
Abstract
Mental-health patients may report more symptoms than they actually experience. Experts and laypeople often view this overreporting as a sign of malingering. We show that there are multiple pathways to symptom overreporting: carryover effects from previous tests that lower the threshold for answering affirmatively to symptom items, suggestive misinformation that escalates symptom reports, inattentive responding that promotes indiscriminate endorsement of symptoms, and personality traits that bias symptom reports in an upward direction. A one-sided focus on malingering may distract from a research agenda that may contribute to knowledge accumulation in this domain.
Some mental-health patients exaggerate their symptoms. Clinicians and laypeople often interpret this symptom overreporting as a sign of malingering (Martin, Schroeder, & Odland, 2015; Thompson, Lin, & Parsloe, 2018), a label with negative connotations such as dishonesty and antisocial traits. These connotations are also evident in how the Diagnostic and Statistical Manual of Mental Disorders–Fifth Edition (DSM–5; American Psychiatric Association, 2013) portrays malingering. According to the DSM-5, the defining feature of malingering is the intentional overreporting of symptoms, motivated by financial or legal benefits. However, whereas malingerers will engage in symptom overreporting, not everyone who overreports symptoms is a malingerer. When this is overlooked, misunderstandings may arise.
Consider, as an example, a widely used test called the Structured Inventory of Malingered Symptomatology (SIMS; Smith & Burger, 1997). The SIMS asks respondents to indicate whether or not they suffer from atypical symptoms; for example, “Sometimes I lose all feeling in my hand so that it is as if I have a glove on.” Using the SIMS, a clinician may test whether, relative to normative data, a patient endorses a heightened number of atypical symptoms. If so, the patient is said to overreport symptoms, and questions can be raised about the accuracy with which the patient describes his or her health condition. In such a case, the validity of self-reported symptoms—technically called symptom validity—becomes an issue.
However, like all symptom-validity tests, the SIMS cannot determine why a person overendorses symptoms (Bass & Wade, 2019). There might be multiple reasons why people do so, and malingering is only one of them. Therefore, the name of the SIMS reflects the unfounded assumption that all overreporters are malingerers. A similar misunderstanding may arise with the popular Test of Memory Malingering (TOMM; Tombaugh, 1996), which measures whether a person underperforms on a simple memory task. Again, malingering might be one reason why individuals perform below their true abilities, but there are a variety of other antecedents of underperformance, and not considering them may lure clinicians into drawing unwarranted conclusions. Thus, symptom-validity tests such as the SIMS and TOMM may help to define an end point (i.e., symptom exaggeration), but they are silent as to the external and intrinsic factors contributing to this end point.
In research and clinical practice, symptom overreporting is often seen as noise that should be screened out with the help of symptom-validity tests. Yet it is highly informative for clinicians to know when and why their patients overreport their symptoms. For example, patients who fail the TOMM or similar instruments may not receive accurate diagnoses or adequate treatment for conditions that are truly present, leading to relatively high health-care utilization (Horner, VanKirk, Dismuke, Turner, & Muzzy, 2014). In addition, overreporting may have deleterious effects on how a person is perceived by family members and friends (Thompson et al., 2018).
In the current article, we make the case that symptom overreporting is an interesting phenomenon in its own right and that it is a gross simplification to conceptualize it as something done only by dishonest people with a hidden agenda. There are multiple reasons other than malingering why patients might exaggerate symptoms.
Sequence of Items and Tests
Testing context may profoundly affect symptom reporting. For example, Kwan, Wojcik, Miron-shatz, Votruba, and Olivola (2012) showed that students report more symptoms on a checklist for thyroid cancer when a streak of items about general symptoms (e.g., shortness of breath) preceded items about specific symptoms (e.g., pain in throat) than when the reverse order was presented. Likewise, Andreasson et al. (2017) found that people give more unfavorable ratings to their general health condition when they first have been asked to consider a range of specific somatic and mental symptoms. Villemure, Nolin, and Le Sage (2011) used two methods to interview patients with mild traumatic brain injury about their symptoms: spontaneous free recall of symptoms and an extensive checklist on which patients had to identify their symptoms. The second method yielded consistently more symptoms than the first one. One explanation for this pattern might be that checklists may unwittingly convey the message to patients that they are expected to experience certain symptoms. Findings from all of these studies suggest that priming people with symptoms may artificially raise their symptom reports.
Germane to this are also context effects, which may occur when measures of symptoms are administered in close proximity by the same researcher or clinician in the same session (Council, 1993; Lemons & Lynn, 2016). The first measures may lower the threshold for responding affirmatively to later symptom measures, either because people may want to appear consistent in how they present themselves or because the earlier tests create an availability bias when respondents later try to disambiguate vague symptom items. Whatever the reason, symptom overreporting because of context effects crucially differs from malingering. Whether symptom-validity tests such as the SIMS and the TOMM are sensitive to context effects is, to the best of our knowledge, an open question. At the very least, this possibility should be taken into account when these tests are embedded in a longer test battery that may engender inflationary carryover effects.
Symptom Misinformation
Another pathway to symptom overreporting is providing individuals with misleading information. The misleading information may either frame expectancies about the symptoms they are going to experience or it may take the form of false feedback about their health condition. An example of the first category is a study in which participants inhaled a benign substance that was presented to them as a suspected toxin. Relative to a not-inhale comparison group, those who inhaled the substance subsequently showed an increase in reported symptoms (Lorber, Mazzoni, & Kirsch, 2007). Another illustration of the escalating effects of symptom expectations is the study by Crichton, Dodd, Schmid, Gamble, and Petrie (2014; see also Crichton & Petrie, 2015). These researchers provided some of their participants with information about the adverse health effects of infrasound (high-expectancy group), whereas a comparison group was not given such information (low-expectancy group). Next, both groups were exposed to sham and real sessions of infrasound. The high-expectancy group exhibited elevated symptom reporting from before to after exposure, whereas the low-expectancy group did not report any symptomatic changes. Furthermore, sham and real infrasound sessions induced comparable symptomatic increases in the high-expectancy group. Similar effects of expectancy manipulations on the potential of sham exposures to induce symptom escalation have been described in studies on electromagnetic fields (Witthöft & Rubin, 2013) and radio frequency (Stovner, Oftedal, Straume, & Johnsson, 2008).
As to the second category of studies, researchers have noticed that it is relatively easy to create symptom overreporting in participants by providing them with misleading feedback. For instance, Baumann, Cameron, Zimmerman, and Leventhal (1989, Study 1) gave some undergraduates false feedback suggesting that they had raised blood pressures, whereas other students were informed correctly that they had normal blood-pressure readings. Subsequently, the false-feedback group more often endorsed symptoms that laypeople associate with high blood pressure (e.g., flushed face, headaches) than the comparison group. Merckelbach, Jelicic, and Pieters (2011) had undergraduates rate the extent to which they experienced common symptoms such as fatigue, concentration difficulties, and low mood on a 5-point scale ranging from never to all the time. After a short interval, participants were interviewed about why they had evaluated the symptoms the way they did, but unbeknownst to them, two symptom ratings were manipulated by upgrading the ratings by two full scale points. A slight majority of participants (63%; n = 49) failed to notice both manipulations, as indicated by their confabulating reasons for symptom ratings they had never given. At a 1-week follow-up session, participants who had accepted the misinformation gave higher symptom ratings to manipulated symptoms than to nonmanipulated symptoms. This pattern of symptom escalation is suggestive of misinformation internalization, and it was absent in participants who had rejected the misinformation. Because of ethical considerations, studies on the escalating effects of symptom misinformation have included only nonclinical participants; however, similar phenomena may occur in clinical groups. For example, information that stresses the cognitive side effects of chemotherapy contributes to cognitive problems in cancer patients (Schagen, Das, & Vermeulen, 2012).
It is unclear whether symptom-validity tests such as the SIMS are immune to misinformation. One could argue that the SIMS largely consists of atypical symptoms that, even for misinformed people, are too unlikely to be plausible descriptions of health problems. Still, the history of medicine is replete with incredible symptoms that can be induced by misinforming patients (Wessely, 1994).
Inattentive Responding
With the increasing popularity of online surveys, the research interest in what has been called inattentive responding has also grown. Using bogus items (e.g., “I have never eaten a meal”), researchers have found that 15% to 20% of participants demonstrate careless or random responding to online survey items (Fleischer, Mead, & Huang, 2015). Even when inattentive responding occurs in a minority as small as 10% of the sample, it may have huge psychometric effects. Inattentive responding may inflate reliability coefficients, distort factor structure solutions, and artificially raise prevalence estimates of disorders (Meade & Craig, 2012).
Inattentive responding not only occurs with online surveys but also may play a role when individuals fill out symptom scales or are given neuropsychological tests. For example, Meyer, Faust, Faust, Baker, and Cook (2013) noticed that many scales assessing addictive behaviors do not contain bogus items to screen for inattentive responding. When respondents fill out these questionnaires in a careless or random way, they may easily obtain scores that exceed the clinical cutoff and that cannot be discriminated from those of patients with genuine addiction problems. This problem may also arise when people complete symptom-validity tests such as the SIMS or the TOMM in an inattentive way. Doing so would lead to overreporting and underperformance, respectively, but these have nothing to do with malingering. People who engage in this type of responding are not motivated by the prospect of incentives, and it is not their intention to impress as more impaired than they really are. Rather, they are bored or tired because of, for example, the test length or test duration. Or their genuine symptoms may interfere with their attentive capacity (Peters, Jelicic, Moritz, Hauschildt, & Jelinek, 2013).
Personality Traits
Certain personality traits may predispose people to overreport their symptoms. For example, people with high levels of negative affectivity (i.e., the habitual tendency to experience a wide range of negative emotions, including anxiety and depression) report more physical and psychological symptoms than people with low levels of negative affectivity, although their medical condition is not always found to be worse (Costa & McCrae, 1987; but see Friedman, Kern, & Reynolds, 2010). Research by Suls and Howren (2012) has clarified the mechanism behind the inflated symptom reports of people with high levels of negative affectivity. Specifically, anxiety is accompanied by an attentional bias (i.e., a heightened sensitivity to threat cues), which is associated with inflated reports of momentary symptoms. Depression is accompanied by a recall bias (i.e., a heightened accessibility of negative memories), which is associated with inflated reports of past symptoms.
Another trait that is linked to inflated symptom reports is alexithymia: the inability to identify and describe feelings. When people are alexithymic, they may misinterpret common experiences as serious symptoms, an effect known as somatosensory amplification. De Gucht and Heiser (2003) conducted an analysis on 16 separate studies that had looked into alexithymia and symptom reporting and concluded that there is a consistent and positive relationship between these two variables: The more alexithymic people are, the more symptoms they report.
There is evidence to suggest that individuals with negative affectivity or alexithymia have also raised scores on symptom-validity instruments such as the SIMS (Merckelbach, Prins, Boskovic, Niesten, & À Campo, 2018; Van Impelen, Merckelbach, Jelicic, & Merten, 2014), although further research along this line is needed. This research might profit from the voluminous literature on the psychology of symptom reporting, which shows that factors such as worrying and catastrophizing might lead to overinterpretation of common symptoms (Rief & Broadbent, 2007).
Concluding Remarks
There is a longstanding tradition in the clinical sciences to attribute symptom reports to the nature of persons and to disregard situational factors. Accordingly, the predominant view on symptom overreporting is that it indicates malingering. To be sure, malingering does exist, and in some settings (e.g., the forensic context) it occurs on a nontrivial scale (Young, 2014). However, as our review shows, there are multiple pathways to symptom overreporting, and malingering is only one of these (Fig. 1). Our review is not meant to be exhaustive. Apart from the antecedents shown in Figure 1, other factors (e.g., positive symptoms in schizophrenia; Peters et al., 2013) may encourage symptom overreporting, although these have been studied less systematically. Some authors have speculated that symptom overreporting is a cry for help, but the well-documented link between treatment dropout and overreporting appears to contradict this interpretation (Merckelbach, Boskovic, Pesy, Dalsklev, & Lynn, 2017).
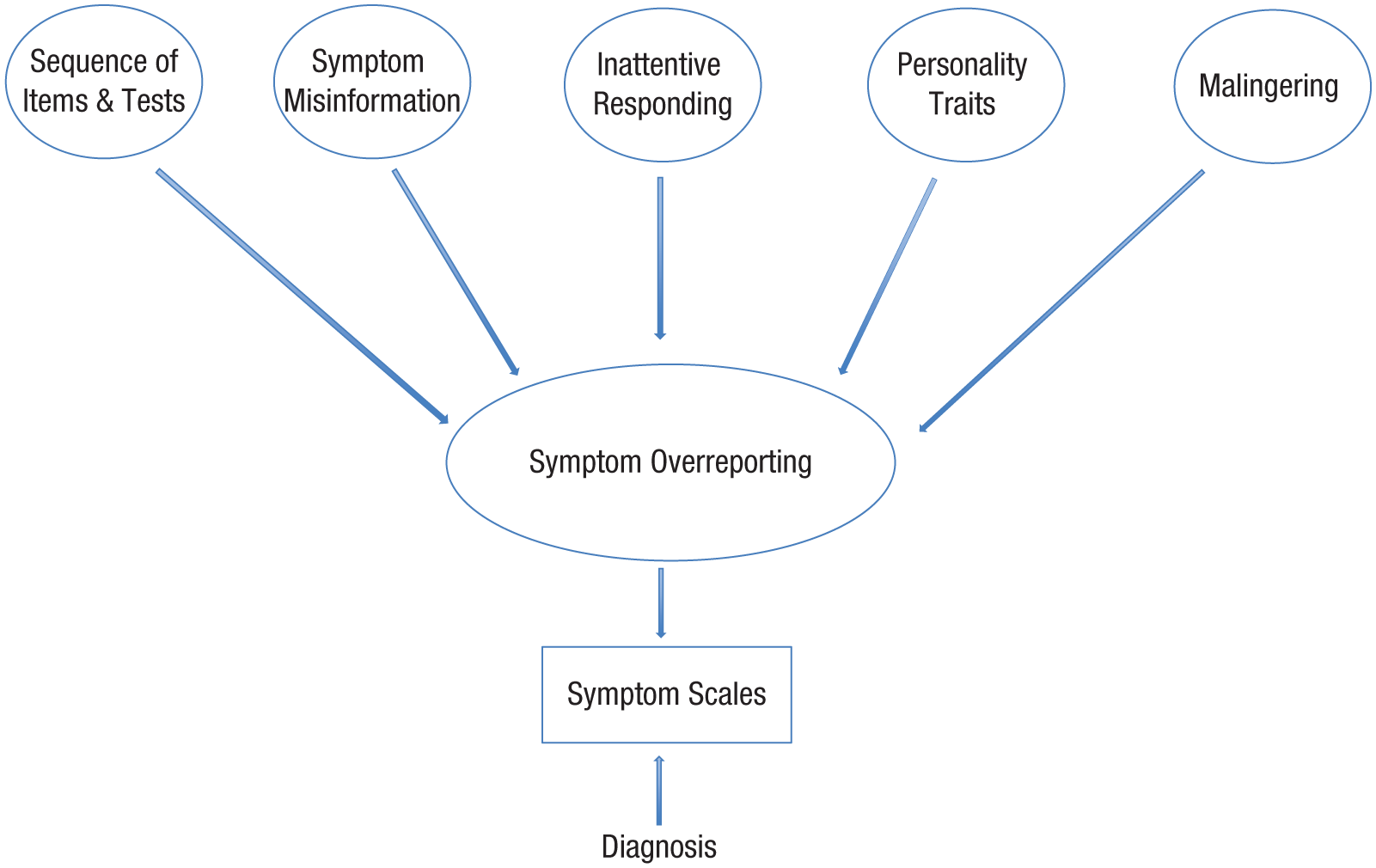
Illustration showing various antecedents that lead to symptom overreporting in patients, which in turn leads to potentially incorrect clinician diagnoses based on symptom scales. See the text for further details.
The one-sided emphasis on malingering in the literature on symptom overreporting distracts from three important research topics. The first is the harmful potential of treatment. As pointed out by Moritz and colleagues (2018), adverse effects of therapeutic interventions have long been neglected in psychology. It would be timely to systematically investigate whether interventions that provide patients with dubious expectations and post hoc misinformation produce symptom escalation. When misinformation inflates symptom reports, do these inflated reports result in overvaluing negative autobiographical memories, and does this, in turn, fuel symptom reports? We do not know, but such a symptom-memory cascade is what one would predict on the basis of the extensive literature about the memory-distorting effects of misinformation (Loftus, 2017) and the clinical phenomenon termed memory amplification (i.e., when patients become more symptomatic over time, they report more negative events from the past; Oulton, Takarangi, & Strange, 2016).
Second, to the extent that symptom overreporting is the result of negative affectivity or alexithymia, it might be amenable to treatment. Van den Bergh and Walentynowicz (2016) discussed initial studies in which interventions such as interoceptive training and affect labeling were shown to be successful in reducing symptom reports. Clearly, this is an issue that warrants further research.
Third, the findings summarized in this article may be used to improve tests assessing symptoms such that their design minimizes elements conductive to overreporting tendencies (e.g., by paying attention to streaks and context effects and by avoiding suggestive information). If overreporting through avenues other than malingering can be reduced, we could probably gain a better understanding of genuine symptoms experienced by people and a better idea of when a person is malingering.
Recommended Reading
Bass, C., & Wade, D. T. (2019). (See References). A review article about malingering and related conditions that also critically discusses the practical value of symptom-validity tests.
Merckelbach, H., Jelicic, M., & Pieters, M. (2011). (See References). Demonstrates the principle that misinformation may escalate symptom reports.
Suls, J., & Howren, M. B. (2012). (See References). A concise analysis of anxiety and depression as precursors of heightened symptom reports.