
Abstract
This article examines the motivations of doctors operating in restrictive abortion regimes, and it takes Poland as a case study. It places in the foreground institutional and intra-professional factors that determine abortion healthcare, which to date have been accorded little attention. The article compares the impact that criminal, professional, and social sanctions have upon the provision of abortion services. In so doing, its purpose is to refocus debate in this area. It aims to move the emphasis away from legal and political factors, including the criminalisation of abortion, and to place it on medical agency. The Polish case study is examined to test out, in the context of a late-transitional polity, the sustainability of neo-institutionalist approaches to the study of law and organisations and the sociology of professions. The analysis is particularly important and urgent in light of the recent retrenchment of reproductive rights in Poland, and beyond.
Keywords
Introduction
Writing over 20 years ago about the history of abortion law in the USA, Reagan (1997: 3) noted that ‘[i]t would have been virtually impossible for the state to enforce the criminal abortion laws without the cooperation of physicians’. The studies of abortion in different regional and socio-political contexts have confirmed that (a) historically, official medical bodies provided strong support for the criminalisation of abortion (Keown, 1988; Luker, 1984; Mohr, 1978; Sheldon, 1997; Solinger, 1998); (b) many physicians are, at least officially, inclined to interpret abortion laws narrowly, limiting or denying access to abortion services (Bentancur Pérez and Rocha-Carpiuc, 2020; Bergallo, 2014; De Zordo and Mishtal, 2011); and (c) the medical profession is generally reticent to support liberal abortion reforms (Freedman, 2010; Joffe, 1995; Joffe et al., 1998). Yet, far less is known about the reasons and mechanisms that shape the collective and individual behaviour of the medical profession and its members 1 in relation to abortion in states with restrictive abortion regimes. Much social science literature to date has emphasised the impact of conservative legal and political actors, at both national and international levels, on abortion practices (Enright and De Londras, 2018; Petchesky, 1984; Solinger, 1998; Yamin et al., 2017). Criminalisation and the so called ‘chilling effect’ of the law are often seen as primary factors constraining access to lawful abortion services (Nowicka, 2011). Researchers have attempted to account for physicians’ behaviour on historical and cultural grounds, including deeply rooted patriarchal structures, pervading paternalism and the importance of religious organisations in society (De Zordo, 2018; Hoff, 1994; Jankowska, 1991). However, these studies often omit important aspects of abortion law and healthcare.
This article gives prominence to institutional factors determining the collective and individual behaviour of medical professionals, which to date have been accorded little attention (Freedman, 2010; Halfmann, 2011; Joffe, 1995). It combines insights from the sociology of professions and (neo-)institutional theory to argue that questions concerning the behaviour of the medical profession regarding abortion cannot be comprehensively addressed without the analysis of professional organisations and employment structures. Such studies have generated important insights by analysing the impact of law, organisational practices and processes of professionalisation on the development of institutions (Chiarello, 2019; DiMaggio and Powell, 1983; Edelman et al., 2010). 2 This article extends this research by examining the legal, professional, and employment frameworks shaping the relationships and power dynamics within the medical profession, addressing, in turn, how these affect the development and operation of abortion law. In particular, it considers the factors determining physicians’ professional autonomy in relation to abortion, that is, their regulatory independence from the state and their decision-making power in every-day medical practice (Freidson, 1993). On this basis, the article assesses the role that criminal law, professional regulation and institutional and organisational relationships play in restricting professional autonomy, and it investigates how these restrictions impact upon the provision of abortion services. As such, the study adds an important layer of analysis to scholarship concerning attitudes and behaviour of healthcare professionals in relation to abortion. Existing studies have shown how emotionally driven attitudes, in particular the fear of negative legal, professional and personal consequences, influence the actions of healthcare practitioners relating to abortion (Duffy et al., 2018; STER, 2018). The article argues that, although fear of criminal sanctions may be an important factor shaping behaviour, the rhetoric of fear is often utilised as a tool enabling physicians to pursue the restrictive interpretations of abortion law and remove responsibility for their actions. In this respect, the article acknowledges the influence of churches and religious organisations on abortion practice, noted by other scholars (David and Titkow, 1994; Fuszara, 1991; Graff 2008; Mishtal, 2015). However, in an attempt to redirect current debates, it focuses on the ways in which such influences are facilitated through (intra-)professional relationships.
The article takes as a case study the provision of abortion services in Poland. Poland has distinct importance in this context for several reasons. First, Poland is a primary example of a state with restrictive abortion regime. Its medical profession placed an active role in the introduction of restrictive abortion legislation in 1993 (Łętowska, 2012), and numerous violations of the reproductive rights of women in Poland have been criticised by the European Court of Human Rights (ECtHR) (Tysiąc v Poland, R.R. v Poland, P.S. v Poland). Second, although Poland is currently a regional outlier in terms of abortion practices, the behaviour of the medical profession bears some similarities with countries, like Ireland, which have recently liberalised their laws, but where barriers to abortion services still exist. The study of abortion in Poland offers the opportunity to examine ‘the importance of professions and professionals as agents in the creation, maintenance and disruption of institutions’ (Muzio et al., 2013: 704). Third, Poland's particular explanatory significance lies in the unusual non-linear development of reproductive rights. Under the Socialist system abortion was legal and widely available. However, the political and socio-economic transition, formally initiated in 1989, gave rise to one of the most restrictive abortion regimes in Europe. These experiences can be instructive for the discussion of other post-Socialist states, such as Croatia, Hungary or Lithuania. These countries have retained liberal abortion laws, but they are witnessing a surge in anti-abortion movements calling for restrictive legal reforms.
In more general terms, the analysis of a healthcare system in which there exist different strata of professional and institutional organisations, marked by the strong remnants of a previous socio-political regime, provides an opportunity to build up a more complex understanding of professional and institutional structures affected by past legacies. It offers the opportunity critically to test in the context of a late-transitional polity the value of neo-institutionalist approaches to the study of law and organisations (Edelman and Suchman, 1997; Edelman et al., 1992; Heimer, 1999). The study of institutions and their impact on abortion law in Poland is also instructive for broader inquiry into countries with a populist government, traditional society and institutionalised religion in other geographical contexts (e.g. Nicaragua), which have witnessed retrenchment with regard to reproductive rights.
The analysis presented in this article is particularly urgent in light of the recent legal developments in Poland, where the Polish Constitutional Tribunal issued a judgment (K 1/20), which resulted in the re-criminalisation of abortions performed on grounds of diagnosed risks of severe disorders or incurable illness of the foetus. In July 2021, the ECtHR began proceedings concerning 12 Polish applicants alleging that the judgment breaches their human rights (ECtHR, 2021). The judgment is also seen to limit professional autonomy of physicians to such an extent that, for the first time in decades, the medical profession found itself openly in opposition to the government. Unprecedentedly, not only individual doctors, but also medical organisations have raised concerns over the recent developments in abortion law (PCPD, 2020; PSHG, 2020). Understanding the factors determining professional behaviour acquires particular importance as a part of strategy for building alliances for future mobilisation in favour of liberal reforms.
Methods
The article is the result of a 12-month study of the autonomy of the medical profession in Poland. 3 The study utilised a mixed-method approach (Denscombe, 2007; Newman and Benz, 1998; Tashakorri and Teddlie, 2010). First, within the theoretical framework provided by neo-institutionalist approaches to law and organisations and the sociology of professions (discussed below), the project used doctrinal analysis of relevant primary and secondary legislation, case law of the Constitutional Tribunal, professional regulations and related policy documents. This material was analysed to determine the scope of the criminal and professional liability of medical professionals with regard to abortion services and the legal status of employment relations among physicians in hospitals. The theoretical and doctrinal analysis of legal and policy documents constitutes the main body of the article.
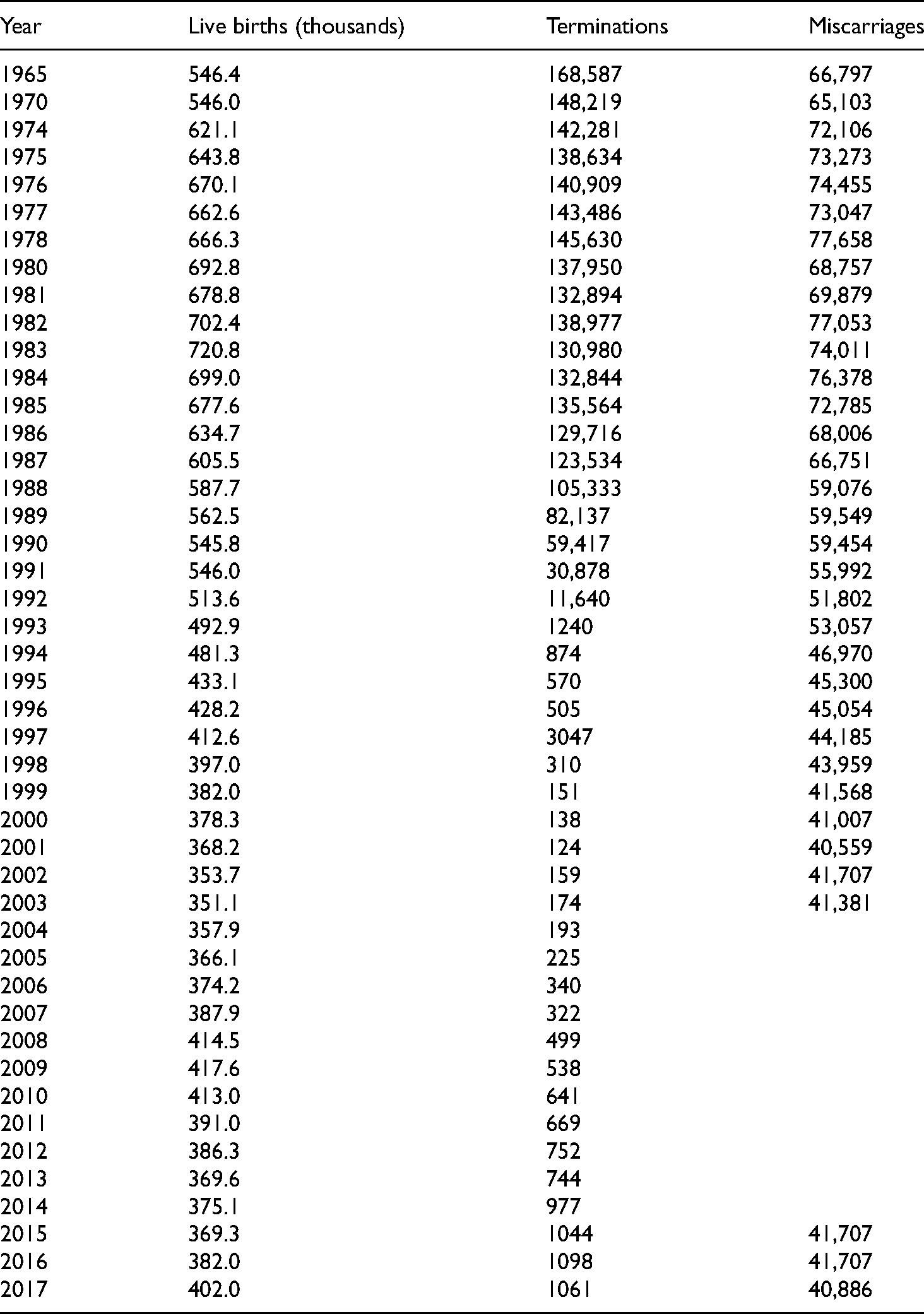
Second, the study analysed available quantitative data concerning the criminal and professional liability of medical professionals to establish whether the criminalisation of abortion in Poland fully explains restrictive medical practices. Three main types of data were analysed in this context. The first type of data concerned the number of abortions officially performed between 1965 and 2017. Such data were retrieved from Government Reports (1996–2017) on the implementation of the Act on Family Planning, the Protection of the Human Foetus and Conditions Permitting Pregnancy Termination 1993 (thereafter the Act 1993) and are presented in Table 1. These data were supplemented by data published by the Federation for Women and Family Planning (FWFP, 2020). The second type of data concerned the number of cases of illegal abortions, which were officially noted by the prosecution service between 1993 and 2017. These data were also collected from the aforementioned Government Reports (1993–2019). The quality of such data is mixed. It has been impossible precisely to ascertain the impact of the criminalisation of abortion on physicians as a special separate category of potential offenders. Nonetheless, the analysis made it possible to draw conclusions about the fluctuations and/or consistency in levels of reporting of unlawful abortions in comparison to the levels of prosecutions brought against individual persons (regardless of whether they were doctors or not). The visual representation of this comparison has been provided in Figure 2.
The number of abortions registered in Poland between 1965 and 2017.
The third type of data concerned the number of professional liability proceedings initiated during the period 1993–2018 against physicians in connection to abortion, that is, concerning a breach of the relevant provisions of the Code of Medical Ethics 2004 (and 1991), which outlined the professional standards and conditions for abortion. This information was collected through Freedom of Information (FOI) requests sent in October–November 2018 to all the Regional Chambers of Physicians, including 17 Regional Reviewers of Professional Liability and 17 Regional Medical Courts, as well as to the Supreme Reviewer of Professional Liability 4 and the Supreme Medical Court, 5 organs of the Polish Chamber of Physicians. Out of the 17 Regional Medical Courts and Reviewers of Professional Liability existing in Poland, 14 Courts 6 and nine Reviewers 7 replied. One of the 14 Regional Chambers that replied refused to provide data on the basis of insufficient public interest. 8 Two provided data since 2008 and one provided data since 2006, as earlier data had been archived and their retrieval would have required a disproportionate deployment of resources. In addition, the Supreme Reviewer and the Supreme Medical Court replied to the FOI requests, but provided data only from 2010 onwards. These gaps could be partially filled by data concerning professional liability collected by the Government since 2002, although due to the vagueness of the categories applied in these reports, their utility in assessing the exact number of proceedings is limited. Despite their obvious limitations, the data make it possible to build a comprehensive picture of the engagement of professional self-regulation bodies in the implementation of legal and professional standards concerning abortion.
Third, the study used secondary qualitative data extracted from a Report published by the Foundation for Equality and Emancipation ‘STER’ – entitled ‘Allies or Opponents’ (STER, 2018). The Report concerned the role of the medical profession in abortion debates in Poland. The Report was based on the analysis of semi-structured interviews with 85 Polish gynaecologists working in Poland and/or abroad. It revealed the attitudes of Polish medical professionals towards abortion law. As such, it constituted the starting point for this article, which juxtaposed the findings of the STER Report with the analysis of quantitative data and doctrinal and policy analysis. Overall, the findings of the mixed-method analysis conducted here challenge some explanations that focus on political and extra-professional factors shaping the particularly restrictive and conservative behaviour of Polish physicians with regard to abortion.
Theoretical Framework
Sociology of Professions and Sociological Studies of Abortion
Owing to the effects of medical institutions and professional structures on such agency, the analysis of the factors shaping individual and collective agency of medical professionals in relation to abortion requires a multi-layered theoretical framework. The framework used to capture this in this article is based on three distinct, yet interrelated bodies of literature, that is, socio-legal studies of abortion, the sociology of professions and recent (neo-)institutionalist studies.
Studies focusing on the role of the medical profession in the development of abortion law have so far been dominated by Anglo-American scholars. Such scholars have utilised concepts of social closure, jurisdictional competition and professional autonomy in medicine, developed by sociologists of professions like Freidson (1970), Johnson (1972), Larson (1977), and Abbott (1988). They used these approaches to demonstrate how the members of the medical profession have exploited abortion (law) to further their interests in an unequal struggle for regulatory autonomy, economic power and social authority (Keown, 1988; McGuinness and Thomson, 2015; Reagan, 1997; Sheldon, 1997; Thomson, 2013). Of particular importance for such analysis and for the present study is the concept of medical autonomy, developed by Freidson. Freidson interpreted professionalisation as a process marked by the gradual expansion of corporate and clinical autonomy. He defined corporate autonomy as the regulatory independence of professionals from the state, and he defined clinical autonomy as decision-making power in every-day medical practice (1993: 73). He argued that, despite diverging degrees of corporate autonomy in different political systems, the medical profession always retains substantial freedom in determining its every-day practices, regardless of its relationship to the state and state regulation (1993: 59). Understood in this way, clinical autonomy is a central indicator of, and a factor that underlies, individual and collective agency of medical professionals in relation to abortion. For instance, McGuinness and Thompson (2015: 190) noted that medical organisations in the UK refused to support liberal reforms to abortion law because this refusal expressed resistance both to patients’ demands, and to encroachment by the legislature on clinical discretion (…) and scientists’ epistemic authority. Analogously, Reagan claimed that medical professionals in the USA mobilised around liberal reforms only when the abortion regulation restricted physicians’ decision-making power in everyday medical practice to such an extent as to undermine their medical autonomy (Reagan, 1997: 234).
It is sometimes claimed that the concept of clinical and regulatory autonomy has limited value for describing the professional structures in societies under Socialist governments. For instance, Freidson's findings have been called into question in the context of Socialist states. This is due to his (alleged) insufficient regard for the limits that authoritarian political systems and patterns of economic management imposed on the clinical autonomy of the medical profession (Hoffman, 1997: 347–348). This article partially challenges this view. On the one hand, it recognises that the absence of independent professional organisations and the lack of basic resources under Socialist polities imposed serious constraints on the collective behaviour of medical professionals. On the other hand, however, it argues that, in such contexts, intra-professional hierarchies – partially developed under Socialism and subsequently reinforced by privatisation during the first years of post-Socialist transformation – retained importance in shaping clinical autonomy. Consequently, professional autonomy remains an important point of reference in discussions about abortion law, especially in the context of late-transitional (post-Socialist) societies, a context which remains under-studied.
Neo-institutionalist Approaches
Neo-institutionalist approaches have particular importance in showing how organisational and institutional structures determine professional behaviour, and they contribute in vital ways to our understanding of patterns of legal formation.
Such methods complement the neo-Weberian paradigm in that they frame professions as institutional agents with distinct motivations and survival strategies (Brock and Saks, 2016: 3). Early neo-institutionalists helped elucidate the grounds upon which institutions, including healthcare providers, operating in different contexts, make similar decisions. For instance, Di Maggio and Powell showed that institutions are marked by the orientation towards increasing homogeneity in organisational forms and practices, that is, ‘institutional isomorphism’. In turn, they explained how this orientation could result from (a) the coercive force of law and political influence, (b) inter-organisational practice borrowing or (c) the processes of professionalisation including formal education and professional networks (DiMaggio and Powell, 1983). Furthermore, neo-institutionalist approaches help us to understand the mechanisms that condition legal implementation, compliance and resistance. Early neo-institutional theory perceived law as a predominantly explicit, stable and coercive force (DiMaggio and Powell, 1983). By contrast, later studies have pointed out that organisations can construct and transform the meaning of law and compliance and reconfigure legal regimes even as they respond to them (Edelman and Suchman, 1997: 484; Suchman and Edelman, 1996: 905). The structures developed in institutional settings may have a chilling effect on the implementation of law, or they may influence the way in which law is understood, in turn, in ways that inhibiting its mobilisation of law (Edelman et al., 2010: 666).
Importantly, as observed by Edelman and Suchman, law and organisations studies have shown on numerous occasions that professionals can exaggerate or reify legal threats ‘in ways that may have little to do with reality’ (Edelman and Suchman, 1997: 500). Certain forms of compliance become institutionalised through the reproduction of normative constructions promoted by professionals within organisations (Chiarello, 2013). Subsequently, these constructions ‘attain a mythical and taken-for-granted form of rationality and spread quickly among organisational populations’ (Edelman et al., 2010: 656). It follows from this that coercive legal effects may arise after professional and organisational communities have socially constructed a definition of compliant behaviour (Edelman and Suchman, 1997: 498; Suchman and Edelman, 1996). Consequently, in the context of healthcare provision, neo-institutionalist scholars have argued that the discretion of healthcare providers is limited not only by actual legal obstructions, but also ‘by imagined barriers that they erect for themselves’ (Chiarello, 2019: 123).
Finally, neo-institutionalist theory emphasises the formative effects of the interactions between official legal bodies, healthcare institutions, medical professional organisations and other institutional actors (e.g. human rights NGOs). Through these interactions, the meanings of the law and legal sanctions and the options for compliance are continuously negotiated. At the same time, while healthcare institutions (e.g. hospitals) are ‘doctors’ turf’, which privilege the perspective of elite physicians and afford them respect, the power of medical professional is restricted by the realities of organisational life and external actors (Heimer, 1995: 53–54). In the context of abortion, Freedman (2010: 15) demonstrated how change in organisational leadership in US hospitals subjected healthcare professionals to new institutional (religious) logics and rendered those willing to provide abortion services unable to act in accordance with their conscience.
The subsequent parts of this article examine the complex relationship between law, professions and organisations, and its impact on abortion practice in Poland. It starts by examining the coercive effects of criminal law, and it then analyses the multi-layered organisational and institutional environment, in which doctors operate and apply abortion law. It concludes by showing how professional bodies influence the individual and collective behaviour of physicians. The article indicates how deep professional and organisational structures – rather than the law or direct fear thereof – shape abortion practice in Poland.
Legal, Institutional and Professional Factors Shaping Medical Agency and the Limits of Medical Autonomy
The Chilling Effect of Abortion Law: A Case of ‘Coercive Isomorphism’?
DiMaggio and Powell viewed changes in the legal and regulatory environment as an important factor shaping common organisational behaviour and structure. They claimed that ‘coercive isomorphism results from both formal and informal pressures exerted on organisations by other organisations upon which they are dependent and by cultural expectations in the society within which organisations function’ (1983: 150). As such, their findings can be used to explain the chilling effect that the criminalisation of abortion and political pressures can have on access to abortion services (Casas and Vivaldi, 2014; Payne et al., 2013; Sheldon et al., 2020). The history of abortion law in Poland can be seen as constituting a perfect example of this phenomenon.
Under Socialism, Poland had one of the most liberal abortion regulations in the world. The Conditions of Pregnancy Termination Act 1956 (thereafter, the Act 1956) 9 permitted abortion on health and socio-economic grounds, the latter of which was initially scrutinised by the doctor and since 1959 was based on a declaration submitted by the pregnant woman. 10 For almost 40 years, trained doctors performed abortions in public hospitals free of charge. According to official statistics, the number of registered abortions exceeded 168,000 in 1965 and 135,000 in 1985 (Government Report, 1997), and unofficial estimates suggest that it could have reached 650,000 in 1985 (Szawarski, 1987: 29). However, as illustrated in Table 1, by the end of the Socialist period, the numbers began to decline and the number of abortions performed in public hospitals dropped from 105,333 in 1988 to 30,878 in 1991 (Government Report, 1999). It has been commonly accepted that this decrease was caused by the changes in the legal, political, and regulatory environment. First, in the late 1980s, the Conservative parties and the Catholic Church organised an aggressive anti-abortion campaign, which was intensified in the first years of the political and economic transition and continues until this day (Mishtal 2015; David and Titkow 1994). Second, shortly after the post-Solidarity government was formed in 1990, the Ministry of Health issued regulations requiring additional consultation with GPs, qualified gynaecologists and psychologists in cases of abortion for socio-economic reasons. 11 Finally, the number of abortions decreased dramatically after the adoption of the Act 1993, which remains in force today. 12 It is widely acknowledged that the Act was adopted as symbolic recompense for the Catholic Church for its support of the Solidarity movement in the 1980s, which contributed to the collapse of the Socialist system (Zielińska, 1990). While presented as ‘abortion compromise’, it was heavily influenced by politicians and medical professionals closely linked to the Church.
Until 27 January 2021, abortion was lawful under Article 4(a) para. 1 of the Act 1993 in cases where:
Pregnancy endangers the mother's life or health; Prenatal tests or other medical examinations indicate a high risk that the foetus will be severely and irreversibly damaged or suffer from an incurable life-threatening illness (in such cases, abortion can be performed until the foetus is capable of surviving outside the mother's body)
13
; There are strong grounds for believing that the pregnancy is the result of a criminal act (in such cases, abortion may be performed only until the end of the 12th week of pregnancy).
In cases falling under the first two categories, the health-related risks must be certified by a physician other than the person performing the abortion, or by another qualified person chosen by the woman (Article 4(a) para. 6). In such cases, according to Article 4(a) para. 3, the abortion shall be performed by a qualified doctor in a hospital (hence, only abortions on the ground of rape or incest can be performed in private practices). However, as noted by the Council of Europe Commissioner for Human Rights (2007: 95), ‘even when [doctors] do issue a certificate, the doctor who performs the termination can question the certificate's validity and refuse the service’.
The 1993 Act is a typical piece of abortion legislation that provides a defence for doctors, stipulating the circumstances that exclude criminal liability. Under the Polish Criminal Code 1997, 14 the performance of an abortion that falls outside the scope of the Act 1993 is considered an ‘offence against the life and health’ of the woman and/or the ‘conceived child’, and it is covered by Articles 152–154 (Chapter 19). Under Article 152 § 1 and § 2, ‘whoever, with consent of the woman, terminates her pregnancy in violation of the law’, or ‘renders assistance to a pregnant woman in terminating her pregnancy in violation of the law or persuades her to do so’ is subject to imprisonment of up to three years. Article 152 § 3 stipulates long-term imprisonment for abortion performed after the foetus has reached viability. Under Article 153, performing abortion without the woman's consent carries a prison sentence up to eight years. Article 154 § 1 provides for up to 10 years of imprisonment for performing an abortion that causes the death of the pregnant woman. It is worth noting that women seeking or having abortions are not committing an offence, only the people who terminate the pregnancy or render assistance in doing so. This is important in the age of medical abortion and telemedicine. Women purchasing abortion pills, of which Misoprostol is the only drug registered in Poland and available on prescription (officially used for inflamed joints and gastric ulcers), are not committing a crime. According to Article 68 para. 5 of the Pharmaceutical Law, they can also purchase other abortion pills online for private use. 15 However, as discussed below, others, for example, friends or family members, who pay for the drugs may be reported to the police and prosecuted.
As illustrated in Table 1, the number of registered abortions performed officially by public healthcare providers is strongly correlated with legislative and regulatory changes (Girard and Nowicka, 2002; Nowicka, 2011). Except for a brief spike in registered abortions – linked to a short-lived re-introduction of the socio-economic indicator in 1997 16 – the number reached a record low of 124 terminations in 2001. The official number of registered abortions started to increase slightly in the last years of the centre-right government led by the Civic Platform, and it remained roughly constant, even after the populist Law and Justice party came to power in 2015. However, data collected recently by FWFP (2020) show, alarmingly, that the overall number of abortions provided under the therapeutic indicator in Poland fell by 60% from 55 in 2016 to 22 in 2017. In 2019 out of 1116 abortions, only 42 were performed on health grounds. Furthermore, they reveal large regional variations, showing that there were no official abortions performed in hospitals in the South East of Poland (FWFP, 2020). This could be associated with a series of legislative and judicial initiatives instigated by ultra-Conservative groups in recent years, which aimed to restrict or ban access to lawful abortion (Kubisa and Rakowska, 2018).
The data seem to support Di Maggio and Powell's claim about ‘coercive isomorphism’. While the majority of the medical profession did not support the introduction of the restrictive abortion regime,
17
the adoption of the Act 1993 led to a dramatic institutional change in officially performed abortions, almost overnight. It would also seem that this legal compliance is not simply ceremonial and symbolic, but substantive and almost universal across the sector. The harsh restrictions imposed by hospitals leading to systematic violations of women's rights have been reported by many different international human rights bodies, including the Human Rights Committee (2016) and the ECtHR. Both in Tysiac v Poland [2007] and in R.R. v Poland [2011], the Court noted that ‘the legal prohibition on abortion, taken together with the risk of their incurring criminal responsibility under Article 156 § 1 of the Criminal Code, can well have a chilling effect on doctors when deciding whether the requirements of legal abortion are met in an individual case’ (§ 114–116; § 193). This was further reiterated by one of the doctors, interviewed by the STER Foundation, who summarised the chilling effect of the Polish abortion law as follows: The law is broken, doctors are very reluctant to interrupt pregnancies. Even in the case of spontaneous miscarriages, which are frequent, doctors do not want to deal with patients because they are afraid that someone will suspect that it was an abortion. Doctors (…) are afraid that even if the abortion was legal, someone would prove that the indication for that abortion was false (2018: 66).
However, such interpretation does not take into account the disjunction between institutional (official) behaviour in hospitals and individual (covert) behaviour of particular physicians concerning the provision of abortion services. It is commonly accepted that the estimated number of clandestine abortions in Poland, although impossible to assess precisely, has oscillated between 80,000 and 150,000 a year since the 1993 legal reforms (FWFP, 2013). The disjunction could be seen as a deliberate strategy employed by healthcare institutions to offload the legal responsibility for abortion care onto individual doctors operating outside the law. This is becoming particularly true in light of the development of medical abortion and telemedicine, where such responsibility can be ‘offloaded’ onto patients and/or healthcare systems abroad. Such phenomena are not new and have been noted in the Irish context as examples of ‘peripheral governance’ (Fletcher, 2012). This interpretation would indicate that compliance is much more symbolic or ‘ceremonial’ than the numbers might suggest, that is, doctors refuse to provide abortion services in public hospitals, but provide the same services privately and unlawfully. What remains true is DiMaggio and Powell's (1983: 150) observation that the fact that the behaviour is ceremonial, and not based on internalisation of the new legal rationality, does not mean that is inconsequential.
Furthermore, the Polish case study corroborates the findings of more recent neo-institutionalist and law and organisation studies demonstrating that the law is always a result of continuous coproduction of individuals, institutions and professions (Chiarello, 2019; DiMaggio and Powell, 1983). The cases brought against Poland before the ECtHR clearly demonstrate that Polish physicians systematically construct restrictive interpretations of abortion law, erecting additional and wholly unnecessary medical and procedural barriers that prevent women from accessing lawful abortion services. The STER Report (2018), quoted above, suggests that individual doctors are motivated by the fear of legal sanctions. However, neo-institutionalist theories indicate that very often the perceived threat of negative legal consequences – constructed through the interaction between professionals and institutions – is far greater than the actual threat. The next section examines the data concerning the levels of criminalisation of abortion to determine the nature and the extent of such threat and the coercive influence of law and law enforcement institutions on individuals and healthcare providers.
Criminalisation of Abortion: Exaggerated Legal Threats?
In Poland, the state institutions involved in criminal procedure are the police and the prosecutor's office. First, the police or the prosecutor's office registers the case. Subsequently, initial investigative stages are undertaken to determine if there was a violation of the penal law and to establish the perpetrator. The prosecution can then either refuse to initiate formal proceedings or, when sufficient evidence is collected, can initiate formal prosecution. Consequently, proceedings can be either discontinued or the case can be brought before the court, which can find the defendant guilty, not guilty or discontinue the case. As mentioned earlier, the quality of the data collected from the Government Reports on the implementation of the Act 1993 is poor. However, despite the shortcomings, data analysis reveals an interesting and complex correlation between criminal law and abortion practice. Chart 2 summarises government data concerning the criminalisation of abortion in Poland between 1997 and 2017. These have been systematised under five headings: (a) cases registered under the provisions of the Criminal Code stipulating offences against the women and the foetus, (b) cases registered under Art. 152 of the Criminal Code (abortion with women's consent), (c) cases discontinued, (d) cases resulting in prosecution, and (e) cases in which the prosecutor refused to initiate formal proceedings (Figure 1).
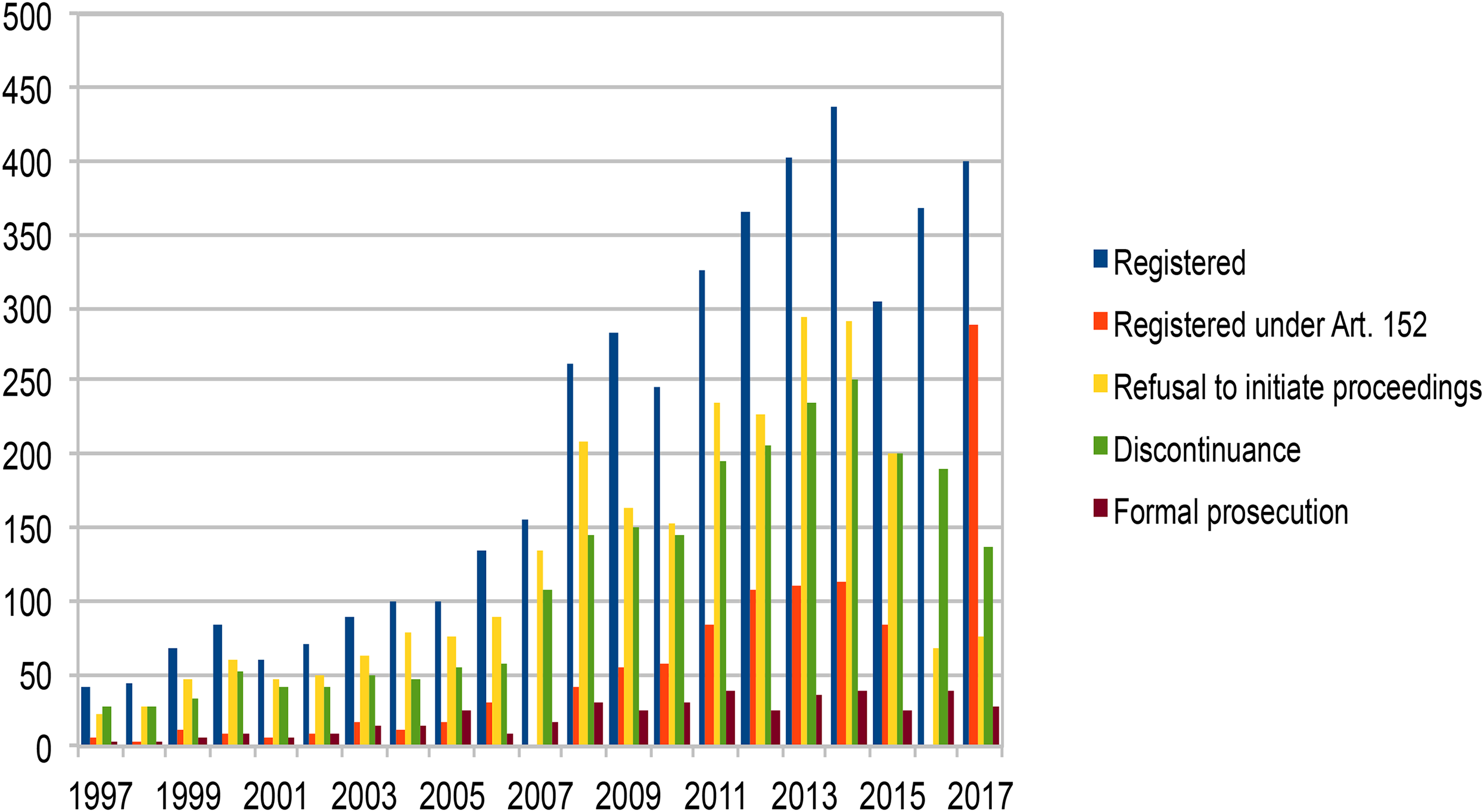
Police and criminal proceedings concerning abortion registered in Poland between 1997 and 2017.
First, what becomes immediately clear is that, from a relatively large number of registered cases, only a small number leads to a formal prosecution. In most registered cases, the prosecution services refuse to initiate formal proceedings, or, if initiated, such proceedings are usually subsequently discontinued due to lack of evidence. The number of cases that results in a formal prosecution before the court constitutes approximately 10% of all cases registered under Articles 148, 149, 152, 153, 154, 157a, 157, and 160, that is, offences against a pregnant woman and/or a foetus, which include manslaughter, neonaticide, abortion with consent, abortion without consent, injury to the ‘conceived child’, and exposure of the pregnant woman to health risks. The number of registered cases rose during the time when the centre-right Civic Platform government was in power (2007–2015), but the number of cases brought before court remained low. For instance, in 2000 out of all 83 registered cases related to pregnancy (Articles 148–160), 59 were registered under Article 152. However, out of the 83 registered cases, only nine cases were formally prosecuted, 52 have been discontinued, and in nine cases, the prosecution refused to instigate proceedings (the 13 remaining cases were carried forward). In 2013, the overall number of registered cases reached 599, out of which 293 were registered under Article 152. However, only 35 cases reached the court through formal prosecution; in 109 cases, the prosecutor refused to instigate the proceedings; and in 234 cases, the proceedings were discontinued. In 2017, out of 289 cases registered under Article 152, only 27 led to formal prosecution, while 136 were discontinued and 75 resulted in a refusal to instigate proceedings. There is no indication as to whether people prosecuted for the offences under Art. 152 were doctors, family members or abortion travel organisers, all of whom could be said to provide or aid in the provision of abortion services.
Most tellingly, most Government Reports do not provide disaggregated data concerning the number of cases leading to convictions, making it impossible to establish how many doctors were convicted under Article 152 over the years. Writing in 1995, Kulczycki (1995: 475) noted that ‘not one of the 53 cases of alleged illegal abortion investigated in the law's first year resulted in a conviction. Further, there were 30 cases of false denunciation, and one physician suspected of performing an illegal abortion committed suicide’. Kulczycki's account illustrates well the atmosphere of the early years of criminalisation. The denunciation of ‘abortionists’ has been conducted periodically by Conservative groups ever since. However, the vast majority of registered cases, stemming from denunciations, result in discontinuation because of lack of evidence. Unless a doctor finds residues of abortion pills inside the woman's body, the police and prosecutors are unable to establish whether the miscarriage was spontaneous or induced, or identify the person suspected of performing the abortion. This suggests that in practice medical doctors have been operating relatively freely or at least that the fear of criminal sanctions is not based on facts. Furthermore, there seems to be little evidence that the medical profession is subject to criminal sanctions by state institutions. However, this may change in the near future, owing to the increased scrutiny of abortion practices by prosecutors following the recent judgment of the Constitutional Tribunal. Signs that the attitude of public authorities toward abortion is changing are already visible. In January 2021, a man was sentenced to six months in prison for purchasing abortion pills for his partner (Nowak, 2021). In this instance, the prosecution services and the courts acted with unusual severity, as an act of this kind would, until recently, have typically resulted in a suspended sentence or a discontinuation of proceedings. However, it is worth noting that the sentence did not affect a medical professional, but someone close to the woman. In fact, although they were under no legal obligation to do this, it was the doctors who were providing her with post-abortion care that informed the police about the incident. For the time being, the number of prosecutions, publicised trials and incidents involving the naming and shaming of doctors performing illegal abortions remains very low. This means that the medical profession has aligned itself with the officially articulated aims of the Polish state without particular direct insistence from public institutions.
Scholars studying the emotions of healthcare professionals in other countries have made similar observations. For instance, Duffy et al. demonstrated in the Irish context that the refusal to engage in certain forms of abortion care stems not necessarily directly from coercive regulation, but from fear that such actions might potentially be rendered unlawful in future. In other words, physicians’ behaviour is not straightforwardly related to legal frameworks, and it stems from fear of ‘an imagined – but unrealised – futurity’ (2018: 17). The participants of the STER project confirmed that fear of sanctions is not the primary driver of individual behaviour, that is, the reluctance or refusal to provide lawful abortion services. Some firmly stated that ‘it is not about the legality of it’ (2018: 40). Instead, they claimed that physicians are often governed by the fear of being labelled ‘abortionists’ (2018: 67), a label that could potentially ruin careers. Others saw ‘cowardice and opportunism’ as the main causes for the behaviour of medical professionals with regard to abortion (2018: 68). As eloquently summarised by one of the participants, ‘in medicine, your opinions can help you advance’ (2018: 42).
These quotes indicate that some doctors utilise the potential threat of sanction as a self-exculpatory justification for inaction. Furthermore, the quotes suggest that doctors are prepared to deny a woman a lawful abortion – often violating the law – to comply with perceived social expectations. They imply a hierarchy of normative orders, in which moral and professional values acquire higher status than legal norms. In this respect, the quotes are consistent with earlier findings by De Zordo and Mishtal, who argued that not criminalisation, but fear of stigmatisation underlies many decisions to refuse access to lawful abortions. In their study, physicians identified fear of stigmatisation ‘by colleagues, the media, and the general public’ and well as fear of ‘potential or perceived harassment by the Church’ as the main factors shaping their behaviour (2011: S35). STER findings, however, further indicate that individual doctors do not only exaggerate legal threats, but also exploit them to secure their own professional position and status.
Consequently, the above analysis suggests that the restrictive interpretations of abortion law by the medical profession can only partially be seen as a result of ‘coercive institutional isomorphism’. While criminalisation of abortion constitutes an important element of the legal framework introduced in Poland in 1993, the enforcement of the law is far less severe than suggested by the abortion practice in healthcare institutions. In fact, the threat of criminal sanctions and socio-cultural expectations seem exaggerated in the eyes of the individual professionals. This finding corroborates the late neo-institutional accounts that point at other institutional factors influencing the construction of the meaning of legal norms and associated threats. The next section demonstrates that rather than speaking of the chilling effect of the law it would be more accurate to speak of the chilling effect of institutional and professional relationships.
Institutional Factors Shaping Medical Agency: A Complex System of ‘Feudal’ Hierarchies
So far, the analysis has demonstrated that, while implementation of the law by enforcement agencies can certainly shape the scope and content of abortion laws, these factors are not able to explain comprehensively the behaviour and attitudes of Polish physicians in relation to the provision of abortion services. While De Zordo and Mishtal (2011: S35) argued that restrictive practices are caused by poor knowledge of the law and fear of stigmatisation, the study conducted by the STER Foundation found that medical reticence in relation to abortion was determined by fear of negative consequences at work. Some doctors admitted that their contracts were often contingent on compliance with conservative hospital policy. One STER interviewee summarised the physician's fear of dismissal, unemployment and pressures from employers as follows: Where I live people are afraid to lose their jobs (…). If I lose my job at the hospital, I have nowhere to go. (…) It is all about fear (2018: 29).
Furthermore, although the majority of gynaecologists claimed that they felt no pressure from their supervisors, some agreed that hospital directors might influence doctors’ attitudes, particularly through financial decisions. For instance, employers or private hospital owners may decide if some procedures will or will not be contracted by their institution and, therefore, performed in the facility (STER, 2018: 53). One STER interviewee noted that, while ‘directors of the medical institutions, theoretically have no impact [on doctors’ decision-making], (…) in practice they may exercise direct or indirect pressure on working doctors and medical personnel’ (2018: 53). Furthermore, age, experience and position have been identified by the STER Report as one of the most important reasons for the doctors’ conservative interpretation of the abortion law and lack of engagement in abortion debates. While ‘older doctors’ had almost unlimited freedom, ‘younger gynaecologists’ could not exercise any decision-making power (2018: 41).
On the one hand, these findings confirm the importance of emotions such as fear in the construction of legal meanings in abortion practice (Duffy et al., 2018). On the other hand, they emphasise the need for micro-level analysis, that is, the examination of employment structures for the understanding of institutional environments. The following analysis shows how the legal framework regulating employment is an important – although typically entirely omitted – factor shaping abortion healthcare.
Legally, employment relations in Polish hospitals are shaped by a number of legal provisions set out in the Act on Healthcare Practice 2011, 18 the Act on the Professions of Physician and Dentist 1996 19 and the amended Labour Code 1974. 20 According to Article 49 of the Act on Healthcare Practice 2011, in a public hospital the authority is concentrated in the hands of the CEO, that is, the director or manager of the hospital, his/her deputies, chiefs of units and senior nurses. The employment position of a doctor working in a public hospital has been described as ‘autonomous subordination’ in Polish literature (Karkowska, 2012: 81). The doctrine suggests that the doctor should have autonomy with regard to clinical decision-making, but may be subject to organisational, logistical and economic decisions of the healthcare provider (2012: 81). However, the actual scope of autonomy depends on the specific employment circumstances and practices in a particular hospital. In some instances, employers provide very detailed contracts, in which case, the doctor becomes simply a contractor who performs set tasks. Private hospitals have much more autonomy in shaping employment relationships, which usually leaves employees more vulnerable, albeit better paid.
In fact, highly hierarchical structures are deeply ingrained in the institutional memory of healthcare institutions in Poland (Kubot, 1979, 2002). Under the Socialist system, hospitals were operated by the state. Chiefs of units performed clinical, administrative and economic functions. The chiefs of units could take financial decisions concerning particular treatments and the unit as a whole and could give professional orders that needed to be followed. They organised working times and responsibilities of all members of staff, who were directly accountable to them. At the same time, however, chiefs of units bore sole responsibility for the functioning of the unit. They could be dismissed immediately and without any justification by the hospital director, who nominated them (Kubot, 2002). While they could influence the careers of their members of staff, final employment decisions belonged to the hospital director, whose tenure, in turn, usually depended on political bodies controlled by the Polish United Workers Party. With some modifications, this system existed in Poland for over 30 years. Paradoxically, despite the socio-economic transition and legal changes aimed at creating a meritocratic system of healthcare organisation, the position of the chiefs of units has been strengthened in recent years (Kubot, 2007: 21). Despite seismic changes in the political, socio-economic and regulatory environment, which transformed (and almost destroyed) the Polish healthcare system, certain power structures remained in a largely unmodified form. The following analysis demonstrates the reproduction of old relationships of dependency and control.
At present, the director of a public hospital is appointed in a competitive procedure by the appointment committee and is employed by the Ministry of Health or the local government. According to the Act on Healthcare Practice 2011, if the competitive process does not lead to an appointment, the founding body can select, nominate, and employ the person of their choice. It is at this point that politically motivated appointments are most probable, which explains why some hospital directors continuously seek political support. The hospital director is responsible for the entire management of the public hospital and has decision-making powers with regard to employment. Additionally, she/he sets out hospital regulations, which determine the methods and conditions for providing healthcare services, commissioned by the National Insurance Fund (Dercz and Rek, 2014: 241–247). As such, the hospital director plays a crucial role in deciding whether the hospital will provide abortion services and in defining staff duties in this respect.
The role of the chief of unit remains controversial. The powers and responsibilities stipulated in Article 93 of the Act on Healthcare Practice 2011 focus on clinical skills and experience and no longer include administrative or economic duties. However, hospital directors often expect chiefs of units to assist them in drafting the list of healthcare services provided by the hospital (Dercz and Rek, 2014: 368–381). They are also no longer the line managers of all medical staff with regard to employment matters. Consequently, the chief of unit is no longer authorised to give professional orders to his members of staff. Instead, she/he can provide guidance with regard to the clinical work and the optimal course of treatment (Karkowska, 2012: 369–393). However, they are still considered to hold the highest clinical position in a hospital hierarchy. In the absence of uniform procedures across the country, the chiefs of units have retained substantial decision-making power concerning for instance assigning patients, dividing tasks between members of staff, and determining their working times. Therefore, in practice, due to the deeply embedded historical relevance of their position, their recommendations and guidelines are usually treated as orders by staff (Łuków and Wrześniewska-Wal, 2007). Crucially, the chiefs of unit play an important role in their staff's professional development overseeing their progression and recommending them for promotion. They often supervise their training and evaluate different stages of specialisation of early career physicians in teaching hospitals (Karkowska, 2012: 353–374).
Furthermore, scholars have argued that the actual relationship of subordination and the hierarchical dependency between the chief of unit and a doctor working in the unit has been strengthened in recent years (Łuków and Wrześniewska-Wal, 2007). While many doctors are employed in hospitals on short fixed-term contracts (enjoying little labour law protection), the chiefs of units can be contracted for six- to eight-year periods, with the possibility of re-election. In addition, hospital directors who have the power to employ the chief of unit are known to refuse to employ the person chosen in a competitive process by a special selection committee. In an audit conducted during 2013–2014, the Polish Supreme Audit Office found that many chiefs of units obtained their positions in a non-competitive process and some of them were employed indefinitely (NIK 2014). Furthermore, as the current Act on Healthcare Practice 2011 allows for hospital units to be led by doctors other than chiefs of units, who are nominated by the hospital director, many hospitals choose this option to circumvent the legal requirements for a competitive appointment procedure. All this has been said to undermine the integrity of and trust in the medical profession (Karkowska, 2012).
As mentioned earlier, employment, professional and educational structures overlap and influence each other. Chiefs of units often enjoy the support of chambers of physicians, trade unions as well as higher education institutions. As a result, they constitute the most privileged and influential group of employees in the healthcare system. In fact, chiefs of units have so much power that the relationship between them and other members of staff are often described as ‘feudal’ and the position of the regular medical staff as ‘serfdom in independence’ (Kubot, 2007: 22). These ‘feudal structures’ are deeply embedded in the legal and administrative framework and in professional cultures and include relationships between healthcare staff and hospital directors as well as regional and national consultants. Furthermore, the legal frameworks allow for the appointment of hospital directors to be often politically influenced. As Conservative parties have dominated the political arena for decades, it comes as no surprise that the main jobs in public healthcare institutions are dominated by people who conform to the Conservative (and/or right-wing) political agenda, supported by the Catholic Church.
One of the most striking examples of the hierarchical structures influenced by Conservative politics is that of the former hospital director and regional gynaecological consultant, Professor Bogdan Chazan, supported by the Catholic Church and right-wing politicians. According to the participants of the STER study, because of Chazan's well publicised anti-abortion views and decision-making power – able to ‘ruin the career of young doctors’ – members of staff in his hospital never performed abortions (2018: 40–42). Chazan's example is not the only one. Maintaining good relationships with local politicians and clergy is often a priority of the hospital management in smaller towns and villages. In such places, the medical community will try to please local authorities by limiting access to abortions, to receive financial and professional benefits (STER, 2018: 53).
The above analysis of the legal administrative provisions explains the variations in the provision of abortion services between regions and hospitals in Poland, identified in the annual report of the FWFP (2020). The analysis also demonstrates that the clinical autonomy of the early career doctors in Polish hospitals is very limited. The vertical relations of subordination hinder the ability to build sustained modes of resistance. In addition, the above analysis shows that the fragmentation of the medical profession, noted by McGuinness and Thomson (2015: 197), is a phenomenon that is not exclusive to the Anglo-American context. Importantly, the analysis of Polish institutional realities demonstrates that tensions can be observed not only between different professional groups, but also within one professional subfield. Such fragmentation and heterogeneity, tied to deep historical foundations, are constantly reproduced by institutional structures. However, it is important to remember that these institutions do not operate in a vacuum. As pointed out by neo-institutionalist scholars, they are shaped by professional standards and values (DiMaggio and Powell, 1983). The following section examines the impact of official medical organisations on healthcare institutions in the context of abortion practice in Poland. It demonstrates that the role of such bodies in shaping abortion law and medical behaviour bears a certain resemblance to similar organisations in the Anglo-American context.
The Role of Professional Bodies in the Construction of Legal Meanings
Neo-institutionalists have long argued that processes of professionalisation play an important role in the emergence of institutional isomorphism. Every day professionals interpret legal norms and construct potential consequences of non-compliance, thus contributing substantially to the process of legal co-production (Edelman et al., 1992). The role of professional networks in such co-production has been widely documented (Chiarello, 2013; Heimer, 1999; Larson, 1977). The following analysis shows how even under circumstances of high levels of state control through law and regulation, ‘medicine (…) can wield important powers’ (Freidson, 1993: 59). From the moment of their reinstatement in 1989, the medical organisations in Poland have been particularly active in shaping the official meanings of abortion law through litigation and professional regulation. At the same time, however, data concerning the use of professional disciplinary procedures cast some doubt over the extent of its influence on the behaviour of individual doctors and healthcare institutions.
The medical profession in Poland enjoys special protection and broad regulatory autonomy guaranteed by the Constitution 1997 21 and special legislation. According to the Medical Chambers Act 1989 (2009), 22 the main regulatory powers lie with the Polish Chamber of Physicians and Dentists (thereafter, PCPD). The Chamber regulates and supervises ‘the proper and conscientious exercise of medical practice’, determines the principles of professional ethics, oversees issues of professional liability and represents the medical professions at state level. The institutional structure of the PCPD includes a supreme and regional level. National organs consist of the National Assembly of Physicians, the Supreme Medical Council, the Supreme Medical Court and the Supreme Reviewer of Professional Liability. Accordingly, Regional Chambers include Regional Assemblies, Medical Councils, Courts and Reviewers of Professional Liability. All chambers are independent bodies of professional self-government with legal personality.
One of the first decisions taken by the PCPD, re-established in 1989 after a decades-long struggle under the Socialist rule, was to call for the restriction of the 1956 Act (PCPD, 1989). The second National Assembly of Physicians adopted the first Medical Code of Ethics in 1991 without prior consultation with the members of the medical profession, except for those who were already anti-choice (Hoff, 1994: 632). As argued elsewhere, this was possible because the main organs of the Chambers have been dominated by doctors active in the Solidarity movement in the 1980s and closely linked to the Catholic Church (Krajewska, 2021). Through these connections, the main medical professional body in Poland after 1989 became a powerful ally of the Catholic Church and an active supporter of its anti-abortion agenda. Consequently, the Code adopted in 1991 allowed doctors to ‘risk the foetus’ life only in cases where it was necessary to save the life and health of the mother and in cases where the pregnancy resulted from a criminal act’ and prohibited abortion if the foetus was diagnosed with a developmental or genetic disorder. These provisions were in clear contravention of the 1956 Act, in force at the time. As such, they were challenged by the Ombudsman, who questioned the constitutionality of the relevant provision of the Medical Chambers’ Act 1989, which empowered the Chambers to set out professional standards. In a majority judgment, the Constitutional Tribunal refused to review whether deontological norms set out in the Code of Medical Ethics violate constitutional law, on the basis that they belong to a different normative order. Nevertheless, it found that in a situation, in which those two orders diverge, doctors, who act in accordance with positive law (i.e. the Abortion Act 1956), cannot be professionally liable for violating the norms of the Medical Code of Ethics 1991. 23 This decision led to the amendment of the Medical Code of Ethics in 1993. By that time, however, the 1993 Act had already been adopted and the grounds for lawful abortion considerably restricted.
According to the current wording of Article 39 of the Medical Code of Ethics 2004, ‘a doctor providing medical treatment to a pregnant woman is simultaneously responsible for the life and health of her child’. Therefore, it is the doctor's duty to try to preserve the life and health of the foetus during pregnancy. The provisions of the Code seem to establish stricter standards of care towards the foetus than the current abortion law, even in its new restricted form. While the 1993 Act clearly indicates (albeit limited) grounds for lawful abortion, the Code expects the doctor to always balance the life of the mother against that of the foetus, placing particular emphasis on the preservation of the life and health of the latter. This directs a particularly restrictive interpretation of the legal provisions of the 1993 Act, which can lead to violations of individual autonomy, dignity and other ethical obligations towards patients, exemplified the cases of Tysiac v Poland [2007], R.R. v Poland [2011] and P. and S. v Poland [2012] (Chańska and Hartman, 2009; Korytowska, 2009). However, as demonstrated below, the PCPD is rarely concerned with violations of this kind.
The PCPD continues to engage in legal activism and attempts to shape professional behaviour. For instance, in 2015 it successfully challenged legal provisions delineating conscientious objection in medical practice before the Constitutional Tribunal. As a result, doctors are now able to declare conscientious objection without the need to suggest ‘a real alternative possibility to receive healthcare services from another doctor or medical facility’. 24 The litigation was presented as a struggle for wider professional autonomy for all doctors. However, in reality, it provided strong support for healthcare institutions wanting to restrict access to abortion and to justify their refusal to provide lawful abortion services. It also revealed the extent to which professional bodies not only conform to state policy, but can also shape the regulatory abortion framework and influence institutional and individual practice. And yet, despite the ideological and symbolic importance of these norm-setting actions, the following analysis demonstrates that the PCPD rarely imposes sanctions against doctors for violating ethical provisions concerning abortion and has limited authority among physicians.
Issues concerning professional liability are dealt with by the Supreme and Regional Reviewers of Professional Liability, which register claims, initiate proceeding and, if the case has merits, refer it to the Regional Medical Courts, where they act as the prosecutor on the case. The Court can discontinue the case if there is insufficient evidence to support the charges, or if the charges are baseless. The Supreme Medical Court hears the appeals and can refer cases back to Regional Courts for re-examination. As mentioned above, the data provided by the organs of the Polish Chamber of Physicians at both national and regional levels are limited. However, they provide a good illustration of the engagement of professional self-regulation bodies in the implementation of legal and professional standards concerning abortion.
Overall, only a small number of proceedings instigated by the Regional Reviewers have been subsequently referred to the Medical Courts, and an even smaller number has resulted in an imposition of a sanction. According to the Government's data collected between 2002 and 2007, Regional Reviewers registered 37 claims concerning abortion and Regional Courts imposed sanctions only in 13 cases, the severity of which has not been revealed (Government Reports 2003–2008). Data collected as a result of the FOI requests sent out to Chambers of Physicians indicated a similarly low number. According to the FOI responses received from 12 (out of 17) Regional Medical Courts, since 1989, they only heard 12 cases concerning the breach of Article 39 of the Code of Medical Ethics. Out of these 12 cases, only two cases resulted in the doctor being banned from practicing medicine for a period of one year, three cases resulted in a reprimand, and one in a caution (under the 1956 Act), and in one charges were dropped. More specifically, according to the data provided by the Regional Medical Court in Łódź, there were four cases concerning abortion since 1993: (a) one, in which the physician was banned from medical practice for one year for injuring a woman during an incorrectly performed abortion; (b) one concerning abortion with the woman's consent, which resulted in a reprimand; and (c) two, which were discontinued. According to data provided by the Regional Chamber of Physicians in Poznań, between 1989 and 2018, the Regional Reviewer of Professional Liability instigated nine proceedings concerning abortion, but only three cases have been referred to the Regional Court. Furthermore, since 2010, only three cases concerning Article 39 have reached the Supreme Medical Court. Out of these, two cases were referred back to respective Regional Medical Courts for re-examination, and in one all charges against the doctor were dismissed (PCPD, 2019a). These numbers are particularly striking in light of the fact that the overall number of practicing physicians over the years has oscillated around approximately 138,000, including approximately 8000 practicing gynaecologists (PCPD, 2019b).
It is worth mentioning that the proceedings concerning Article 39 of the Medical Code of Ethics 2004 can include cases where the physician: (a) acted negligently and caused harm to the woman when providing abortion; (b) refused to provide lawful abortion services; and (c) provided unlawful abortion services disregarding the provisions of the Medical Code (e.g. concerning prenatal testing). This means that the cases before the Medical Courts could have involved badly performed lawful abortions, falling within the scope of the Family Planning Act 1993. Unsurprisingly, none of the professional liability bodies has ever heard cases concerning doctors’ refusal to provide lawful abortion services.
These numbers indicate that, despite the legal activism of the PCPD, the ‘inward-facing’ activities, directed at the medical profession have a minimal impact on every-day abortion practice. Consequently, in line with many previous abortion studies, the analysis demonstrates a discrepancy between official pronouncements of medical bodies and their control of individual behaviour of medical professionals. It could be argued that professional bodies – like other institutions operating in a restrictive legal and political environment – have adopted a strategy of outward formal and symbolic compliance, and little substantive implementation. In fact, the activities of the PCPD could be interpreted as having one main aim, that is, to widen the scope of medical autonomy. Another, complementary and perhaps more plausible, explanation of the Chamber's ambivalent stance towards abortion would be that while professional bodies influence the construction of the regulatory environment in which other healthcare institutions operate, they themselves do not operate in an institutional vacuum. What can be observed in Poland is a unique symbiosis of the state, the professions and healthcare institutions, which for decades has perpetuated and reinforced very particular individual and collective behaviour with regard to abortion (Krajewska 2021). It is this symbiosis that facilitated the deep influence of the Catholic Church on abortion practice.
According to Reagan, such patterns can continue as long as medical professionals enjoy certain amount of professional autonomy. As soon as their clinical autonomy, that is, the every-day decision-making power is threatened, they turn against what they perceive as the source of threat (1997: 234). This is exactly what we could witness in Poland after the announcement of the abortion judgment of the Constitutional Tribunal (K1/20). First, in an unprecedented move, the Polish Chamber of Physicians – for the first time in decades –expressed ‘deep concern’ in relation to the restrictions resulting from the judgment (PCPD, 2020). Both the Polish Society of Gynaecologists and Obstetricians (2020) and the Polish Society of Human Genetics (2020), which have never before expressly criticised abortion law in Poland, also issued statements about the importance of prenatal diagnosis in pregnancy, which is expected to be curtailed as a result of the judgment. We could finally be seeing some mobilisation among different professional groups that could become the basis for a wider alliance in support of liberalisation of abortion law. At the same time, the above analysis suggests that such attempts would be challenging due to deeply rooted institutional and (intra-)professional structures.
Conclusions
This article has examined the socio-legal factors determining the individual and collective behaviour of medical professionals in a restrictive abortion regime. It took Poland as a case study to refocus existing abortion debates and bring into foreground institutional, employment and intra-professional determinants of medical agency. As such, it aimed to juxtapose, test and critique existing theories in socio-legal abortion scholarship and neo-institutionalist studies.
Despite challenges related to the scarcity of the available data and the bifurcation of views expressed in the interviews, the analysis provided important insights about the processes and structures underlying restrictive abortion practices in Poland. First, the analysis has clearly demonstrated how the meanings of abortion law are constantly (re-)negotiated through interactions between legal, cultural, professional and, importantly, institutional norms and values. These interactions are not one-directional or vertical (following a simple implementation model), but reciprocal, complex and non-linear. The analysis has further shown that while abortion law influences access to abortion provisions, emphasis on criminalisation of abortion may obscure other important aspects of abortion healthcare. Internal professional and institutional dynamics – and the underlying legal and administrative framework – are as important as criminal law in influencing the development of abortion laws and practices. These factors are often overlooked in mainstream abortion literature. While feminist and socio-legal studies of abortion tend to emphasise political and socio-cultural determinants of abortion practice, this article has shown that healthcare institutions, such as hospitals and medical practices, and in particular the relationships inside these institutions, play a significant role in determining the way in which law is constructed and applied. The article showed how these relationships have a direct impact on the adoption of restrictive interpretations of abortion law.
Second, the analysis provides important insights for neo-institutional studies. It corroborated in the context of a late-transitional polity the findings of law and organisation scholars studying predominantly Western societies. While it showed that legal and political context is indispensable for understanding medico-professional behaviour, it also demonstrated that law and associated threats are never clear, authoritative or static. Rather, they are ambiguous and fluid, and always co-produced by a complex array of different actors. The article added a layer of additional knowledge to these findings. It emphasised the fact that professions constructing legal meanings in organisational settings cannot be seen as monolithic, promoting one specific interpretation of legal norms. Divisions between official medical bodies and medical professionals, and between different strata of physicians in healthcare institutions, contribute to the propensity of physicians to restrict access to abortion. While, officially, the medical profession enjoys unprecedented levels of corporate autonomy, due to strong hierarchical structures, the clinical autonomy of many doctors can be severely restricted. While managers and chiefs of units increase their power and privilege in their ‘feudal fiefdoms’, the rest of the profession is left fragmented, relatively powerless and disillusioned.
Finally, the article offers practical insights for the provision of abortion services in societies with restrictive abortion regimes. Strategies developed to ensure or extend access to safe abortion vary substantially. They often include litigation against, and the naming and shaming of, doctors who deny women access to lawful abortion services. While existing strategies are valuable, the present findings suggest that they need to be complemented by more inclusive initiatives focused on supporting those doctors who are willing to provide abortions. Strategies could include training and educating doctors about their employment rights or providing legal aid and support in the area of labour law. To be sure, these strategies do not guarantee liberalisation of abortion laws on their own. They will require concerted effort from different corners of liberal abortion activism. However, understanding the factors determining professional behaviour offers an additional avenue that could help gain the support of at least some constituencies of the medical profession.
Footnotes
Acknowledgements
I would like to thank the Social and Legal Studies’ Reviewers for their close engagement with my article and helpful suggestions. Many thanks also to Mairead Enright, Kate Bedford, Rosie Harding, Jean McHale and Chris Thornhill for their insightful and encouraging comments on earlier drafts.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no external funding for this publication, but this project has been part of the Birmingham Fellowship 2018-2022, Birmingham Law School, University of Birmingham.
Ethics Approval
The Project received approval from the Ethics Committee at the University of Birmingham in August 2018 (Application for Ethical Review ERN_18-1297) and was conducted in accordance with the institutional research regulations. Although all project participants agreed to be named in the article, in light of the deteriorating political situation in Poland, identifiers have been removed for protection. I would like to thank all my interviewees, for their time, honesty and commitment. The interviews have been an invaluable source of knowledge and understanding of the intricacies of the Polish abortion regime.
Supplemental Material
Supplemental material for this article is available online.