
Abstract
Objectives:
People with visual impairment participate in less physical activity than sighted people, and may have been further affected due to the COVID-19 pandemic and associated social distancing and lockdown measures. The aim of this study was to evaluate the use of mat-based group Pilates as a possible ‘return to sport’ intervention for adults with visual impairment.
Methods:
A 10-month intervention of community-based instructor-led mat-based group Pilates sessions was conducted with 14 participants with visual impairment. Measures of quality of life and balance confidence were collected at the start and end of the intervention. In addition, qualitative surveys and participant interviews were conducted pre- and post-intervention to gather data about the participants views and lived experiences of participating in the session.
Results:
There were no statistically significant changes to overall quality of life or balance confidence over the 10-month intervention period, but participants started with good scores with limited scope for improvement. Participants scored lower on the environmental domain (p = .042) after the intervention, which may be due to services struggling to return to pre-pandemic levels. Reflexive thematic analysis identified themes relating to becoming a community, (re)gaining competence, and developing independence with the intervention having a positive effect on both physical and mental health.
Conclusions:
Despite no quantifiable positive changes in balance confidence or quality of life, the qualitative analysis identified that the participants valued and benefitted from the intervention and found it helpful to their overall function as well as wellbeing and mental health. This suggests that mat-based group Pilates classes as a physical activity intervention is useful in this population and warrants further research.
Introduction
In the United Kingdom, approximately 340,000 people are registered as visually impaired (NHS, 2022). Physical activity is a significant predictor of quality of life in adults with visual impairment, and correlates with increased life satisfaction (Łabudzki & Tasiemski, 2013). Yet on average, adults with visual impairment complete less physical activity and exercise compared to the general population (Holbrook et al., 2009). This population group have been further affected by the COVID lockdown and social distancing measures implemented in the United Kingdom since 2020, which may contribute to worsening health-related outcomes (Strongman et al., 2022). In addition, people with visual impairment report considerably more moderate and severe loneliness than the general population which may further affect life satisfaction (Brunes et al., 2019). Barriers to participation in recreational physical activity include lack of transport and dependence on others (Jaarsma et al., 2014), physical barriers, and safety concerns (Lindsay et al., 2021). These factors all suggest that an effective method to encourage people with visual impairment to return to physical activity post-COVID, reduce the barriers to participation, and maintain this level of participation thereafter, may improve quality of life and general wellbeing in people with visual impairment.
Whereas previous exercise interventions with people with visual impairment have had a focus on balance, mat-based group Pilates classes have not been evaluated as a specific training method for this population (Sweeting et al., 2020) despite showing increased dynamic balance, quality of life, and mental health in sighted people (Campos et al., 2016; Fleming & Herring, 2018). The aims of this research were to evaluate the extent to which mat-based group Pilates classes improve quality of life and balance confidence in people with a visual impairment and to evaluate this as a method of long-term behaviour change. The primary research question for this study is as follows: Are mat-based group Pilates classes an effective method in engaging people with visual impairment to return to physical activity following the COVID-19 lockdowns in the United Kingdom?
Methods
The UK-based sight loss charity CamSight provided mat-based group Pilates classes to their service users as a method of returning to physical activity following the easing of lockdown. Following local institutional ethical approval, 14 participants (seven male, seven female, age = 65.9 yrs ± 12.6) from the CamSight service users, adults with visual impairments, were recruited to participate in a 45-min weekly, community-based instructor-led mat-based group Pilates classes. The classes were managed to ensure maximum accessibility for this participant group, the same room at the venue was used each week and mats were placed in the same places within the room. No music was played during the session and participants were provided with a chair if required to help with balance. Volunteers from CamSight were available to guide people to the room and to their mats if required, and participants were asked to arrive 15 min before the class so they could be guided to their place if needed. The volunteers and instructor all introduced themselves to participants when they arrived, and the instructor wore similar, brightly coloured clothing each week to increase visibility.
Participants had a range of visual impairments, 10 are registered as severely visually impaired, acuity of <3/60 with full visual field, or <6/60 with severe reduction of field (e.g., tunnel vision), or >6/60 with very reduced field of vision (Royal National Institute for the Blind [RNIB], 2019). In addition, current levels of physical activity within the participants varied, and their experience in previous Pilates classes was also variable, with two people having taken part in mainstream mat-based group Pilates classes aimed at sighted participants. Sample size was limited due to the venue and provider COVID-19 regulations in place at the start of the intervention (social distancing). No incentives were provided for taking part in the research, but the classes were provided free of charge to the participants. The classes ran from September 2021 until July 2022, and participants were asked to record their thoughts on the sessions through online questionnaires during the period of the intervention. In addition, telephone or in-person interviews were conducted pre- and post-intervention to capture data on quality of life and balance confidence and to allow participants to respond to open-ended questions about their lived experience of participation in the sessions. Online and telephone methods were included due to the ongoing COVID restrictions at the time of the start of the sessions, and to ensure maximum accessibility for the participants.
Quality of life was measured using WHOQUAL_BREF which has been used in previous studies with people with visual impairment (Soares et al., 2019) and is based on the answers to 26 questions spanning four domains: physical health, psychological, social relationships, and environment. Data were collected at the start and end of the research study through telephone interviews. As the classes continued after the period of the research study, we did not collect further data to evaluate retention beyond this. In the interviews, the standardised instructions were read to participants, and they were able to respond using Likert-type scale options, for example, participants were asked, ‘How would you rate your quality of life?’ and could respond, ‘Very poor’, ‘Poor’, ‘Neither poor or good’, ‘Good’, ‘Very good’. When analysing and scoring the results, the data collected were cleaned and prepared according to the WHOQUAL_BREF guidelines (World Health Organization, 2012).
The participants’ balance confidence was estimated using the CONFbal scale (Simpson et al., 2009). This scale is commonly used in rehabilitation and has an excellent consistency and reliability (Simpson et al., 2009). As with the quality-of-life measure, participants were asked standardised questions (for example, their confidence in standing from a chair unaided) and their responses recorded. The responses to the 10 standard questions were then summed to give an overall measure of balance confidence, with a lower score representing more confidence. A score of 10 would mean that the participant had answered ‘confident’ to each question.
When evaluating statistics for changes to quality of life of confidence balance, data were checked for normality using the Shapiro–Wilk test and non-parametric tests were conducted as a result (Wilcoxon signed rank test). Data are reported in terms of median and interquartile range and outliers are identified. Alpha was set to 0.05 for all tests, and all analyses were done in SPSS (version 26; IBM SPSS Statistics).
Qualitative surveys using open-ended questions were also completed during the study to further evaluate participant experiences. Participants were encouraged to leave detailed responses to questions such as ‘how does Pilates make you feel?’ as well as having the opportunity to add any other comments that they thought may be useful. The qualitative surveys were analysed using reflexive thematic analysis (Braun & Clarke, 2022) using an iterative process of immersion and data-familiarisation, coding and identifying themes. Data were analysed inductively so that the participants’ own experiences were foregrounded. The main researcher (CS) also maintained a reflexive diary throughout the process to document changes in positionality and viewpoints when considering the participants, and other researchers (RKL, FC, DG) acted as critical friends during the analysis process to develop and refine any themes that were identified (Smith & McGannon, 2017). The research is underpinned by a critical realist paradigm with a mixed positionality across all researchers, consisting of both ‘insiders’ and ‘outsiders’ which allowed us to explore the issues raised in the qualitative analysis from a range of diverse perspectives and using a pluralistic approach (Holmes, 2020). In particular, we felt that it was particularly important to critically reflect on our positionality throughout the intervention, as the majority of the research team does not have visual impairment so there are limits on understanding the participants’ perspectives. Our research team consisted of two experienced sighted guide runners, one person with physical impairment, and one person with visual impairment, so this allowed us to discuss relevant issues and perspectives relating to our participants’ views and lived experiences and to enhance our understanding of disability in physical activity and sport. In addition, two of the research team are mat-based Pilates instructors which allowed further discussion of possible accessibility issues and to avoid potential ableist assumptions in planning and delivering the sessions.
Results
Quality of life
The median score on WHOQUAL_BREF was 62.1 before the intervention and 59.3 afterwards. The differences in values are shown in Figure 1 below.
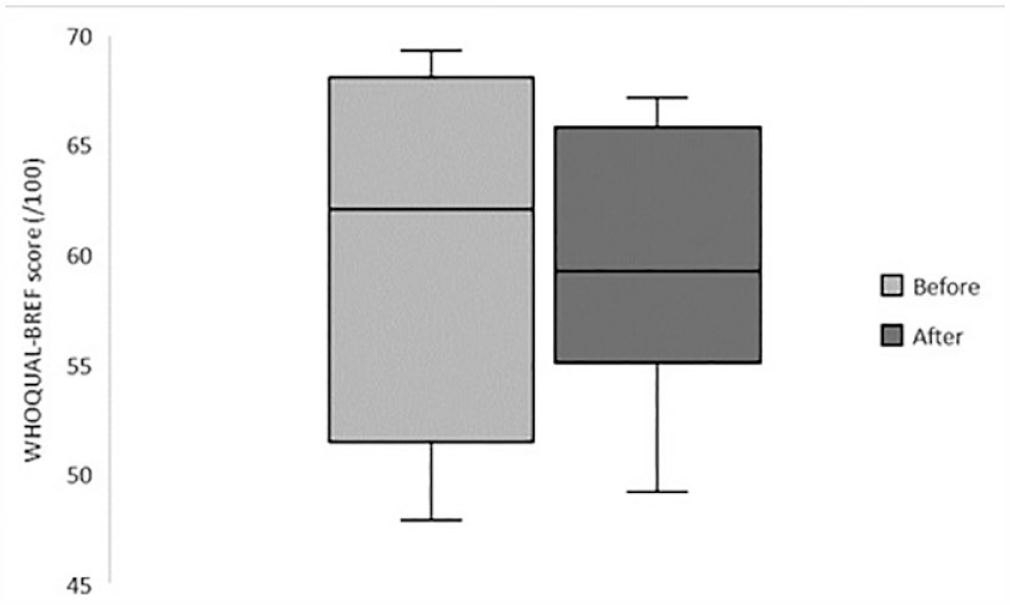
Quality of life data before and after the intervention.
The change in quality of life was not found to be statistically significant (p = .345).
The WHOQUAL_BREF measure is divided into four domains, and there were no obvious patterns observable in the physical health, psychology, or social domains, however all participants scored the environmental health domain as equal or lower after the intervention which was found to be statistically significant (p = .042, g = 0.449).
Balance confidence
The median balance confidence score before the intervention was 11, and 10.5 post-intervention, which was not found to be statistically significant (p = 1.0). Note that a lower value represents a higher confidence, so this suggests a small overall increase in confidence with everyday activities such as standing from a chair, walking on unstable surfaces, climbing stairs. The change in values can be shown in Figure 2 below, with a clear outlier after the intervention.
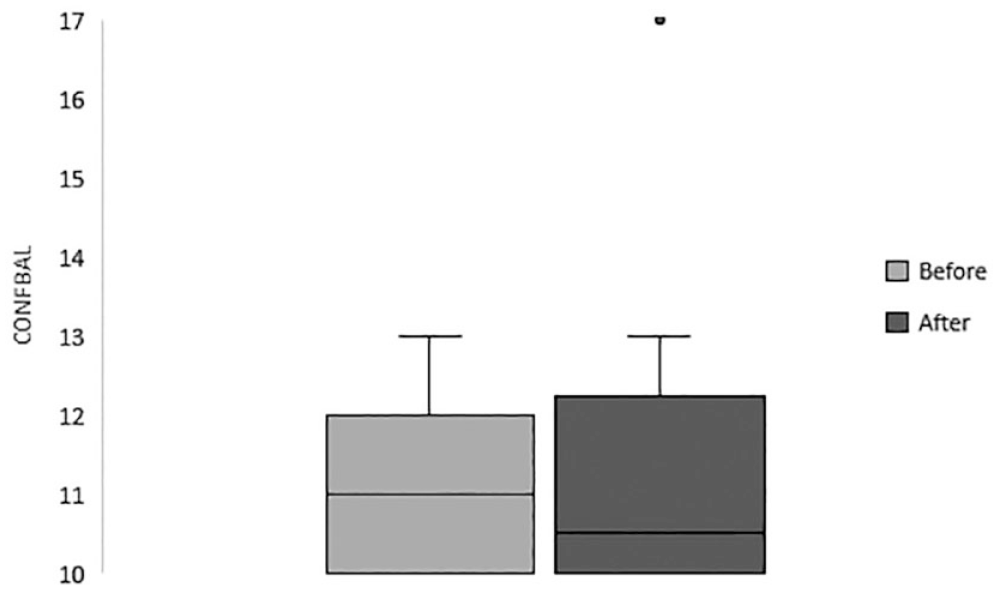
Balance confidence measured before and after the intervention.
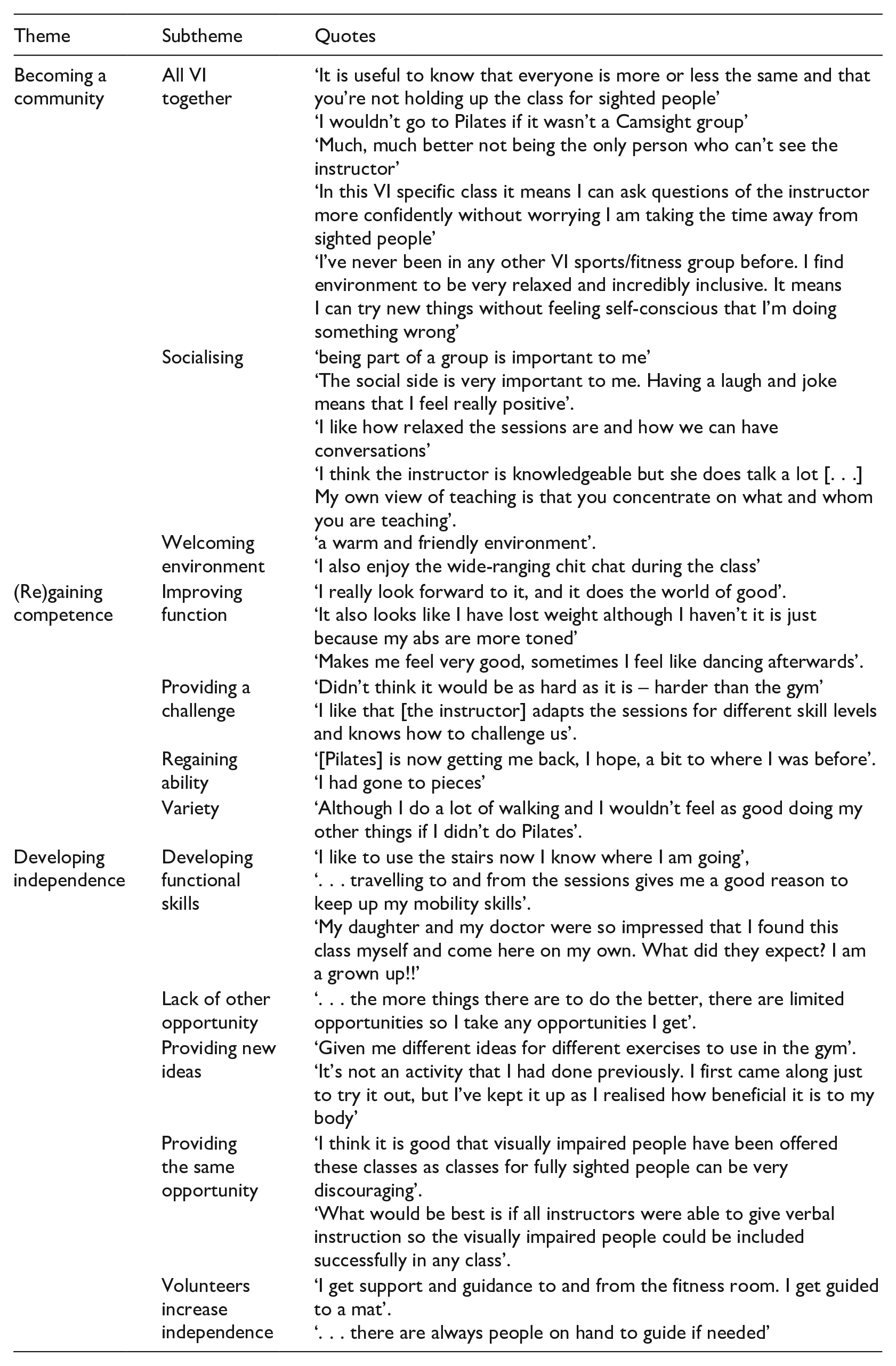
Qualitative data
When evaluating the quantitative data, we were interested in evaluating this modality as an effective method to engage people with visual impairments in physical activity by exploring the participants lived experiences of taking part in the sessions. There were three main themes identified in the reflexive thematic analysis: becoming a community, (re)gaining competence, and developing independence. These themes, and related subthemes with illustrative quotes, are shown in the table below.
Discussion
The qualitative data suggest that the Pilates intervention was perceived as positive overall with themes of becoming a community, (re)gaining competence, and developing independence determined inductively from the participants views and comments. The three themes identified in the analysis show clear links with Deci and Ryan’s (2000) self-determination theory which identifies key areas that allow the development of a self-motivated climate, increasing intrinsic motivation and supporting long-term behaviour change: relatedness, competence, and autonomy. This theory suggests that a self-determined environment is created by the coach, or the mat-based Pilates teacher in this case, and this was reflected in participant comments which suggested that the instructor was important. However, the role of the instructor changed over the intervention, as the participants that were new to mat-based group Pilates became more knowledgeable in the different exercises and adaptations available and could move into a more empowered position through an autonomy supportive environment (Duda & Appleton, 2016). As participants became more competent and autonomous, they were able to make requests for specific exercises that they had found effective and felt more confident in asking for clarification: ‘In this VI specific class it means I can ask questions of the instructor more confidently without worrying I am taking the time away from sighted people’. Feedback from participants helped to co-create the sessions with the instructor and the CamSight staff, and to develop best-practice when creating mat-based group Pilates interventions with this participant group, thus allowing a ‘domain-specific understanding of disability-specific experiences’ (Hall et al., 2023). This participatory process is ongoing (the class has continued since this research study has ended) and combines integrated knowledge exchange ensuring evidence-based practice and experiential knowledge and experience from the participants themselves (Smith et al., 2023).
There was a small improvement in balance confidence since the intervention, with reported confidence being 11 pre-intervention and 10.5 post-intervention. A CONFBAL score of 10 equates to all questions being answered as ‘Confident’ so this suggests that the participants already had a very high level of balance confidence prior to taking part in the class, and any score of 10 could not be improved by the intervention. The scores did not appear to be affected by severity or nature of visual impairment. In addition, changes in circumstance may have affected this score more than the intervention. For example, one participant started attending the classes with a guide dog, but once the guide dog retired subsequently had to learn how to navigate with a long cane and this may have affected her confidence in performing everyday activities that were unrelated to her participation in the classes. As such, it is important to recognise that many of the participants are already at a high level of competence and the emphasis of participating in this intervention may be to support them to regain any confidence they may have lost over the COVID lockdown and to provide variety and a chance to build relationships within their own community rather than to make a large contribution to their fitness and stability.
When planning and developing the sessions, participant independence was a key concern, and although support was available if needed, participants were expected to make their own way to the venue each week. Volunteers were available to help guide people to the room, or to their mat, but as the intervention went on participants reported that they felt more confident to navigate their own way through the city and the venue itself. The social model of disability suggests that barriers to access are socially constructed and not due to any diagnosed impairment (Berghs et al., 2019) and creating an inclusive and empowering space reduced these barriers to participation and created a welcoming space for further discussion in addition to increased physical activity. This allowed participants to share their experiences of visual impairment and some of the challenges they faced: ‘I like how relaxed the sessions are and how we can have conversations’, in particular, issues such as access to vaccines centres and COVID-19 tests, and participation in research were discussed during the sessions. Although this was a theme identified in many participants reflections, not all considered this to be positive: ‘I think the instructor is knowledgeable but she does talk a lot [. . .] My own view of teaching is that you concentrate on what and whom you are teaching’. In addition, this links to the idea of becoming a community, the participants adherence may have been affected by the cohesive group dynamics of having a group with a similar impairment (Spink & Carron, 1994) or by being advocated by a trusted local charity: ‘I wouldn’t go to Pilates if it wasn’t a Camsight group’. This sense of belonging to this community also means that participants can feel more confident that they all have similar issues: ‘Much much better not being the only person who can’t see the instructor’, ‘I’ve never been in any other VI sports/fitness group before. I find environment to be very relaxed and incredibly inclusive. It means I can try new things without feeling self-conscious that I’m doing something wrong’, which may reduce isolation and reduce mental health issues as people consider they are ‘better together’ (Stevens et al., 2021).
Despite previous research suggesting increased physical activity was correlated with increased quality of life measures in people without visual impairment (Soares et al., 2019), the scores for quality of life measured before and after the intervention showed a small non-significant decline in overall quality of life score. This study was conducted during a period of uncertainty and changing restrictions due to the COVID-19 pandemic, and factors relating to availability of health care, lack of other opportunities and changes in policy may also have affected this score. This is particularly evident in the lower score for the environmental domain in the WHOQUAL_BREF score, which includes aspects such as health and social care, opportunities for participation in recreational activity, and access to transport (The WHOQOL Group, 1998), all of which may have been affected since the relaxation of lockdown. Participant comments from the qualitative data also support increased quality of life in certain situations, for example, improved functional skills, increased opportunity, and increasing autonomy. However, access to health care in terms of ophthalmology appointments, retinopathy screening, and routine eye care has significantly changed as a result of the pandemic (Ahmed & Liu, 2021; Lakhani et al., 2021). In addition, delays to scheduled appointments and other health care has resulted in a backlog for routine National Health Service appointments and ongoing referrals (British Medical Association, 2022). While the mat-based group Pilates intervention may have started during a period of optimism that COVID-19 was waning, the return to a ‘new normal’ is not a straightforward process, and this study took place during a time of uncertainty, fear, and negative expectations (Codagnone et al., 2021). Thus, positive impacts from some aspects of the participants lives (e.g., physical activity participation) may be overshadowed by other negative experiences.
Despite a lack of statistically significant results in the quantitative analysis, the themes identified in the qualitative reflexive thematic analysis suggest that the intervention is having a positive impact on the participants and has provided an inclusive and welcoming environment for them to develop their independence and competence in Pilates. This is supported by the long-term adherence to the programme, with only one participant withdrawing from the classes over the whole 10-month period. Improved perception of function and improved sense of wellbeing are key in the participant comments, and this suggests that the intervention is valuable and popular within this participant group. Further projects by this research group will produce and evaluate best-practice guidelines for planning and developing co-created Pilates based interventions for people with visual impairment and reflect on the experiences of delivering and evaluating this intervention.
Strengths and limitations
The strength of this study relates to foregrounding the participant experiences, and using qualitative data to evaluate the effectiveness of the intervention in terms of the lived experiences of this participant group.
The COVID-19 situation limited the testing that was able to be done during this study, due to social distancing and no-touch correction being in place during the sessions, so further research evaluating other aspects that may result from mat-based group Pilates interventions, such as core stability, would be valuable within this population.
Conclusion
There was no statistically significant difference in overall quality of life or balance confidence resulting from this intervention, but most participants already reported high/medium levels for each measure. Participants have rated the environmental dimension of quality of life as lower post-intervention (p = .042) which may relate to slow recovery of health care and reopening of society post-COVID. Despite these results, qualitative analysis of the participants reflections identified themes relating to becoming a community, re(gaining) competence, and developing independence. The participants valued the sessions and considered them beneficial, both as a method of returning to increased activity following the relaxation of COVID-19 restrictions, and as an accessible physical activity option for people with visual impairment.