2). This is most evident in his promotion of ‘tenderness’, its positive impact upon clinical outcome and his recognition of the value of nurses in patient care. 28 His entreaty is as relevant today as it was 250 years ago. His choice of the word ‘tenderness’ (i.e. above ‘sympathy’ or other terms) suggests that modern medical teachers could make greater use of the expression. ‘Tenderness’ may be more comprehensible to medical students/trainees and appeal more directly by drawing upon their natural communication skills and propensity for caring. ‘Tenderness’, thus, emerges as a phenomenon that is more human and more applied than empathy. That is because it captures not just emotion and empathic response but also the importance of care in other ways, for example examining patients in a tender way.
Perhaps the most telling aspect of Hamilton's biography is his practice in later life as a doctor with visual impairment. The medical literature lacks a history of surgeons with physical disability 29 and Hamilton's life offers insight into how doctors adapted to such circumstances. That is because Hamilton appears to have sustained a successful clinical practice, almost certainly due to his ‘tenderness’ and ability to connect with patients. One reason for this achievement undoubtedly lay in the value of listening, touch and smell in making a diagnosis. Learning to appreciate these cues with patient remain essential skills for modern doctors (and ones likely to be overlooked during ‘teleconsultations’).
Hamilton's entreaty stands in contrast to contemporary notions of the Georgian doctor as rich and aloof. Indeed, Hamilton's loss of vision probably connected him even more closely to his patients. If so, his later life offers even greater insight into what it means to consult ‘in the dark’: without being able to see his patients clearly, Hamilton's consultations must have been founded upon careful listening, profound gentleness and sensible advice. Such ‘tenderness’ transcends the sense of sight and touches upon what it means to be human. Developing this gift of connecting with another human by communicating a doctor's deep concern for their wellbeing is a skill that all medical students should learn. That includes the notion that by doing more and more clinical tests doctors may ultimately lose sight of their patient and their problems.
Footnotes
Acknowledgements
We thank the following who kindly read and commented upon drafts of this article: Mr Mick Crumplin, Prof JE Cooper and Mrs ME Cooper.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.