
Abstract
Due to the high absorption rate of traditional autologous fat grafting, cell-assisted lipotransfer (CAL) and platelet-rich plasma (PRP)-assisted lipotransfer were developed. The purpose of this article was to evaluate the efficacy and safety of CAL and PRP in promoting the survival of autologous fat grafting through systematic review and meta-analysis. We searched Pubmed, Cochrane Library, Web of Science, and EMBASE for clinical studies on CAL and PRP-assisted lipotransfer published from January 2010 to January 2020. Then a meta-analysis was performed to assess the efficacy of CAL and PRP-assisted lipotransfer through data analysis of fat survival rate. We also assessed the incidence of complications and multiple operations to analyze their safety. A total of 36 studies (1697 patients) were included in this review. Regardless of the recipient area, CAL and PRP-assisted lipotransfer significantly improved the fat survival rate (CAL vs non-CAL: 71% vs 48%, P < 0.0001; PRP vs non-PRP: 70% vs 40%, P < 0.0001; CAL vs PRP: 71% vs 70%, P = 0.7175). However, in large-volume fat grafting, such as breast reconstruction, both increased the incidence of complications and did not decrease the frequency of multiple operations after lipotransfer. Further prospective studies are needed to evaluate the clinical benefits of CAL and PRP-assisted lipotransfer.
Keywords
Introduction
Autologous fat grafting is a revolution in the field of soft tissue reconstruction and augmentation, and is mainly used to fill up the congenital deficiencies and soft tissue defects in plastic and reconstructive surgery, such as: filling of the face, breast, and buttocks, wound repair and breast reconstruction after breast cancer, etc. 1 Compared with other filling materials, autologous fat grafting has the advantages of good biocompatibility, easy access, abundant sources, good filling effect, and small trauma. So it is recognized as a safe and effective method 2,3 . Traditional autologous fat grafting can obtain satisfactory results early after surgery, but the long-term results are not satisfactory. The main reason is the high absorption rate (20–80%) and low survival rate after fat grafting 2,4 . Therefore, how to improve the survival rate of autologous fat grafting has become the critical factor. In order to improve the survival rate of fat graft, many methods have been proposed, including the application of cell-assisted lipotransfer (CAL) and platelet-rich plasma (PRP)-assisted lipotransfer.
CAL was first proposed by Matsumoto et al 5 in 2006, which referred to co-transplantation of aspirated fat with stromal vascular fraction (SVF) or aspirated fat with enrichment of adipose-derived stem cells (ADSCs), and was subsequently applied to the human body for the first time by Yoshimura et al. 6 Matsumoto and Yoshimura demonstrated that CAL could be used to improve the efficacy of autologous fat grafting in the preclinical and clinical trials. In this technique, the liposuction fluid is rich in SVF. Freshly isolated SVF cells contain multiple cell types, such as endothelial cells, pericytes, fibroblasts, macrophages, and preadipocytes 7 . In particular, adipose SVF provides a rich source of ADSCs. Multiple studies have shown that cytokines and growth factors secreted by ADSCs stimulate tissue repair in a paracrine manner 8 . At the same time, ADSCs promote angiogenesis of endothelial progenitor cells in SVF 9,10 . The advantages of SVF components and its ease of use have facilitated the development of the SVF-enriched ADSC techniques 11 .
PRP is a kind of autologous plasma with red blood cells removed by centrifugation. It contains platelets and other cellular components. It also has various biologically active molecules, including growth factors (such as transforming growth factor-β, platelet-derived growth factors, epidermal growth factor, vascular endothelial growth factor, basic fibroblast growth factor, insulin-like growth factor-1), cytokines, chemokines, and so on 12,13 . Because PRP is rich in growth factors and plasma components, it provides nutritional support, increases angiogenesis and the survival of fat grafts, promotes the proliferation of preadipocytes and adipose-derived mesenchymal stem cells. Its accessibility has led to the active components in autologous blood into the eyes of researchers 14 .
So far, there is no consensus in the literature on the best way to handle fat to ensure the maximum fat survival rate and the viability of grafted fat. CAL and PRP-assisted lipotransfer are the two most promising options currently. Therefore, we conducted a meta-analysis of clinical trials, cohort studies and case series of CAL and PRP-assisted lipotransfer to analyze and summarize their clinical efficacy and safety to better guide clinical practice.
Materials and Methods
Protocol
The research methodology of this study followed the PRISMA 2009 guidelines 15 .
Data Sources and Search Strategy
Two independent authors identified a systematic review of relevant articles published between January 2010 and January 2020 in PubMed, Cochrane Library, Web of Science and EMBASE. The search terms included keywords related to “fat graft” or “autologous fat” or “fat transplantation” or “lipofilling” or “lipotransfer” or “lipograft” in combination with “stromal vascular fraction” or “SVF” or “stem cell” or “cell assisted” or “ADSC” or “ADRC” or “ASC” or in combination with “platelet rich plasma” or “PRP.” The keyword search strategy for PubMed is shown in Appendix 1. The retrieval of articles and the selection of titles and abstracts were carried out independently by the two authors. Full text evaluation of qualified articles were according to inclusion criteria. Any discrepancies were resolved by discussions among authors.
Literature Selection
Data Collection Process and Quality Assessment
Data extraction was performed by two independent reviewers (A.C. and L.Z.) according to a pre-designed data extraction method. The following information was included: (a) Identity: authors, years. (b) Patients included in each study: number, age, BMI. (c) Treatments: intervention factor, stem cell isolation method, injected PRP/fat graft, recipient sites, number of operations, injected volume, volumetric measurement methods, follow-up period. (d) Outcomes: gained volume, fat survival rate, postoperative complication rate, patients Satisfaction. (e) Study design, level of evidence. For articles reporting incomplete data, we contacted the relevant authors.
Two reviewers (A.C. and L.Z.) independently scored the quality of the research and the level of evidence for each study in accordance with the Oxford center for evidence-based medicine 2011 guidelines 16 . Disagreements among reviewers were resolved through discussion.
According to the Cochrane collaboration’s tool for assessing risk of bias in randomised trials 17 , a biased risk map and a biased risk summary chart were drawn for bias risk assessment.
Types of Outcome Indicators
The efficacy of intervention measures were evaluated by fat survival rate. In the light of the incidence of complications and the frequency of multiple operations to evaluate the safety. Complications were assessed including cysts, calcification, fat necrosis, nodules, and fibrosis. Fat necrosis is the initial manifestation of ischemia and hypoxia of the grafted fat particles. Cysts, nodules and calcifications are different manifestations of the further progress of fat necrosis. Redness, swelling and subcutaneous ecchymosis that appear immediately after surgery, local infection after surgery recovering within one to two weeks, undercorrection or overcorrection, asymmetry which are not considered complications. The frequency of multiple operations was defined as repeating the same type of fat grafting surgery at the same recipient site.
Statistical Analysis
Cochrane collaboration software (RevMan 5.2) was used for meta-analysis. A total of 23 eligible articles were included to evaluate the efficacy of CAL technology, PRP-assisted lipotransfer technology and traditional fat grafting. In order to include articles that included traditional fat grafting as a control and enrich the sample data in this paper, we used a meta-analysis of the non-controlled dichotomy data, namely a meta-analysis of the single rate, to calculate the pooled estimates and the 95% fat survival confidence interval for each group using the generic inverse variance and random effect models. For evaluating the heterogeneity of the results of the included studies and exploring the differences in the results of the studies in different recipient sites, subgroup analyses were performed to calculate the inconsistent statistics (I2) of the totals and subtotals. Funnel plot was used to show publication bias.
In addition, 30 articles were included to evaluate the safety of CAL technology, PRP-assisted lipotransfer technology and traditional fat grafting. Chi-square test with Graphpad Prism 8.0 was used to evaluate whether different interventions had statistical differences in the incidence of complications and multiple surgical operations in different recipient sites.
Results
Literature Search
A total of 2,639 articles were retrieved using the predefined keywords, and another 37 were included from the references of other articles. We eliminated 1,835 duplicate articles and included 112 potential full-text articles by reading the title and abstract. After a careful review of the full text, this review finally included 36 articles. The selecting process is shown in Fig. 1.
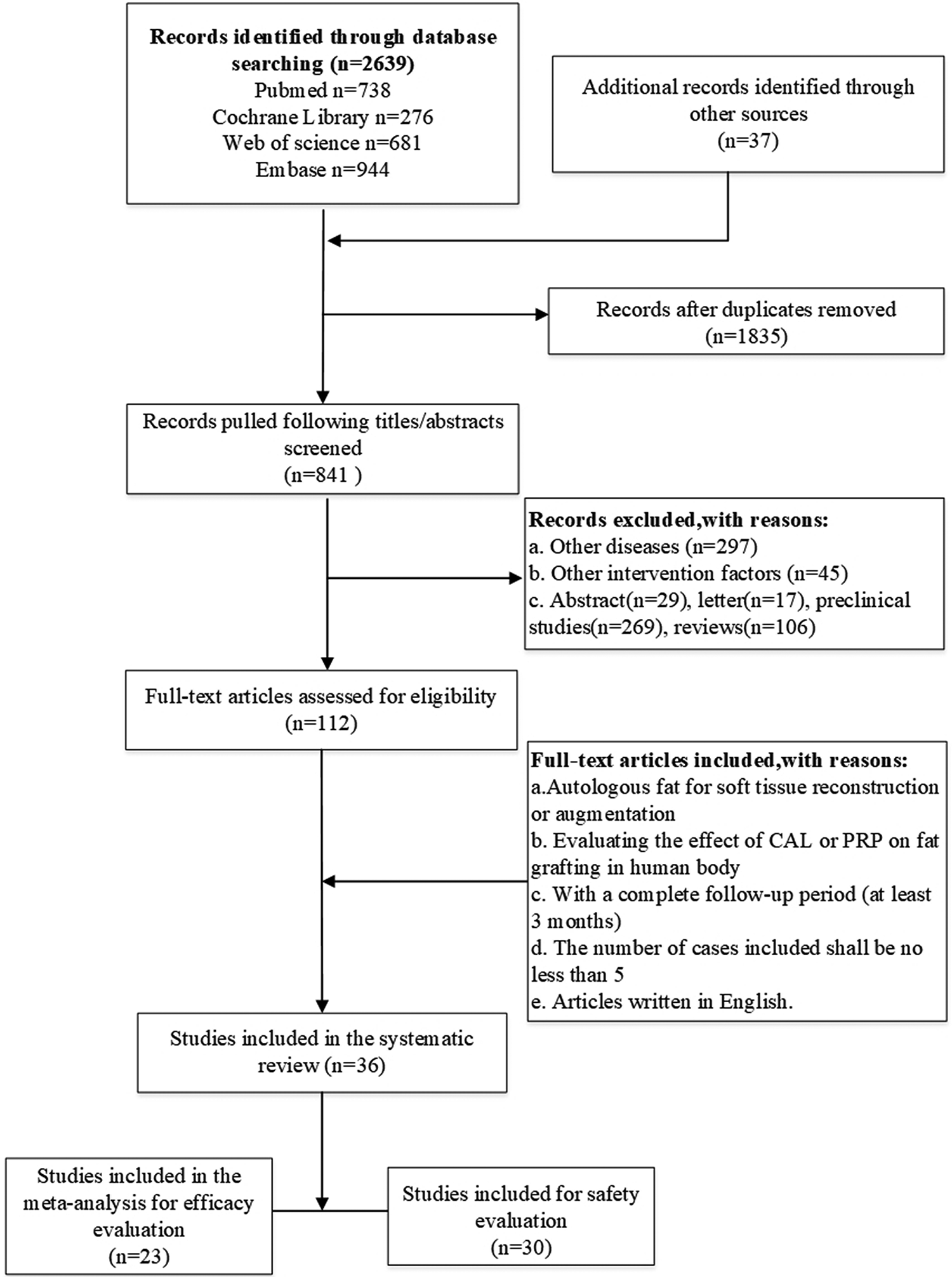
Flow diagram of the study selection. CAL: cell-assisted lipotransfer; PRP: platelet-rich plasma.
Characteristics and Quality of the Included Studies
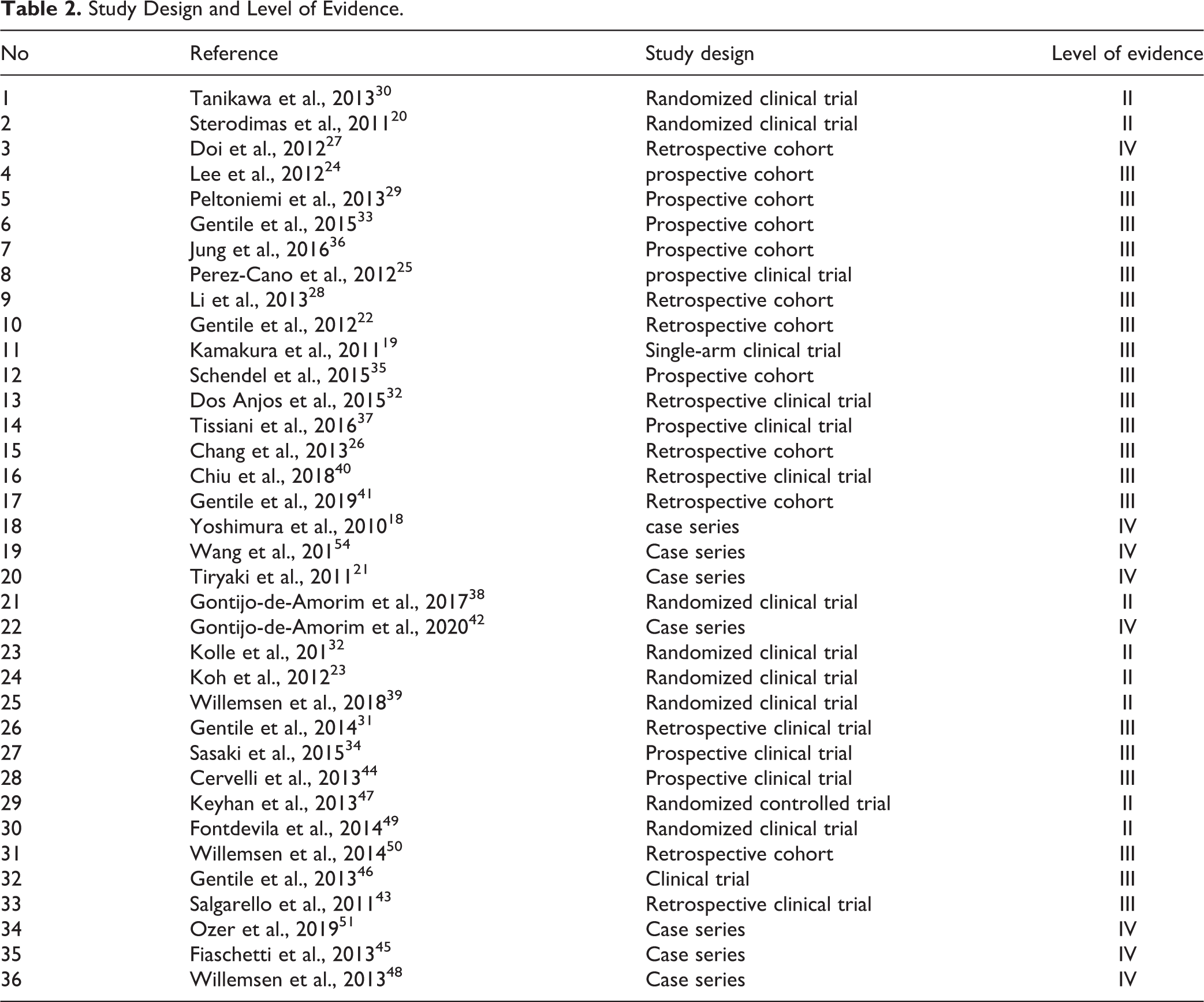
We included 36 studies with 1,697 cases 2,4,18 –51 . The basic characteristics of 36 studies are summarized in Table 1 . The included studies included randomized controlled trials, cohort studies (single-arm or double-arm), and case series. The meta analysis included 24 articles containing the survival rate of grafted fat, including 19 studies about CAL with 453 cases 2,4,18,22,23,26,28 –37,40,41 and 7 studies about PRP-assisted lipotransfer with 359 cases 31,34,44 –47,49 (there were 2 studies that included both cell-assisted and PRP-assisted lipotransfer 31,34 ) (Table 1). For safety evaluation, we assessed the incidence of fat grafting complications. A total of 31 studies reported postoperative complications 2,4,18,19,21,23 –40,43,45 –49,51 . We evaluated the quality of study design and evidence levels for all included studies based on the Oxford centre for evidence-based medicine 2011 guidelines (Table 2). Of these, 8 studies had evidence levels of II, 21 had evidence levels of III, and 8 had evidence levels of IV.
Overview of the Characteristics of Included Studies.
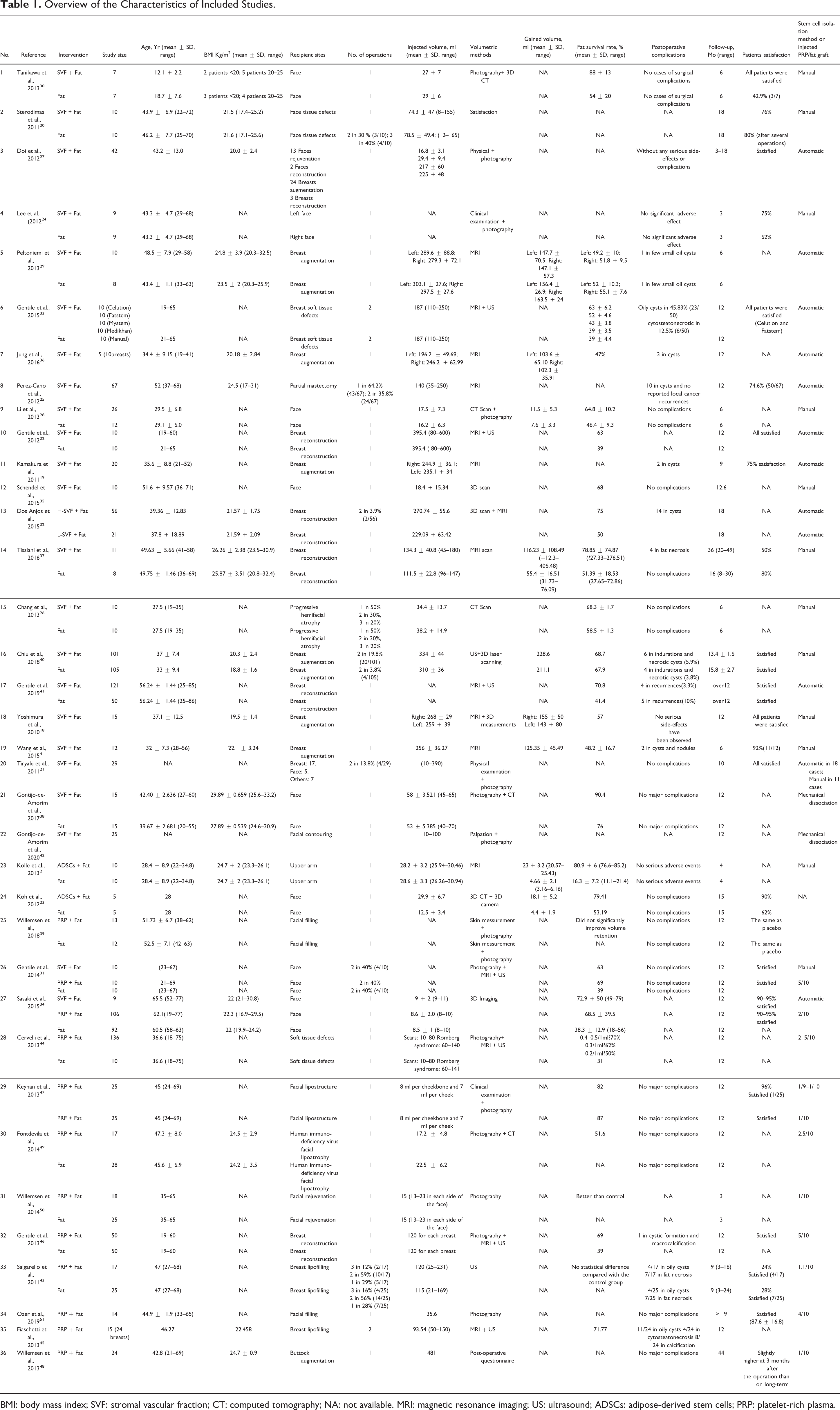
BMI: body mass index; SVF: stromal vascular fraction; CT: computed tomography; NA: not available. MRI: magnetic resonance imaging; US: ultrasound; ADSCs: adipose-derived stem cells; PRP: platelet-rich plasma.
Study Design and Level of Evidence.
Methodological Quality of Included Studies
The risk of bias was assessed according to the Cochrane collaboration group’s risk of bias tool manual 17 for eight included randomized controlled trials 2,20,23,30,38,39,47,49 (Figs. 2, 3). In the eight randomized controlled trials, the risk of each biased item was assessed by percentages. More than 25% risk of allocation concealment bias, performance bias, and reporting bias existed in the eight studies. All the included studies showed a low risk of attrition bias. To sum up, the methodological quality of included studies was feasible.
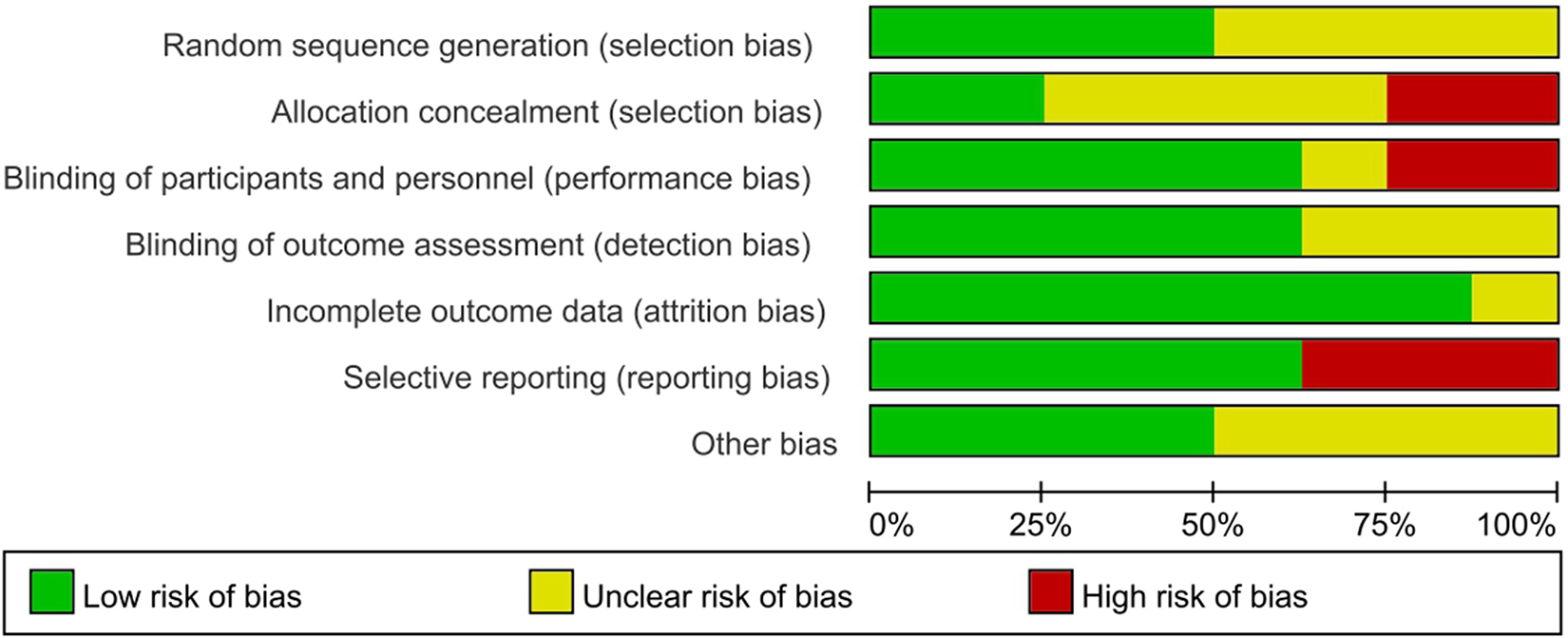
Bias risk graph: a review of the authors’ estimates of bias risk in the seven randomized controlled trials included.
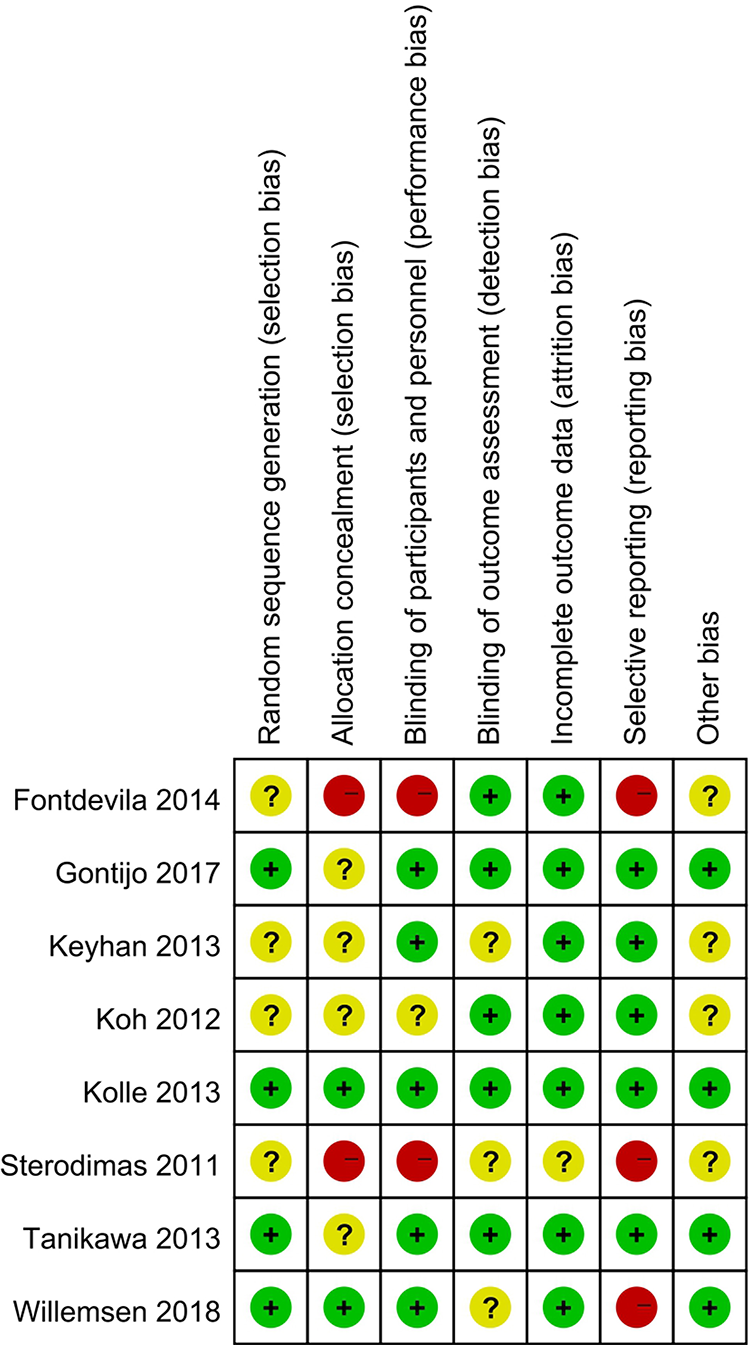
Risk of bias summary: review the author’s decisions on each bias risk item for each randomized controlled trial. Red (-): high risk of bias; Yellow (?): unclear risk of bias; Green (+): low risk of bias.
Efficacy of Cell-Assisted and PRP-Assisted Lipotransfer
According to the survival rate of grafted fat to determine the efficacy of fat grafting (the percentage of obtained fat volume to injected fat volume). In order to study the efficacy of fat grafting in different recipient areas, subgroup analyses were performed on different recipient areas (Figs. 4 –7). For heterogeneity assessment in different recipient areas, the inconsistency value (I2) of CAL is 39.4%, non-CAL is 73.1%, and PRP-assisted lipotransfer and non-PRP-assisted lipotransfer are 0%.
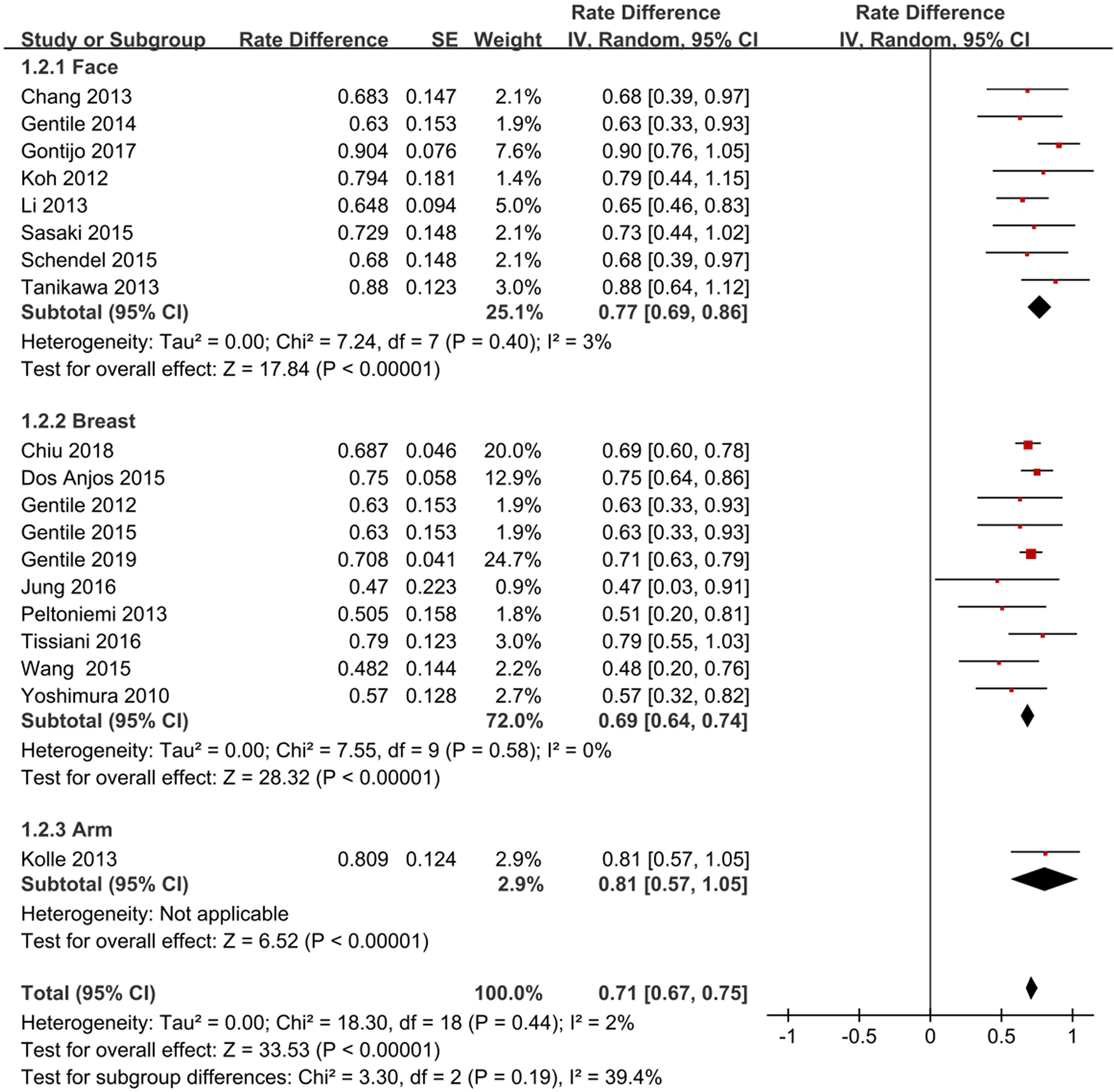
Pooled estimates of fat survival rate with cell-assisted lipotransfer at different recipient areas.
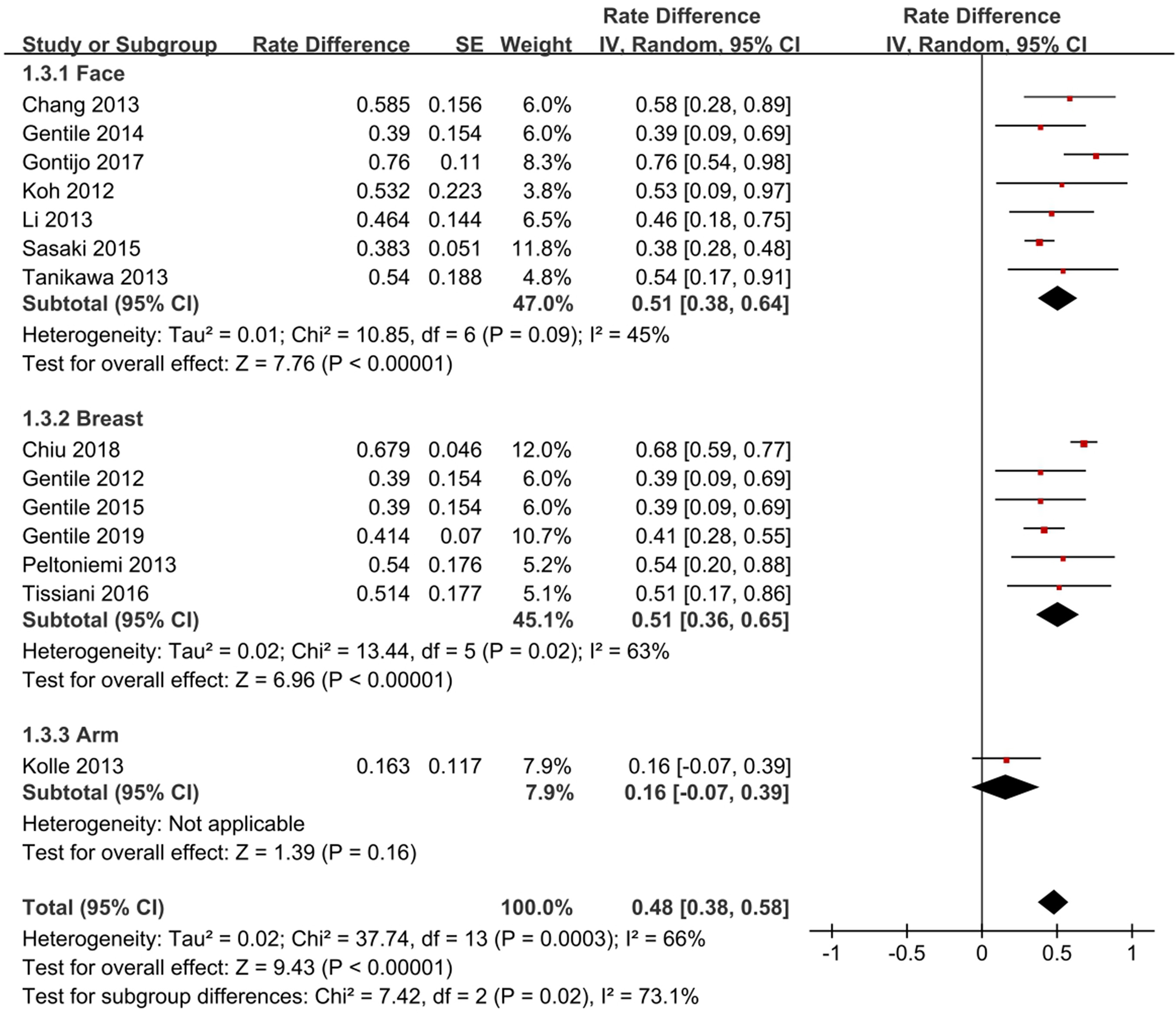
Pooled estimates of fat survival rate with non-cell-assisted lipotransfer at different recipient areas.
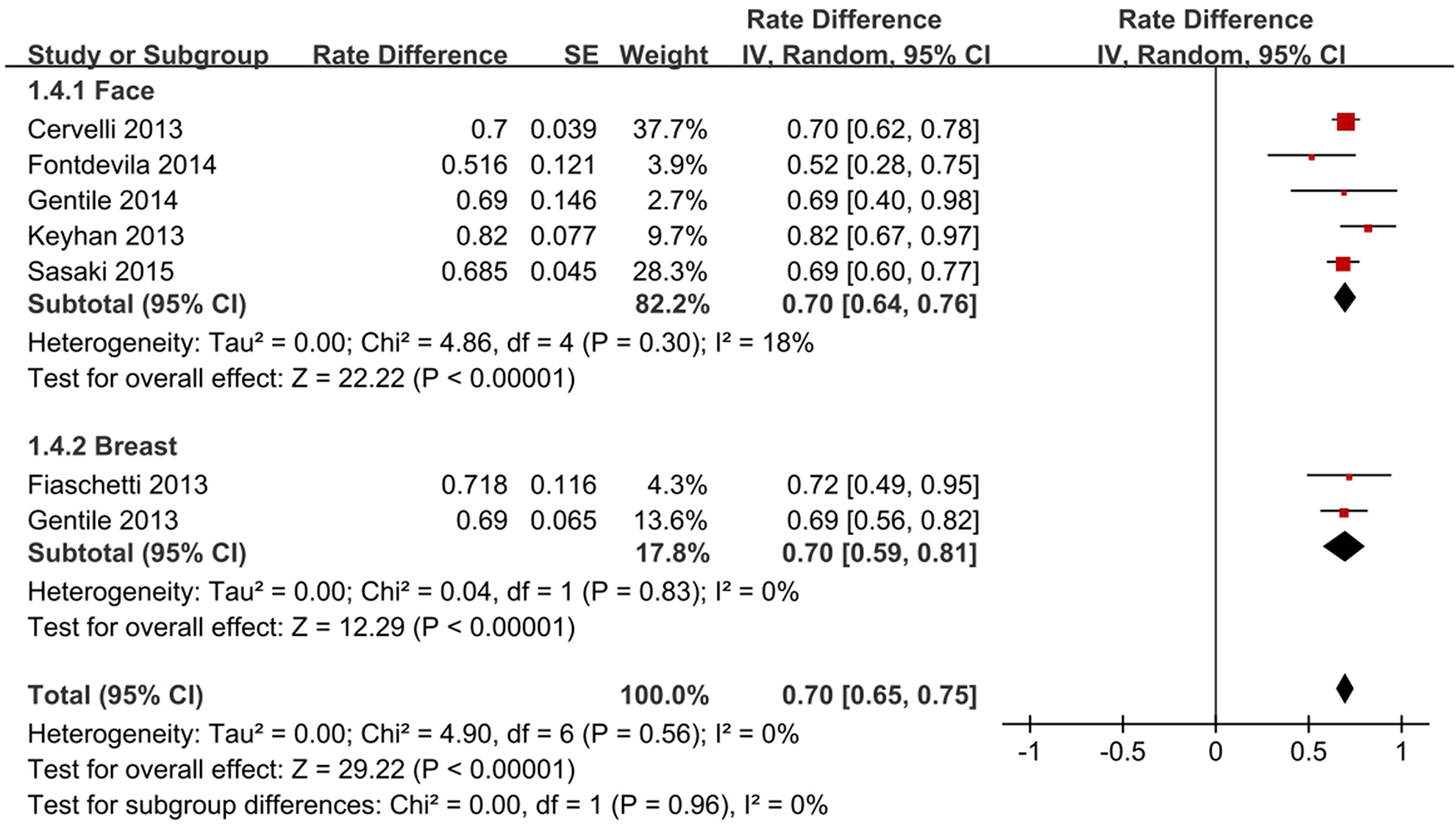
Pooled estimates of fat survival rate with PRP-assisted lipotransfer at different recipient areas.
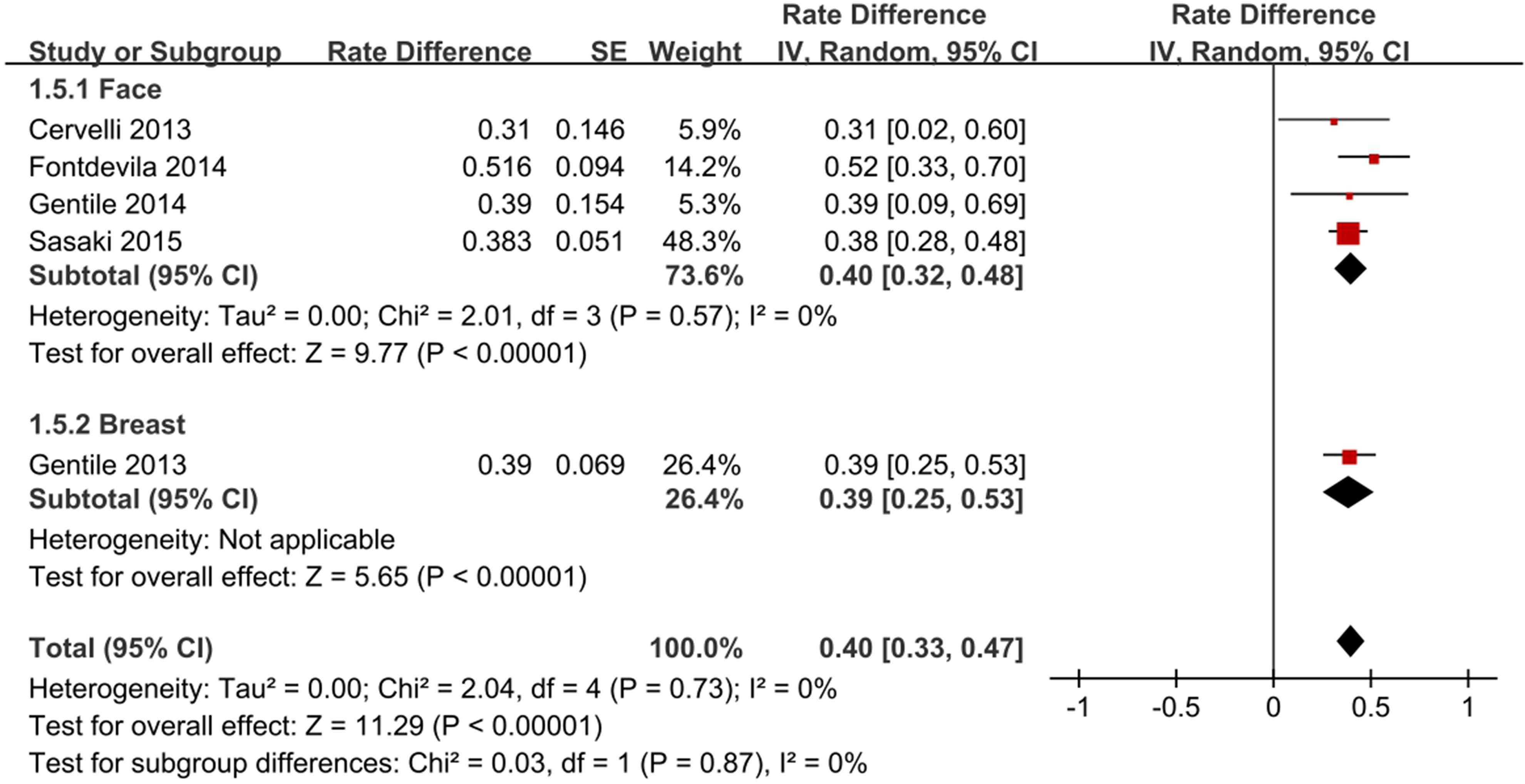
Pooled estimates of fat survival rate with non-PRP-assisted lipotransfer at different recipient areas.
Figs. 4 and 5 show that the fat survival rate of the CAL group was significantly higher than that of the non-CAL group (71%, 95% CI [67, 75] vs 48%, 95% CI [38, 58], P < 0.0001). In the subgroup analysis of the recipient areas, the facial fat survival rate of the CAL group was significantly higher than that of the non-CAL group (77%, 95% CI [69, 86] vs 51%, 95% CI [38, 64], P < 0.0001). Similarly, the breast fat survival rate of the CAL group was higher than the non-CAL group (69%, 95% CI [64, 74] vs 51%, 95% CI [36, 65], P < 0.0001). The fat survival rate of CAL group was significantly higher than non-CAL group in the only arm study 2 (81% vs 16%, P < 0.0001). As can be seen from Figs. 6 and 7, the fat survival rate of the PRP group was significantly higher than that of the non-PRP group (70%, 95% CI [65, 75] vs 40%, 95% CI [33, 47], P < 0.0001). There was no difference in subgroup analysis in different recipient areas (P > 0.5, I2 = 0%). In Figs. 4 and 6, we compared the ability of CAL group with PRP group about promoting the survival of fat grafting, and found no statistical difference between the two groups(71%, 95% CI [67, 75] vs 70%, 95% CI [65, 75], P = 0.7175).
CAL researches include enzymatic separation of SVF (including automatic separation and manual separation), non-enzymatic separation of SVF (i.e., mechanical separation), and in vitro culture of ADSCs. In order to compare the differences in fat survival rates of SVF treated by different methods, the heterogeneity assessment by subgroup analysis demonstrated that inconsistency value (I2) was 63.2% (Fig. 8). There was no statistical difference in the survival rate of fat between automatic separation and manual separation (70%, 95% CI [64,76] and 68% [62,75], P = 0.6072). The mechanically separated fat and ADSCs with in vitro culture have higher survival rate (90%, 95% CI [76,105] and (80% [60,100], P = 0.5628).
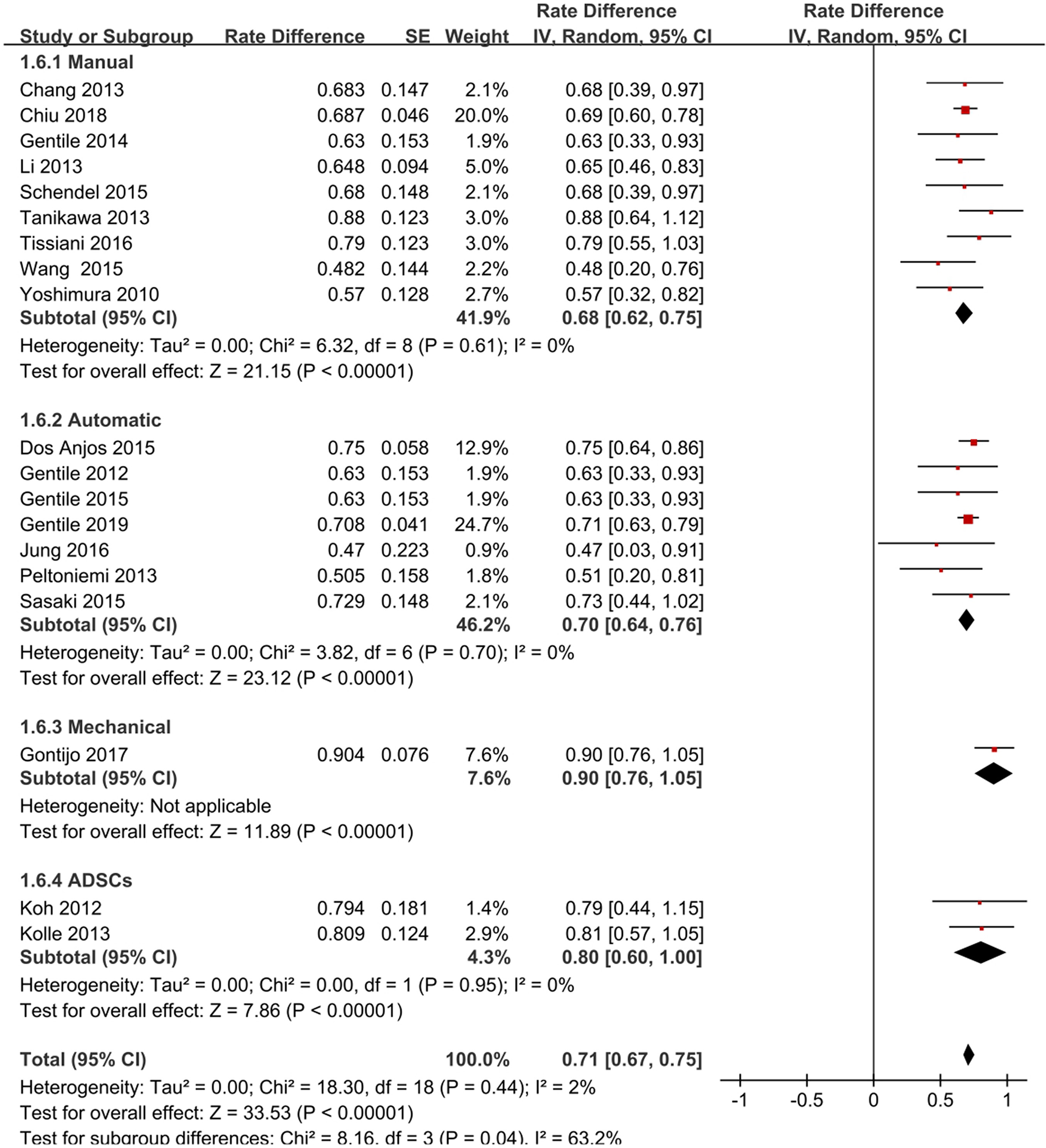
Pooled estimates of fat survival rates for different handling methods of cell-assisted lipotransfer.
Safety of Cell-Assisted and PRP-Assisted Lipotransfer
For safety evaluation, we assessed the incidence of fat grafting complications, including: cysts, calcification, fat necrosis, nodules, and fibrosis. A total of 31 studies reported postoperative complications 2,4,18,19,21,23 –40,43,45 –49,51 . The total average follow-up time was 12.2 ± 8.2 months. The total complication rate was 8.7% (125/1429), of which the cysts had the highest rate (6.0%, 86/1429), followed by fat necrosis (2.0%, 28/1429), calcification (0.6%, 9/1429) and nodule (0.1%, 2/1429). We found that all complications occurred in breast surgery, and no complications occurred in the rest of the body. Therefore, we specifically analyzed the incidence of breast complications in different interventions (Fig. 9A). The incidence of CAL complications was higher than non-CAL (12.81% [67/523] vs 6.08% [11/181], P = 0.0129), PRP group was higher than non-PRP group (36% [36/100] vs 14.67% [11/75], P = 0.0016).
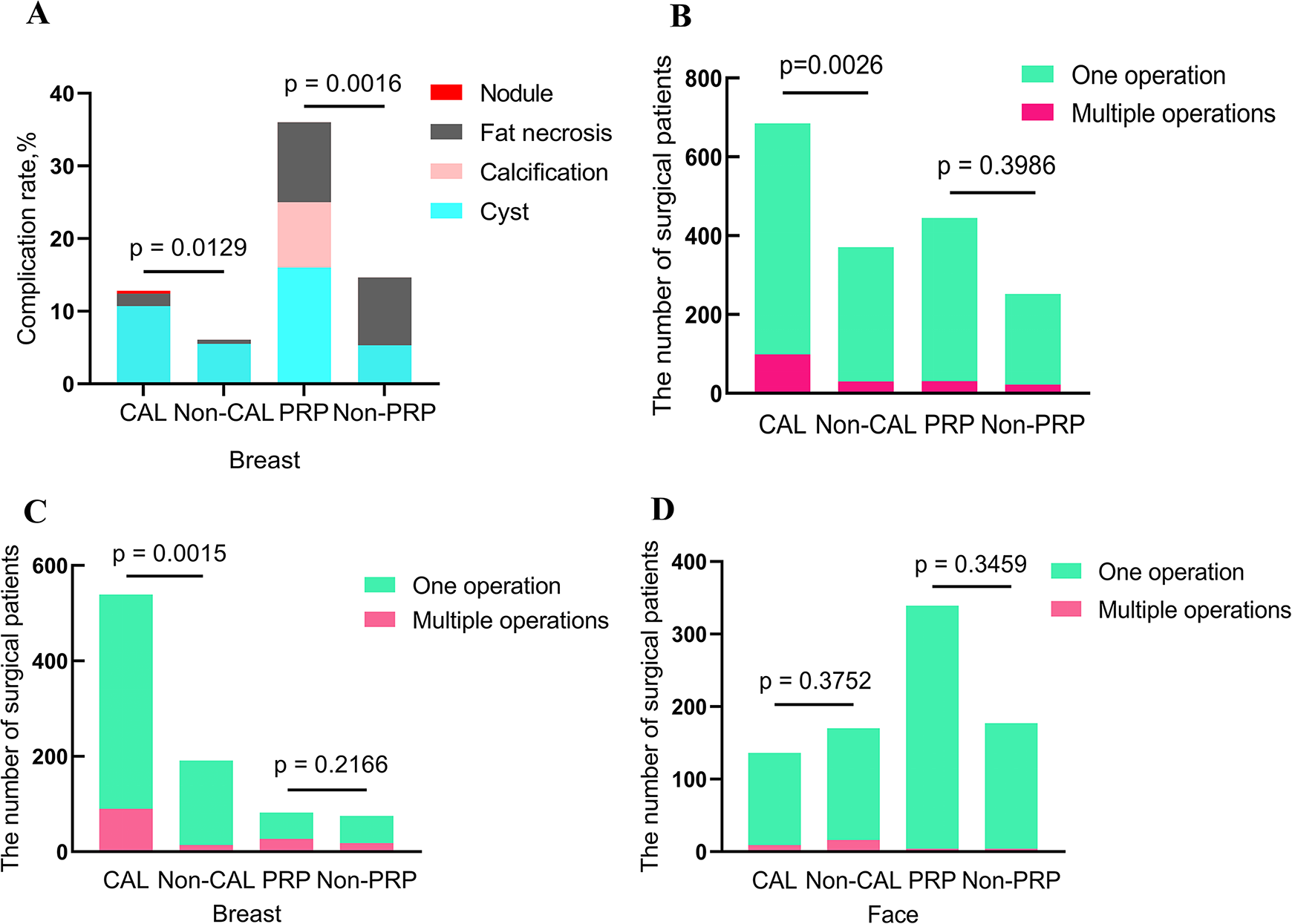
(A) Complication rates of different interventions; (B) All patients were summarized for having complications or not; (C) A summary of all patients undergo facial surgery with single and multiple operations; (D) A summary of all patients undergo breast surgery with single and multiple operations.
Another indicator for safety assessment is the frequency of multiple operations. All the studies in Table 1 were included. For the CAL group and the non-CAL group, both the overall and breast surgery statistics, the incidence of multiple operations of the CAL group was higher than the non-CAL group (the overall: 14.45% [99/685] vs 8.09% [30/371], P = 0.0026; breast: 16.7% [90/539] vs 7.33% [14/191], P = 0.0015), but in terms of the frequency of facial operations, there was no statistical difference between CAL and non-CAL (6.62% [9/136] vs 9.41% [16/170], P = 0.3752) (Fig. 9B–D).
Between the PRP-assisted lipotransfer group and the non-PRP-assisted lipotransfer group, regardless of the overall, face, or breast, there was no statistical difference in the incidence of multiple operations (the overall: 6.97% [31/445] vs 8.73% [22/252], P = 0.3986; breast: 32.93% [27/82] vs 24% [18/75], P = 0.2166; face: 1.18% [4/339] vs 2.26% [4/177], P = 0.3459;) (Fig. 9B–D).
We also compared the relationship between manual and automatic separation of SVF and the incidence of multiple operations, and found no significant correlation between the two interventions (12.93% [30/232] vs 10.33% [38/368], P = 0.3270).
Publication Bias
The funnel charts (Fig. 10) show that the four groups of CAL, non-CAL, PRP-assisted lipotransfer, and non-PRP-assisted lipotransfer have no published bias intuitively.
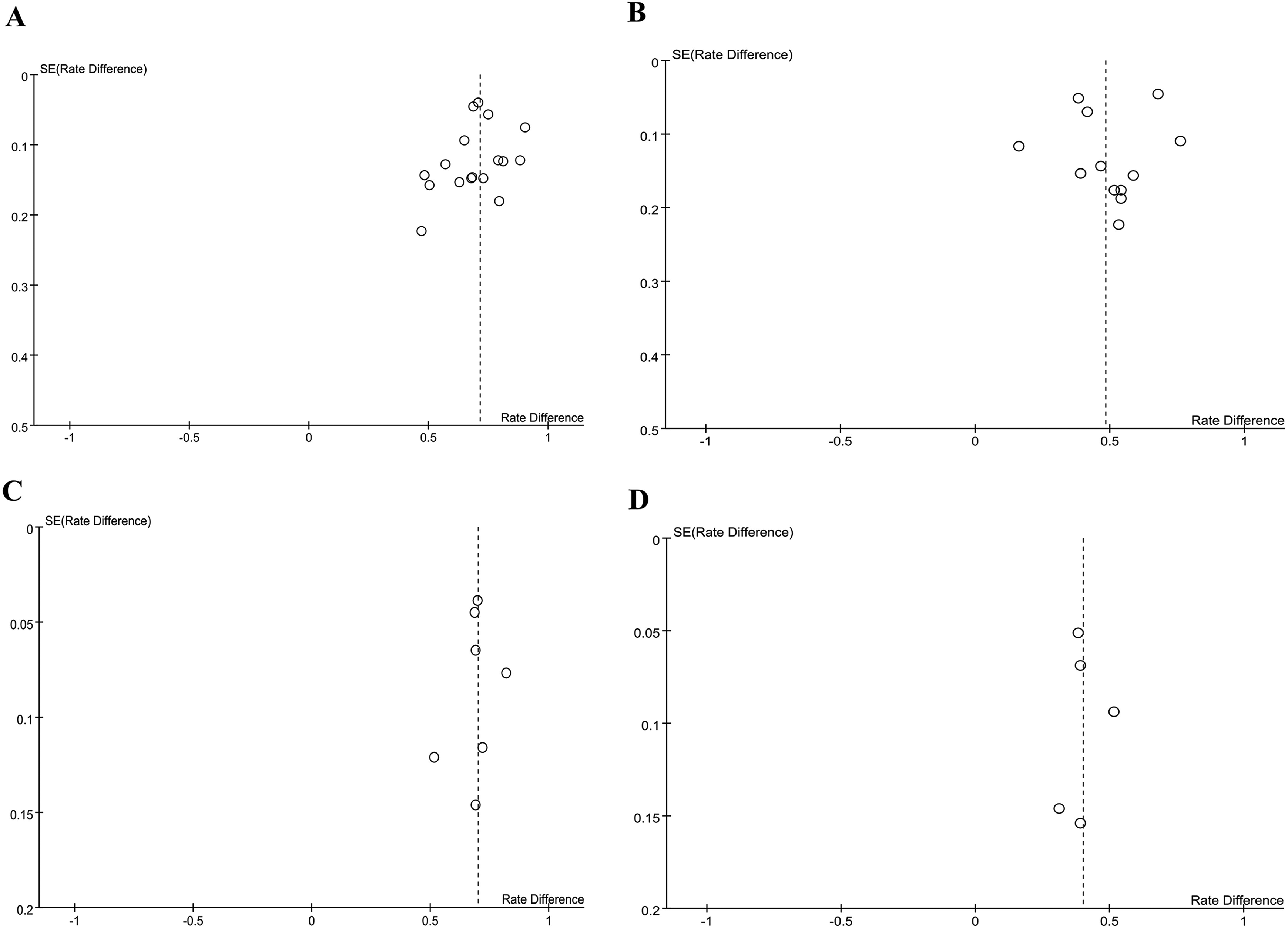
Funnel plot analysis of publication bias for studies on (A) CAL; (B) non-CAL; (C) PRP; (D) non-PRP.
Discussion
With the development of autologous fat grafting technology, researchers tried to find a way to maximize the survival of grafted fat and ensure its safety. In the past 10 years, we can see that cell-assisted fat grafting and the addition of active ingredients from the blood have become the two methods that were recognized by experts in the industry most, and related research articles have also appeared continuously. Most studies indicate that both can promote the survival of grafted fat to a certain extent, but there are a few articles think that both have not improved the survival rate 4,29,36,39,49,52 , and may even increase the incidence of complications 40,43 . Therefore, we conducted a meta-analysis to determine the efficacy and safety of CAL and PRP-assisted lipotransfer compared to traditional fat grafting.
Meta-Analysis Outcomes
The results of the cell-assisted and PRP-assisted lipotransfer studies indicate that regardless of the location of the recipient areas, both cell-assisted and PRP-assisted lipotransfer can increase the survival rate of grafted fat, and there is no difference in the degree of survival rate between the two (Fig. 4). However, both increased the incidence rate of complications in the recipient area. And we found that all complications only occurred in the breast, and no related complications occurred on the face (Fig. 9A). Therefore, we think that one of the main reasons is that the volume of grafted fat leads to complications. According to Yoshimura “three-zone theory” 53 , the evolution of the fat from the edge to the center after grafting, respectively were: survival zone (fat cells survived), regeneration zone (fat cells died, adipose stromal cells survived and dead fat cells were replaced by new ones), and necrotic zone (both fat cells and adipose stromal cells died). The breast surgery requires a larger graft volume than facial surgery, so ischemic necrosis and reabsorption are more likely to occur in the center of breast grafts, which can lead to calcification, oil cysts, and masses 54 . The current cell-assisted and PRP-assisted lipotransfer technology is not enough to reverse the ischemic state and cannot reduce the complications of fat grafting in breast surgery. In addition, it can be seen from the study of Fiaschetti et al. 45 that different detection methods (mammography, ultrasound, MRI, etc.) have significant differences in the detection rate of complications. Ultrasound had a higher detection rate of cysts than mammography and MRI, and the detection rate of mammography for calcification was higher than that of ultrasound. However, the objective detection methods for postoperative follow-up in most literatures mainly focus on the final fat volume, so MRI, 3D scanning were more used, while ignoring its impact on the rate of missed diagnosis of complications.
Our original conjecture was that after CAL and PRP-assisted lipotransfer, it should reduce the occurrence of multiple operations, thereby reducing the cost of multiple treatments. However, the study found that there was no difference in the incidence of multiple operations between PRP-assisted lipotransfer and non-PRP-assisted lipotransfer. In addition, in breast surgery, the incidence of multiple operations for CAL is actually higher than non-CAL. Analyzing specific data sources, we believe that this result is mainly due to the difference in the number of samples in the CAL group and the non-CAL group. For example, In the study of Gentile 33 , all cases were performed twice, but there were 40 cases in the CAL group, while the number in the control group was only 10. In Chiu’s study 40 , CAL group has a higher rate of multiple operations (19.8% vs 3.8%), which was explained that the overall economic situation of the CAL group is better and can bear the cost of the second operation. In addition, the perez-cano study 25 did not set a control, and the rate of patients undergoing secondary surgery reached 35.8% (24/67), which seriously affected the actual results of this index. After excluding these three studies, it was found that there was no difference in the incidence of multiple surgeries between the CAL group and the non-CAL group (1.85% [6/325] vs 0% [0/76], P = 0.5997).
Our results indicated that the SVF separation method (mainly referring to automatic separation and manual separation) does not affect the fat survival rate (Fig. 8), which is consistent with Doi 27 and Laloze, J 55 . It showed that the automatic separation system is a reliable method, and it is expected that clinical trials based on enzymatically hydrolyzed fat particles will be carried out directly in small, sterile facilities without the need for advanced cell laboratories. In addition, non-enzymatic mechanical separation of SVF and in vitro cultured ADSCs seemed to be a good choice to improve the survival of grafted fat. According to the included articles 2,23,38,42 , fat survival rates of adding with non-enzymatic mechanical separation of SVF and in vitro cultured ADSCs were higher than the average level of SVF in automatic and manual separation. No complications were observed and only underwent a single operation. Studies have analyzed the SVF obtained by enzymatic and non-enzymatic treatment, and found that they have similar cell yield, cell survival rate, and SVF composition, The non-enzymatic method consumes less time and lower cost than the enzymatic method, which is more suitable for clinical application 56,57 . However, only a small sample size was used to confirm this processing technique. In this sense, we hope to further evaluate the clinical safety of this processing technology. If the outcome is good, we will not need to use enzymatic hydrolysis or in vitro amplified stem cells. And the non-enzymatic technology will greatly facilitate the implementation of such surgery, improve the survival of grafted fat and reduce the cost of the operation.
Which One Is Better, Cell-Assisted or PRP-Assisted Lipotransfer?
In order to better promote the development of clinical autologous fat grafting surgery, improve its survival rate, reduce its complications and the number of multiple operations. We tried to analyze related articles containing CAL and PRP-assisted lipotransfer for more accurately apply related assisted fat grafting technology in the future.
Many studies have confirmed that traditional autologous fat grafting is safe for breast reconstruction after breast cancer surgery 58,59 , but adipose-derived stem cells have been shown to promote cancer progression in pre-clinical studies 60,61 . Which has caused concern about the safety of cell-assisted fat grafting in breast reconstruction after breast cancer surgery. Most recently Simon Gebremeskel et al. 62 observed that simple adipose-derived stem cells can promote the proliferation and invasiveness of breast cancer cells in vivo and in vitro, but cell-assisted fat grafting will not promote the development of breast cancer. In this review, only two articles reported breast cancer recurrence after breast reconstruction surgery. In the study of Perez-Cano et al. 25 , there was a patient with pelvic bone metastasis after fat grafting, which was considered to be a natural progression of the disease and had nothing to do with the use of CAL. In the study by Gentile et al. 41 , there was no statistical difference between CAL group and the traditional fat grafting group in terms of local recurrence and systemic recurrence and think that cell-assisted or traditional fat grafting is not a risk factor for recurrence. Therefore, there is currently no definite evidence that performing cell-assisted fat grafting on breast cancer patients will increase the risk of breast cancer recurrence. Instead, more clinical data support that the technology is safe and effective 63,64 .
PRP which is easy to implement, does not affect the total operation time, does not require special laboratory equipment and haven’t side effects been reported, so its role in fat grafting is getting more and more attention 43 . Several articles in the included studies mentioned that PRP-assisted lipotransfer shortened postoperative recovery time 39,47,48,50 , which may be due to the increased amount of PDGFs. These cytokines and growth factors are involved in homing, migration, proliferation and differentiation of various cells. Its highly concentrated growth factors can promote the production of collagen and fibronectin, promote angiogenesis, accelerate wound healing and shorten recovery time 65 .
Based on our meta-analysis results and other data from the 36 studies we included, we recommend to use the CAL techniques in large-volume fat grafting, such as breasts and buttocks fat grafting. Although the forest plot results proved that there was no statistical difference between the CAL and PRP-assisted lipotransfer in promoting the survival of grafted fat, no matter whether it was applied to the large-volume or the small-volume fat grafting, we mainly consider the problem of the excessive volume of autologous whole blood required due to the demand for PRP in large-volume fat grafting. We summarized data from 11 included studies that included the ratio of whole blood to PRP or the ratio of PRP to grafted fat (Appendix 2). In addition, we calculated the average value of the injected fat volume of the unilateral breast in the included breast fat grafting articles, which was 219 ml. It can be seen from Appendix 2 that the ratio of whole blood to PRP or the ratio of PRP to grafted fat was different in different articles. Therefore, the proportional relationship between PRP and grafted fat has led to the need for total blood volume as an issue of concern. We choose a moderate ratio from Appendix 2, assuming that the ratios of whole blood to PRP and PRP to grafted fat are 10:1 and 1:5, respectively, and which is the most appropriate ratio. For a patient who wants a breast filling, supposing 200 ml of fat is needed for one-side and 400 ml for both sides. Then 80 ml of PRP would be required. Which means it is necessary to draw 800 ml of whole blood 34,44,49 . This will limit the application of PRP in fat grafting because it will pose a threat to the health of patients. For small-volume fat grafting areas such as face and arm (grafted fat volume <100 ml), we recommend to use PRP-assisted lipotransfer technology. Because based on the above ratio, the amount of whole blood we need will not exceed 200 ml. Furthermore, CAL consumes longer operation time than PRP because SVF requires enzymatic separation or mechanical separation. In addition, compared to SVF, PRP has the advantages of low operational difficulty, short operation time and postoperative recovery time 39,47,48,50,65 . So PRP is superior to SVF in small volume fat grafting.
Limitation
Our study has the following limitations: First, the objective measurement methods for postoperative volume measurement and follow-up of complications were not thorough. Although some studies have confirmed that there was no difference among different objective measurement methods for measuring fat volume 32,66 , the fat volume retention rate obtained by palpation, comparison with immediate postoperative photos and follow-up photos were somewhat subjective 47 . And different objective measurement methods have differences in the detection rate of complications 45 . Therefore, it is hoped that in the future, the objective measurement methods related to the measurement of fat survival volume and the detection of complications will be unified as much as possible, so as to make different studies more comparable. Second, the optimal concentration of enriched SVF cells/ADSCs and PRP in improving the survival of grafted fat cannot be obtained. Because the preparation equipment and methods used in different studies are not uniform, and the information provided is insufficient. So it is hard to compare each other between different studies. Therefore, in order to further improve the research of cell-assisted and PRP-assisted lipotransfer, in the future, we need more complete large samples, objective volume and complication measurement methods, standard and unified preparation equipments and procedures, complete data information recording and follow-up plans in randomized controlled clinical research to further determine the true level of various indicators under clinical conditions and to obtain the optimal use concentration of cell-assisted and PRP-assisted lipotransfer, which have great significance for its conversion into clinical practice.
Conclusions
In this study, we confirmed that both CAL and PRP-assisted lipotransfer can significantly improve the survival rate of grafted fat. But in large-volume fat grafting, such as breast reconstruction, both increased the incidence of complications to a certain extent. We recommend to use CAL for breasts, buttocks and other parts that require large-volume fat grafting, and PRP-assisted lipotransfer for parts that require small-volume fat grafting such as face and arm. Finally, the optimal concentration of SVF/ADSCs and PRP is still a very important and urgent issue. Future studies should address these issues through high-quality multicenter randomized controlled clinical studies and use objective measurements to evaluate the results.
Supplemental Material
Supplemental Material, sj-pdf-1-cll-10.1177_0963689721989607 - Comparison of the Efficacy and Safety of Cell-Assisted Lipotransfer and Platelet-Rich Plasma Assisted Lipotransfer: What Should We Expect from a Systematic Review with Meta-Analysis?
Supplemental Material, sj-pdf-1-cll-10.1177_0963689721989607 for Comparison of the Efficacy and Safety of Cell-Assisted Lipotransfer and Platelet-Rich Plasma Assisted Lipotransfer: What Should We Expect from a Systematic Review with Meta-Analysis? by Aizhen Chen, Li Zhang, Penghong Chen, Chaoyu Zhang, Shijie Tang and Xiaosong Chen in Cell Transplantation
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (Grant number 81671930 and 81971855); the Special financial funds of Fujian Province (Grant number 2018B054); the Industrial technology Joint Innovation Project of Fujian Development and Reform Commission (Grant number 2011601); and the Science and Technology Innovation Joint Fund project (Grant number 2017Y9101).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.