
Abstract
This study aimed to examine the effects of different light-curing modes on the immediate shear bond strength (SBS) of different composite resin types to dentin using universal adhesive. Human teeth were extracted and sectioned to obtain flat dentin slices. The universal adhesive was applied in total-etch mode. Conventional and bulkfill composites were used to create cylindric build-ups. Full power and Ramp mode were used to light-cure the adhesive and composite resin. SBS test was performed in a universal testing machine, and failure modes were determined via scanning electron microscopy (SEM). Two-way ANOVA and Student t-test were used to analyze statistical data. Significantly higher SBS was obtained when bulkfill composite was used compared to the conventional one (p < .001). The difference between Full power and Ramp curing mode was insignificant (p = .4). Mixed failure was the predominant type. Low SBS resulted in adhesive failure, while high SBS resulted in cohesive failure. Shear bond strength was not curing-dependent but rather material-dependent. Ramped curing does not contribute to higher bond strength. Bulkfill composite seems to be more favourable in terms of bond strength.
Introduction
Dental composites have become the most commonly used esthetic material for direct restorations. The durability of resin composite restorations is largely determined by the quality of the adhesive bond between the composite and cavity walls. Despite significant improvements in the development of new restorative materials and bonding agents, drawbacks associated with polymerization contraction and debonding along the composite/dentin interface, still remain a relevant clinical problem in modern dentistry. 1 If the stress resulting from polymerization contraction exceeds the bonding strength of the composite to the cavity walls, marginal junction failures may occur. However, if the bonding interface resists and remains intact, residual stress might be transferred to adjacent tooth structures, possibly resulting in enamel or dentin fractures. 2
Bonding efficiency is determined by various factors, including the light-curing properties and composite resin type. 3 Light of sufficient intensity and appropriate wavelength is necessary to initiate and develop optimal polymerization of deeper composite layers than just the superficial. Curing light is partially absorbed and dispersed on its way through the composite, resulting in reduced efficiency to ensure optimal polymerization. Consequently, this leads to an overall reduced depth of cure and conversion rate. 4 To overcome this problem and enhance the physical properties of composite fillings, manufacturers have developed curing sources with high intensity, which can be emitted in a matter of seconds. However, high irradiance levels may produce higher polymerization contraction and internal stress within the bonding interface. 5 It has been reported that most of the polymerization contraction is developed during the initial phase of the light-curing period. 6 On the other hand, low irradiance for a prolonged period might cause insufficient polymerization of the composite resin, with high levels of residual monomer. This residual monomer can reduce the mechanical properties of the final restoration and transition into the pulp via dentin tubules, causing genotoxic and cytotoxic effects. 7
The topic of modified light-curing is not new to dentistry. Over the years, different curing methods have been proposed to prevent significant development of polymerization contraction and promote higher bond strength.
8
However, a simple and efficient curing method that eliminates all drawbacks related to photopolymerization is still not determined. Modern LED curing units are equipped with multiple curing modes: standard, ramp, step, pulse, pulse-delayed, etc. These modalities can be continuous or intermittent, based on how the irradiance levels change over a predefined period of exposure time (Figure 1). The purpose of modified light-curing is to reduce stress build-up by providing additional time for stress relaxation before the gel-point is reached.
9
Prolonged material flow can compensate for polymerization stresses generated throughout the pre-gel phase. However, when the gel-point is reached, rigid contraction can generate stress at the bonding interface, which may weaken the bond and cause gap formation.
10
Different approaches in modulating the polymerization process 83 × 61 mm (300 × 300 DPI).
Ramp curing mode is a continuous, two-phase polymerization technique based on the use of initially low irradiance. During phase 1, low-light intensity is exponentially increased to its maximum. The goal of the exponential phase is to enable a broad spectrum of light intensity that could correspond to the materials’ unique composition and requirements for optimal polymerization. Phase 2 is a follow-up with a high-light intensity which ensures optimal mechanical properties necessary for the long-term stability of the composite restoration. Limited scientific data is available on the effects of ramped curing in direct relation to bond strength.11–13 Most of the previous research was focused on its effects in reducing contraction stress, in hope that this will ultimately lead to improved bond strength. However, such research resulted in rather conflicting findings.14,15 This is mainly due to the fact that the parameters of soft-start polymerization are still not strictly defined, so it is not surprising to find different recommendations regarding irradiance levels and exposure time. Furthermore, various curing units are available on the dental market, with different parameters, both for phases 1 and 2 of the ramp curing mode.
The current manufacturing practice is to further reduce the working time in the patient’s mouth by producing new composite materials and light sources which promote curing speed. The chemical structure of dental composites has evolved significantly over the last decade to overcome their most significant flaws. Improvements in the development process have led to a significant reduction of polymerization contraction, greater depth of cure, better material flow and adaptation, which overall, contributes to higher bond strength. 16 However, different composite types, placed with different techniques, may perform differently in bond strength.
This study aimed to compare the effects of different light-curing modes and composite resin types on the immediate SBS to dentin using universal adhesive. The following null hypotheses were tested: (1) light-curing will have no significant influence on the SBS and there would be no significant difference between the Full power and Ramp mode; (2) composite resin type will have no significant influence on the SBS and there would be no significant difference between the conventional and bulkfill composite. In addition, SEM was used to examine and record the failure sites.
Materials and methods
Research materials
Materials composition.
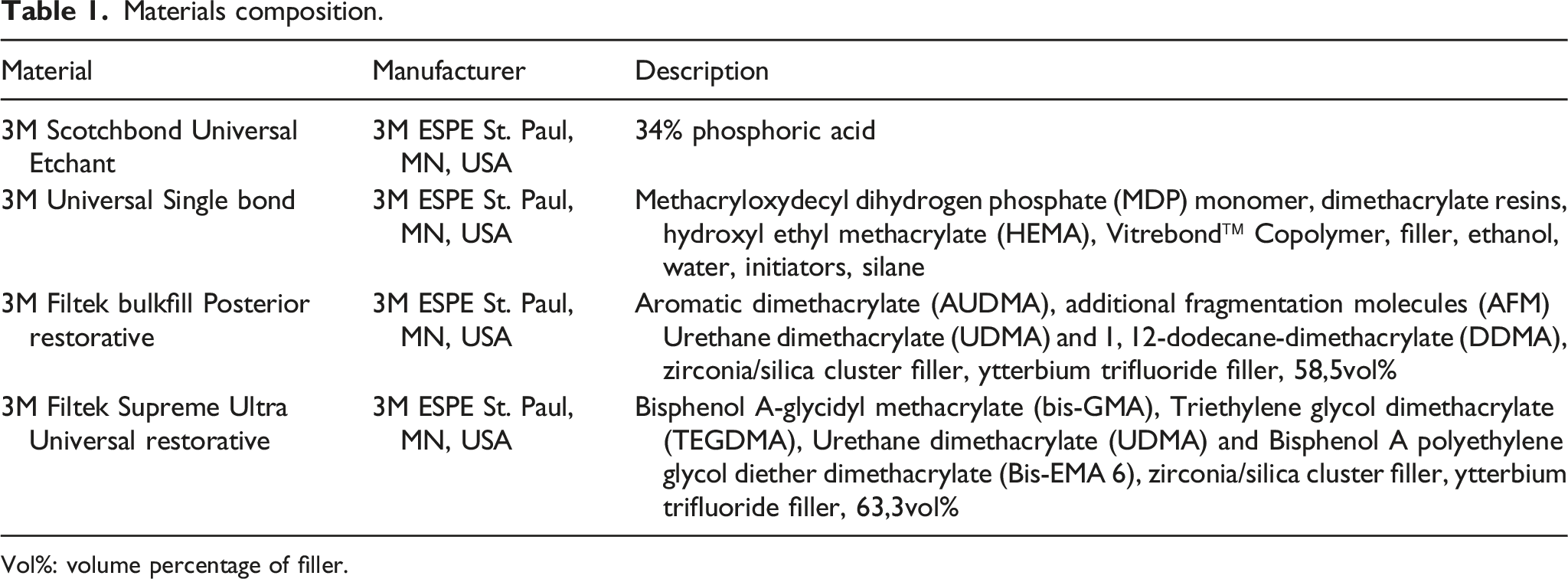
Vol%: volume percentage of filler.
Sample preparation
This study was conducted in accordance with the ethical principles of the Helsinki declaration and was approved by the Ethics Committee of the Faculty of Medicine in Niš (reference number 12-3340-2/5). Informed consent was obtained from each subject prior to their participation in the study. Sample preparation and SBS testing were performed according to ISO 29,022. Sixty human teeth were extracted and collected for the purpose of this experiment. Upon extraction, the teeth were rinsed and cleaned before being stored in saline solution at room temperature to mimic the humid environment in the oral cavity. The crowns were cut in a mesio-distal direction, parallel to their longitudinal axis, without revealing the pulp, using a low-speed diamond disc under the air-water spray. Ultrasonic bath cleaner (USC200 T, VWR International, Radnor, Pennsylvania, USA) was used for smear layer removal from the obtained dentin plates at 25 C for 45 min. The prepared plates were then air-dried and embedded into plastic cylinders with flat dentin surface upright to the cylinder’s long axis and fixed with super-hard stone class IV (Elite Stone, Zhermack, Germany). The exposed dentin surface was processed with Sof-Lex finishing and polishing discs (3M ESPE, St. Paul, MN, USA).
Bonding procedure
Sample grouping and curing mode parameters.

The etching and bonding procedure was done according to the manufacturer’s instruction manual. Etchant 34% was applied to the exposed dentin surface for 15 s, then carefully rinsed for 10 s and air-dried for 5 s. Immediately after, universal adhesive was applied for 5 s by brush and air thinned for 5 s to evaporate the solvent. The adhesive was cured for 10 s using Woodpecker Led-C curing unit (Guilin, Guangxi, China) in full power or ramp mode, accordingly. Woodpecker LM-1 radiometer (Guilin, Guangxi, China) was used to measure the starting/ending curing power. Conventional and bulkfill composite was used to create composite build-ups of 4 mm in diameter and height, using a plastic mould. Bulkfill composite was applied in a single layer and light-cured in either Full power or Ramp mode. The conventional composite was packed in increments of 2 mm thickness and each increment was light-cured for 20 s in Full power or Ramp mode, accordingly. The curing tip was positioned above the sample surface at a minimal distance (Figure 2). Bonding procedure (a), SBS testing (b) and SEM analysis (c) 211 × 101 mm (300 × 300 DPI).
Shear bond strength testing
Immediate SBS was measured using a universal testing machine (Wagezelle Load Cell, Hottinger Baldwin Messtechnik, Germany) at a crosshead speed of 1 mm/min. Before testing, the samples were secured in a metal bracket with boding interface aligned to the loading force axis. Bond strength was calculated in MPa as follows:
Stress = Failure force (N)/bonding area (mm2)
Scanning electron microscopy
Failure modes were determined via SEM (JSM 6610; JEOL, Tokyo, Japan) and classified as: adhesive, cohesive in composite, cohesive in dentin, or mixed failure (consisting of multiple failure modes). The fractured samples were placed in aluminium carriers (Dotite point xc 12 carbon JEOL, Tokyo, Japan) and coated with a thin golden layer, in low vacuum conditions (JFC 1100E Jon Sputter JEOL, Tokyo, Japan), to be eligible for observation under different magnification.
Statistical analysis
Quantitative research data was analyzed using SPSS 21.0 (SPSS Inc, Chicago, IL, USA). Two-way ANOVA and Student t-test with a significance level set at p < .05 were used to compare the obtained SBS measurements.
Results
Descriptive statistics of shear bond strength (in MPa) for each group.

F: Full power mode; R: Ramp mode; C: Conventional composite; B: Bulkfill composite.
Two-way ANOVA.

*Statistical significance at the level of 5%. df-degrees of freedom.
Statistical comparison of shear bond strength between the conventional and bulkfill composite.

*Statistical significance at the level of 5%.
Statistical comparison of shear bond strength between the Full power and Ramp curing mode.

Descriptive statistics of shear bond strength for each failure mode.

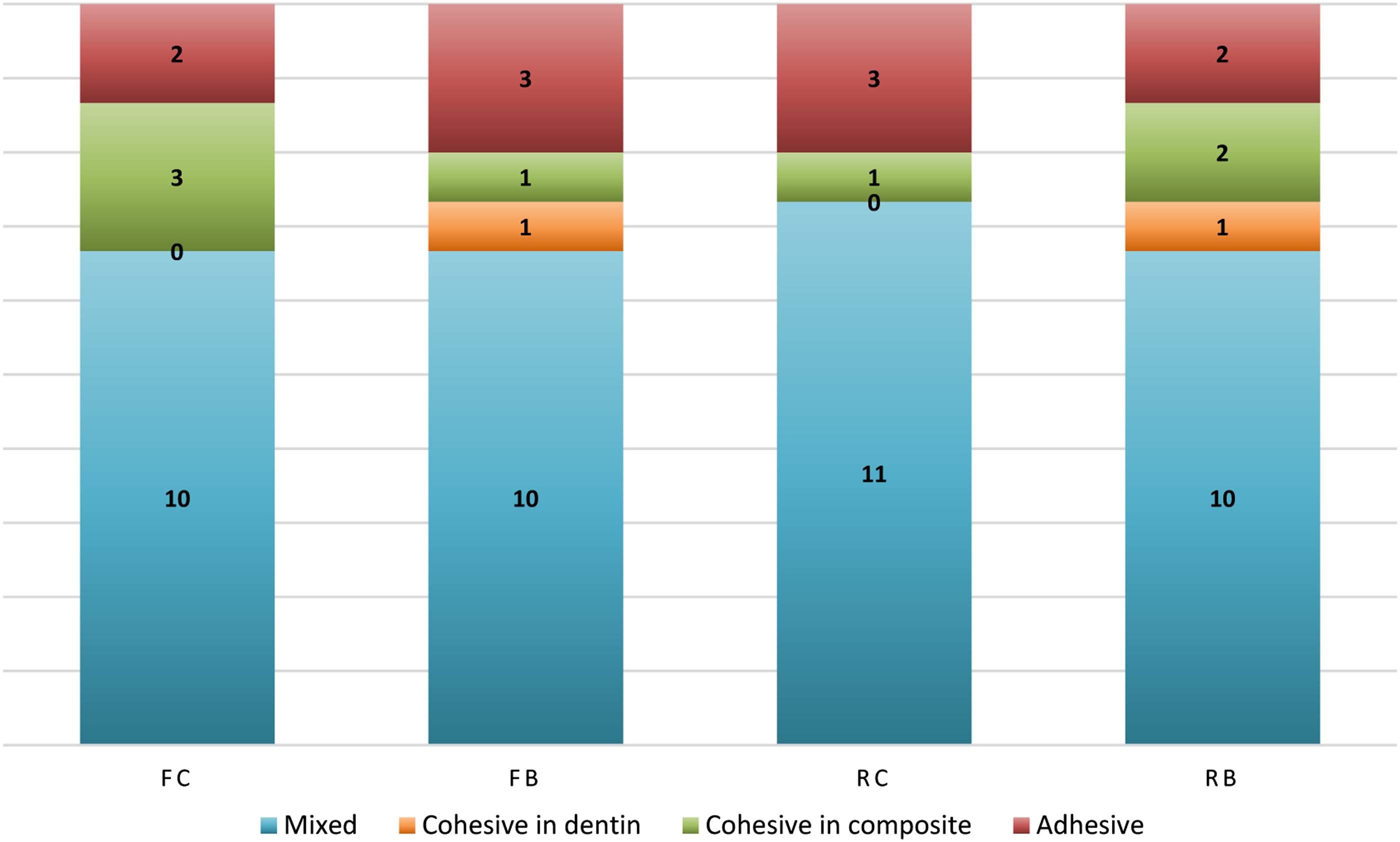
Failure mode distribution for each tested group: FC (full power/conventional composite), FB (full power/bulkfill composite), RC (ramp mode/conventional composite) and RB (ramp mode/bulkfill composite).
SEM images of different failure modes are presented in Figure 4. The adhesive failure site was generally coated with universal adhesive, while the mixed failure site consisted of additional dentin and/or composite areas. Cohesive failure sites were covered only by dentin or resin composite. Cross-section of the composite/dentin interface is shown in Figure 5. Similar morphological appearance of the adhesive and hybrid layer was observed in all sample groups, regardless of the light-curing mode and composite resin type used. SEM images of each failure mode: (a) adhesive; (b) mixed; (c) cohesive in dentin; (d) cohesive in composite 110 × 88 mm (300 × 300 DPI) SEM image of the adhesive interface: A-adhesive layer, H-hybrid layer, D-dentin, C-composite 153 × 121 mm (300 × 300 DPI).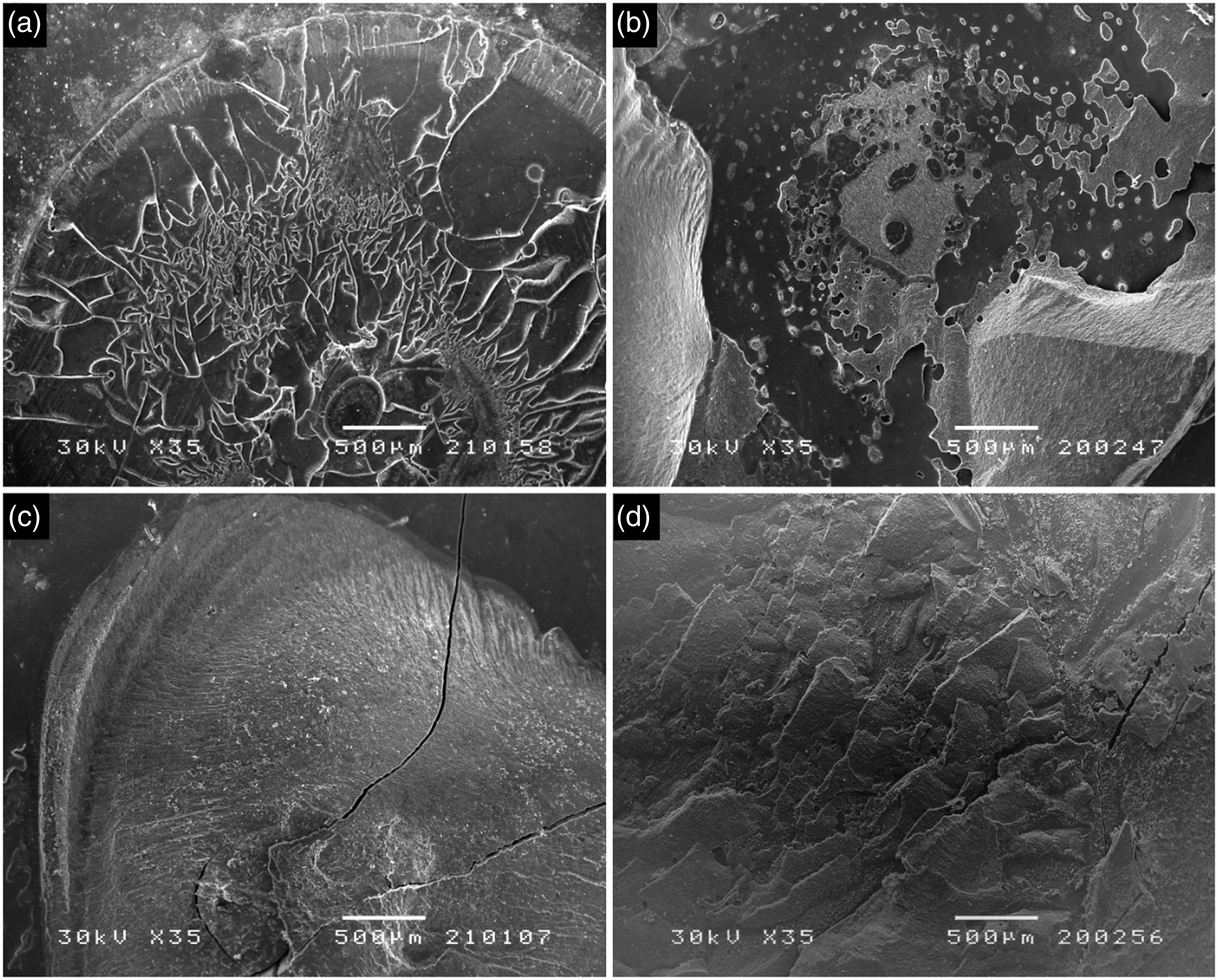

Discussion
Establishing an optimal adhesive bond between two completely different substrates, such as dentin and composite, is extremely complex and dependent on many different factors. Different clinical and laboratory methods are used to assess the efficiency of this adhesive bond. Although clinical studies provide more relevant data, laboratory studies such as SBS testing are conducted more often due to their simplicity and time-saving. 17
Based on the obtained results, the first null hypothesis of this study was accepted. Statistical analysis revealed that “curing mode” is not an influential factor in the variability of SBS and is material-independent. The difference in SBS between the full power and ramp curing mode was insignificant, regardless of the applied composite resin type. The absence of favourable effects of the ramp mode, in this case, could be explained by the fact that the initial phase of low irradiance does not last long enough and is quickly annulled by the final phase of high irradiance, which lasts much longer. Our findings of ramped curing being less effective than standard curing correspond to those of previous in vitro studies which came to the same conclusion using different curing parameters11,12 and different testing methods.18–20 Few studies have experimented with the effects of ramped curing to bond strength in clinical conditions. Dijken et al. 21 reported that, after an observation period of 7 years, composite restorations cured in “soft-start” mode resulted in higher failure rates than those cured in “standard” mode. Moreover, another clinical study reported no significant difference between ramped and constant curing modes in terms of postoperative sensitivity of Class V composite restorations. 22
On the other hand, Fahmy et al. 13 found ramped curing to be effective in improving the bond strength between resin-based cement and dentin, using a wide range of exponentially increasing light intensity (0–1200 mW/cm2). Ernst et al. 23 and Sudheer et al. 24 also reported a significant reduction in contraction stress and marginal microleakage using the ramp curing method. However, these favourable results are based on curing parameters which include prolonged exposure time that compensates for the reduced degree of conversion caused by extremely low initial irradiance used in these studies. This is in contrast to the requirements of modern dentistry for increased curing speed and shorter work time and makes ramped curing impractical for everyday clinical use. In the present study, we focused on a more balanced approach between the irradiance levels (500–1000 mW/cm2) that will have no adverse effect on the degree of conversion and shortened exposure time (20 s) that corresponds to the principles of modern dentistry. However, ramp mode in its chosen parameter setup did not contribute to higher bond strength as expected. Having in mind that the parameters of soft-start polymerization are still not fully standardized, further research is needed to determine the minimal irradiance and maximal duration of the initial curing phase without compromising the conversion and mechanical properties of the composite restoration.
The discrepancy in results of previous studies does not come as a surprise, keeping in mind that different curing parameters are used in each of them to find the best possible curing method. Also, this makes study comparison extremely difficult. Modified curing methods are still continuously examined and reassessed by the scientific community. Some believe that modified light-curing has significant benefits to polymerization contraction and marginal adaptation, while others think this kind of effects are very limited and followed by many disadvantages. The main objection to modified curing methods is that the reduction in shrinkage cannot be achieved without lowering the degree of conversion. 25 It has been previously reported that low irradiance levels slow the polymerization reaction but also generate less chain growth centres and create more linearly structured polymers sensitive to degradation. 26 Moreover, low irradiance produces polymers with lower elastic modulus and a higher level of structural inhomogeneity. 27 Soft-start protocols have also been previously associated with reduced cross-link density of the composite polymer network. 28 Because of these downsides, modified curing methods were never entirely accepted by clinical practice.
The second null hypothesis of this study was rejected. Statistical analysis revealed that “composite type” is a highly influential factor in the variability of SBS and is curing-independent. The difference in SBS between the conventional and bulkfill composite was significant, regardless of the applied light-curing mode. Better performance of bulkfill composite could be attributed to significant improvements in structural and chemical composition. The inorganic part of both composites used in this study is almost identical and consists of 20 nm silica and 4–11 nm zirconia particles, with slightly higher volume in the conventional (63.3%) compared to bulkfill composite (58.5%). Previous reports suggest that bond strength may be influenced by composite microstructure in a way that higher resistance to shearing is observed in composites with higher filler volume, 29 which is contrary to our results. Thus, higher SBS of bulkfill composite, in this case, is more likely related to modifications in the organic portion of the material. The addition of novel monomers AUDMA (aromatic urethane dimethacrylate) and AFM (addition fragmentation monomer) that, in combination, act to lower polymerization stress upon light-curing indirectly reflects on the bond strength as well. The presence of these monomers enables the polymer network to rearrange and adapt throughout the polymerization process to compensate for the developing shrinkage. 30 Higher SBS of bulkfill composite may also be attributed to improved light transmission and greater polymerization depth compared to the conventional composite. Optimization of filler/resin refractive index mismatch 31 and addition of more efficient (germanium-based) photoactivators, like Ivocerin, 32 enabled bulkfill composites to be placed in a single bulk increment and properly cured up to a maximum depth of 4–5 mm.
Bulkfill composites have gained much popularity among clinicians because they prefer simple approaches that save time and minimize the possibility of error. 33 On the other hand, the application of conventional composite in deep cavities is still limited to multiple increments of 2 mm thickness. Although the incremental filling technique is considered beneficial for stress reduction and marginal adaptation, our results suggest otherwise in terms of bond strength since higher SBS was obtained when bulkfill composite was placed in a single increment. Recent studies also suggest that composite placement in oblique increments may cause even higher shrinkage and stress compared to single increment fill. 34 Moreover, increasing the number of increments in deep cavities leads to a higher probability of incorporating voids and porosity, which may compromise the bond strength. 35
An important limitation of this in vitro study is that only immediate SBS was measured, and no artificial ageing was performed to mimic the in vivo environment. When performing bond strength experiments, the use of degradation techniques such as thermocycling and fatigue stress is recommended whenever possible because it has been previously reported that some adhesives with high immediate SBS may show a decrease in bond strength after ageing. 36
Failure mode analysis in the present study demonstrated similar failure patterns in relation to light-curing mode and composite resin type, with the predominance of mixed failure in all sample groups. Ultrasonic removal of the smear layer and additional dentin etching with phosphoric acid enabled better adhesive adaptation and resin tag penetration. The hybrid layer was thick and uniform along the entire surface of the restoration, with numerous resin tags protruding into the lumen of dentin tubules. Furthermore, the use of alternative surface treatments that result in chemical dissolution (polyacrylic acid) 37 or mechanical removal (airborne-particle abrasion, Er:YAG laser)38,39 of the smear layer is recommended to obtain higher bond strength and improve the adhesive to cohesive failure relation r.
Conclusion
Based on the obtained measurements and failure mode analysis, within the existing limits of this study, it has been determined that differences in material composition are a more important factor in determining the SBS than the differences in curing parameters. Bulkfill composites are more beneficial to bond strength than conventional ones. Although ramp mode did not contribute to higher SBS in this case, we believe that the solution to the ideal curing pattern lies in the balanced relationship between the wavelength, irradiance and exposure time. The introduction of polywave LED curing units provides great research possibilities for future studies attempting to design an effective curing pattern that will correspond to the material’s unique composition and requirements for optimal polymerization.
Footnotes
Acknowledgements
The authors thank Miroslav Miljkovic for providing technical support in Scanning Electron Microscopy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Education, Science and Technological Development of the Republic of Serbia (Grant No: 451-03-9/2021-14/200113).