
Abstract
Hematopoietic stem cell transplant (HSCT) is the only cure for patients with sickle cell disease (SCD). Although most SCD patients experience progressive end-organ damage and shortened lifespans, not all patients follow the same disease course, tempo, or outcome. Therefore, the dilemma facing physicians is weighing the selection of patients and timing for the procedure against donor type and transplant-related mortality and morbidity that go up with increasing age. On the other hand, the dilemma facing the patients and families is how acceptable HSCT that carries some mortality risks to them. We have analyzed the chronic conditions due to SCD in 449 patients to determine whether SCD-related multiple chronic conditions (MCC) can be risk-stratified to identify the group of patients predicted to not only have shortened lifespans but also functional limitation and poor quality of life so that these at-risk patients can be offered HSCT early and before MCC develops. We identified that the age of onset of the first SCD-related chronic conditions strongly predicted for the risks for disease-related MCC. SCD patients who suffered their first disease-related chronic condition before age 30 years developed MCC at a rate of 19.1 times faster than those at a later age. These patients are therefore high-risk patients and should be offered HSCT early in the course of their disease before multiple organ damage intervenes, even if matched-related donors are not available. This patient selection and timing approach provides a forum for an easy-to-understand and real-time discussion, including the choice of donor type, with SCD patients and families when considering HSCT.
Introduction
Sickle cell disease (SCD) affects millions of people worldwide. Approximately 300,000 babies are born each year with the disease 1 . SCD individuals suffer multiple chronic conditions (MCC) and severe health disparities. Recurrent vaso-occlusive crisis (VOC) causes chronic disabling arthritis due to osteonecrosis, progressive retinopathy, chronic kidney failure, strokes, and shortened lifespan. The National Center for Health Statistics multiple-cause-of-death databases reported that in 2005 in the United States, the median life expectancy of SCD subjects was only 42 years for females and 38 years for males 2 , compared to 77 years for females and 72 years for males in the general U.S. population 3 . Although only 100,000 Americans are affected by SCD 4 , they impose high healthcare utilization 5 . A benchmark study reported a mean annual rate of 1.52 admissions per SCD patients and 1.08 treat-and-release Emergency Department visits per year 6 . Notably, the highest utilization was observed in the 18 to 30-year-old group. In 2004, more than 80,000 hospitalizations were incurred by adult SCD patients in the United States, costing nearly $500 million 6 . SCD is, therefore, a major public health concern.
Due to MCC, SCD patients experience declining health and quality of life. The unpredictability and frequency of painful crisis contributes to the high unemployment rate among SCD patients 7 . This further impacts financial instability that amplifies health disparities.
Allogeneic hematopoietic stem cell transplant (HSCT) remains the only cure available for SCD. It restores normal hematopoiesis and potentially reverses or halts some of the organ damage induced by the disease 8 –10 . However, the biggest challenge facing HSCT in SCD is the timing and selection of patients for the procedure and weighing the risks associated with HSCT based on donor type. HSCT should ideally be performed early before the occurrence of multiple organ damage that would increase transplant-related mortality (TRM) 11 . Various predictors have also been used to identify patients at risks for early deaths due to SCD 12 –18 and outcomes from HSCT 19,20 .
MCC is associated with functional limitation, poor quality of life, and shortened lifespans 21 –23 . The benefits of avoiding the development of MCC should, therefore, be weighed when considering SCD patients for HSCT. In this study, we sought to investigate the risks for chronic conditions due to SCD and determine whether MCC can be risk-stratified to identify the group of patients who should undergo HSCT early in their disease course, before the development of multiple organ damage.
Patients and Methods
Data Collection
A cross-sectional retrospective chart review survey was performed on patients with the ICD diagnosis code of sickle cell disease (D57) seen at the State University of New York Downstate Medical Center and Kings County Medical Center in Brooklyn, New York. Patient demographics, clinical data, diagnosis, and treatment history were collected. The study received exemption from the Institutional Review Board of State University of New York Downstate Health Sciences University, Brooklyn, New York.
Definition
MCC was defined as the co-occurrence of two or more chronic health conditions. The following were included as SCD-related chronic conditions: chronic kidney disease (defined as at least Stage 3 chronic kidney disease), stroke (defined as a neurologic deficit lasting more than 24 hours, with or without residual abnormalities), retinopathy, chronic arthritis due to osteonecrosis, chronic liver disease (defined as a persistently elevated transaminases), chronic leg ulcers, pulmonary hypertension (either symptomatic or detected by flow studies in echocardiography), and psychiatric illnesses needing chronic medications. These chronic conditions were included for analysis since many of them are part of the Hematopoietic Cell Transplantation-specific Comorbidity Index (HCT-CI) 11 . Furthermore, their occurrence influences functional limitation that affects the quality of life of the patients, as reported by most SCD patients. Chronic conditions were diagnosed by individual subspecialists seen by the patients.
Statistical Analysis
Chi-square test was used to analyze for statistical significance in two comparator groups. The cumulative risk for any particular SCD-related complication was plotted as a time-dependent covariate with 95% Confidence Intervals using the Kaplan-Meier method. Hazard ratios were calculated using the log-rank tests. A two-sided P-value of <0.05 was considered statistically significant.
Results
Patient Characteristics
Medical records from 481 patients who carried the ICD code, D57, were retrieved. After screening, data from only 449 SCD patients were included for analysis. Thirty-two patients were dropped from the analysis because their diagnoses were erroneously coded; they had sickle cell trait (HbAS), HbC disease, or alpha thalassemia. Among the 449 SCD patients included in the study 258 were females and 191 males; and 98% were Blacks. Their median age was 39 years (range 3–88). Forty-seven patients (10.5%) were over 60 years, 14 over 70 years and two over 80 years old. Ninety-three percent of the females and 91% of the males were over 18 years or older. Their phenotypes were: HbSS (284/449) (63%), HbSC (101/449) (22.5%), HbSβ0thal (54/449) (12%), and unknown or other (10/449). Only 34% (151/449) of the patients were taking hydroxyurea.
Probability of Developing SCD-Related Chronic Conditions
We first examined the risks for developing the eight individual chronic conditions associated with SCD. Fig. 1 shows the probability at a particular age for developing a specific chronic condition. As a group, the two most common chronic conditions affecting these patients were retinopathy and chronic arthritis, followed closely by chronic kidney disease and psychiatric illnesses. The risks for developing pulmonary hypertension, stroke, and chronic leg ulcers came next, and the risk for chronic liver disease was the lowest. Since this is not a prospective analysis, the effects of hydroxyurea on these risks could not be determined.
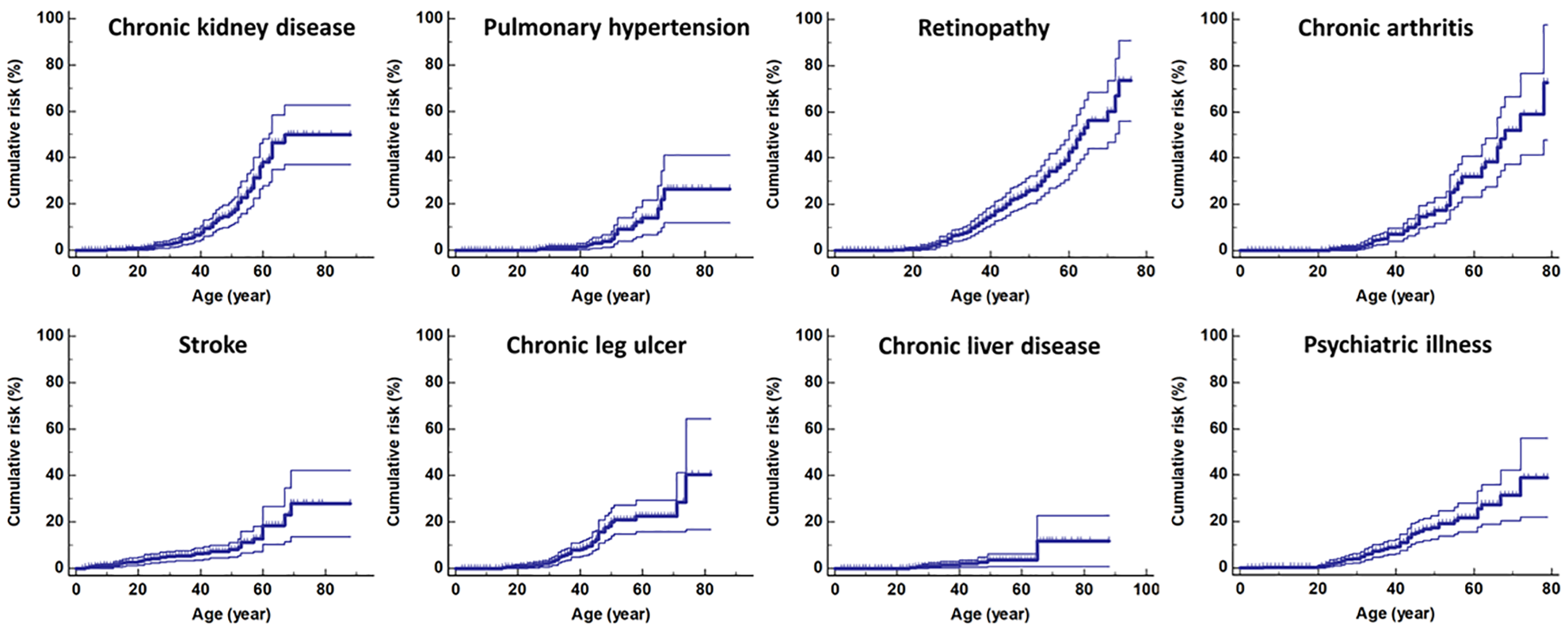
Predicted cumulative risks (+/- 95% CI) over the lifetime of patients for the development of sickle cell disease-related chronic kidney failure, pulmonary hypertension, retinopathy, chronic arthritis, stroke, chronic leg ulcer, chronic liver disease, and psychiatric illness. The cumulative risks were highest for chronic arthritis and retinopathy but lowest for chronic liver disease.
The risk for stroke started as early as age 10 years and plateaued off at age 70 years. Likelihood of developing psychiatric illnesses, mostly depression, started at approximately age 20 years, whereas development of chronic kidney disease, retinopathy, chronic arthritis, and chronic leg ulcers increased progressively a decade later. Pulmonary hypertension tended to complicate the disease in the 5th decade of life, and for chronic liver disease, late in life. The cumulative risks for retinopathy and chronic arthritis were more than 70%, chronic kidney disease nearly 50%, chronic leg ulcers and psychiatric illnesses almost 40%, and stroke and pulmonary hypertension over 25%.
We next investigated whether disease genotype affects the risks for SCD-related chronic conditions by comparing HbSC with HbSS and HbSβ0thal. To do so, only the data from 439 patients with known genotype were included (
Clinical Characteristics of Patients.
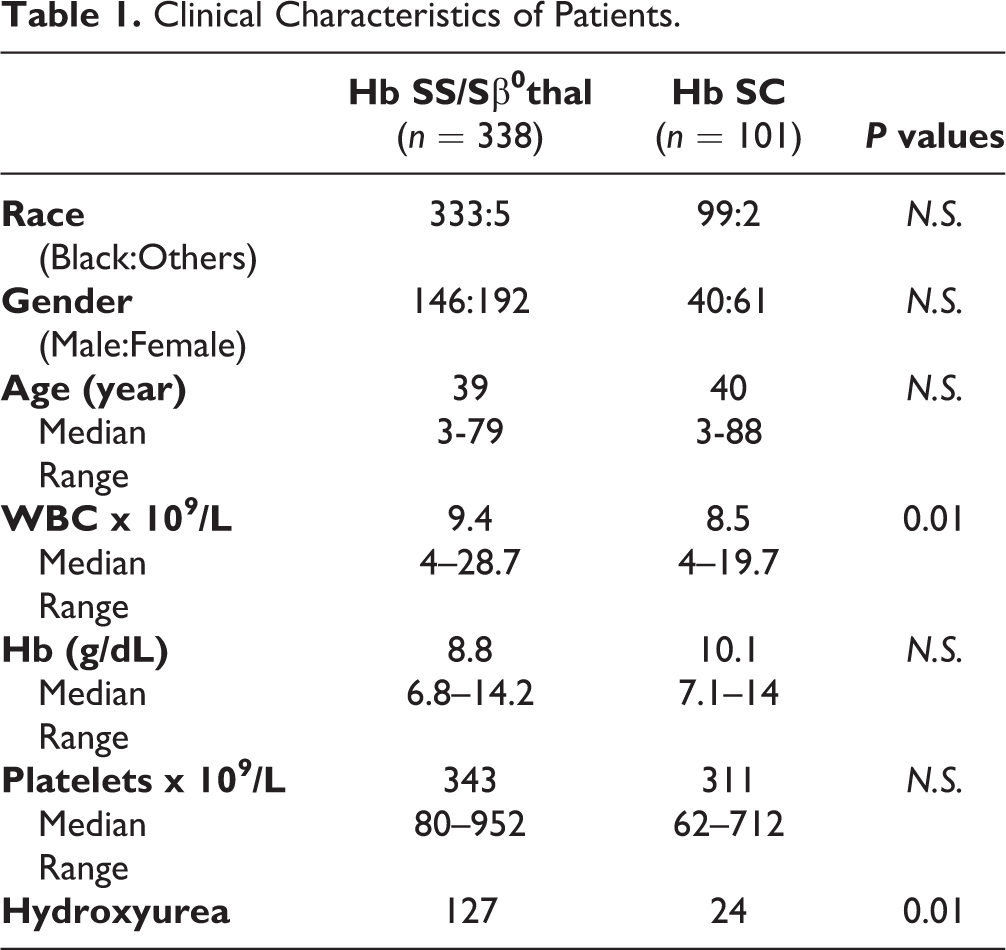
Fig. 2 shows the hazard ratios of HbSC to HbSS and HbSβ0thal for each of the individual disease-related chronic conditions. In keeping with previous reports 24,25 , compared to those with HbSS and HbSβ0thal, patients with HbSC were more likely to develop retinopathy (P < 0.0001). However, their risks for chronic kidney disease (P = 0.014), pulmonary hypertension (P = 0.0075) and chronic leg ulcers (P = 0.001) were lower.
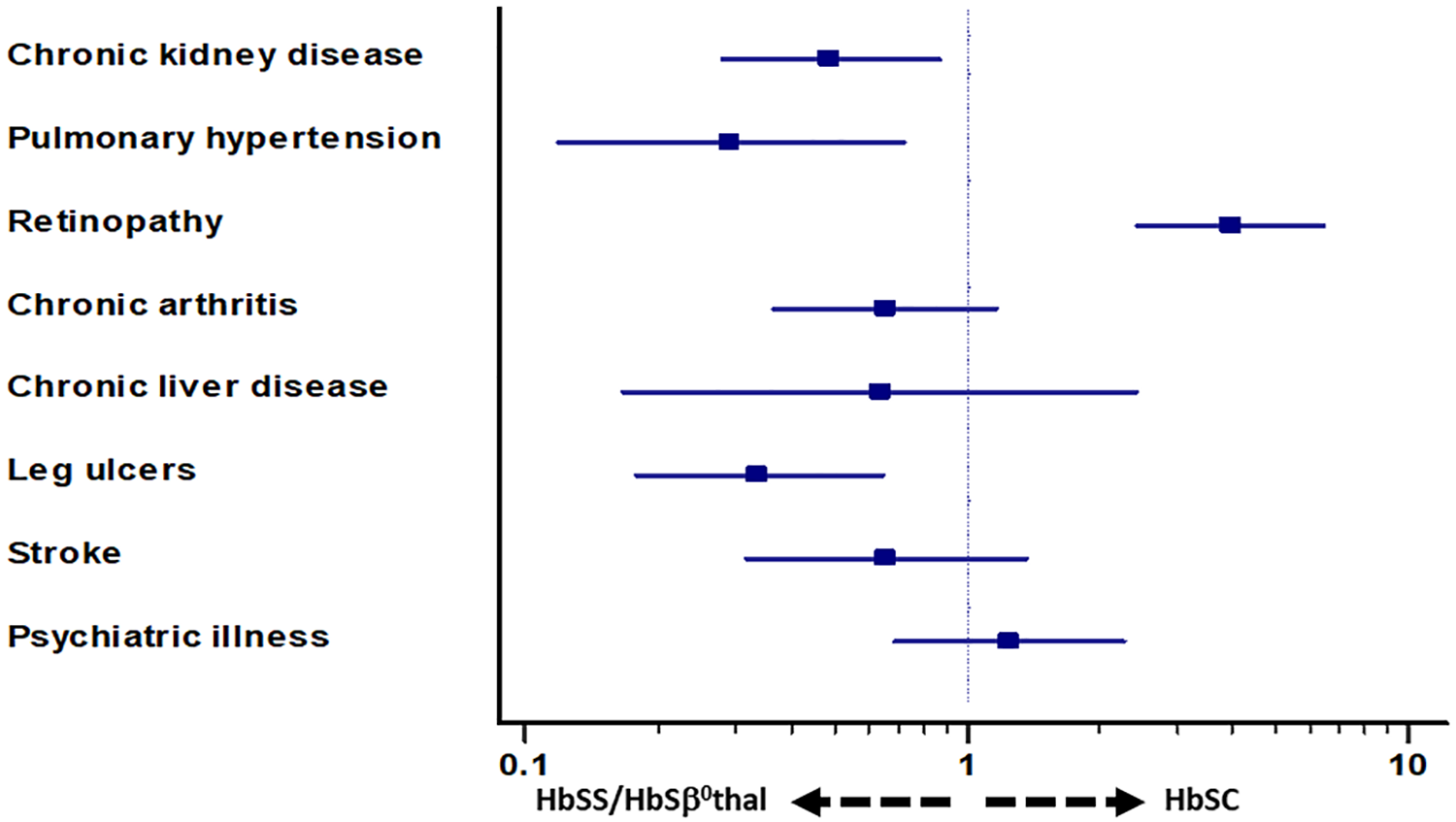
Hazard ratios comparing the risks for patients with HbSC to those with HbSS or HbSβ0thal for the development of the eight disease-related chronic conditions. HbSC patients were at higher risks for the development of retinopathy, but lower risks for chronic kidney disease, pulmonary hypertension, and chronic leg ulcers.
Risks for Disease-Related MCC
SCD-related MCC is prevalent among this cohort of patients (Fig. 3). As a group, the probability of developing at least two disease-related chronic conditions was almost 80%, three or more disease-related chronic conditions almost 60% and four or more disease-related chronic conditions at approximately 45% by the age of 75 years. Interestingly, despite lower risks for three of the eight SCD-related chronic conditions, the likelihood for developing disease-related MCC was not any lower in patients with HbSC than those with HbSS and HbSβ0thal. Multivariate analysis of the clinical characteristics listed in Table 1 did not identify specific parameters between the two groups of patients in their likelihood to develop MCC. The hazard ratio for developing two or more disease-related chronic conditions was 0.732 (95% CI: 0.4899–1.0931) (N.S.), three or more was 0.7192 (95% CI: 0.3929–1.3165) (N.S.), and four or more was 0.6641 (95% CI: 0.2587–1.7051) (N.S.).
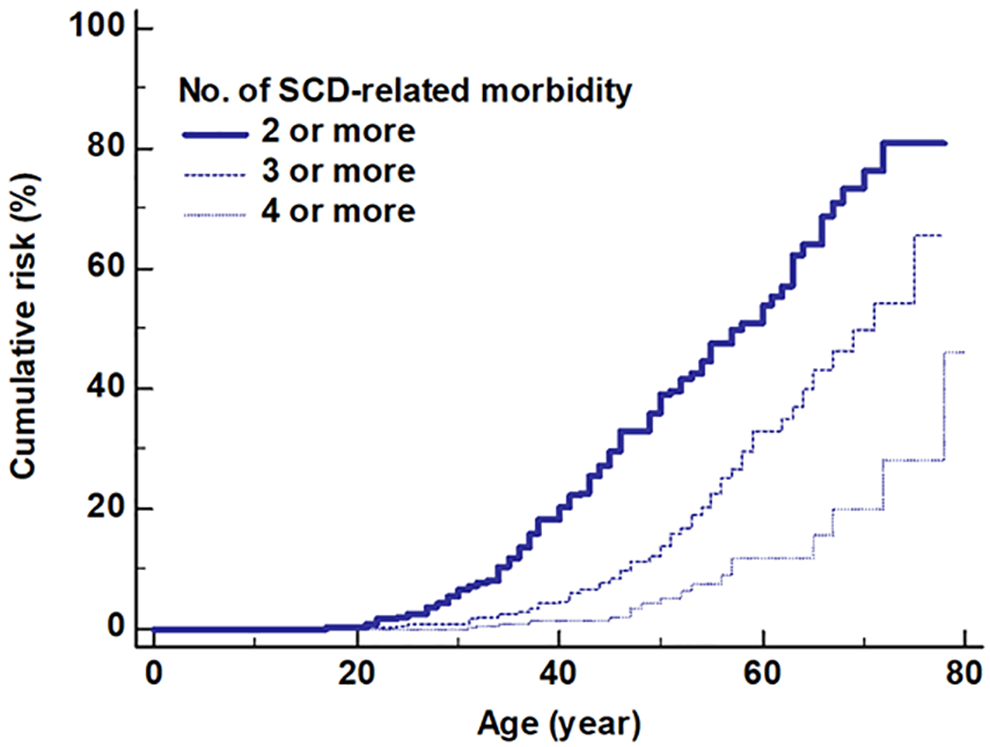
Predicted cumulative risks over the lifetime of the patients for the development of SCD-MCC. The risks for MCC increase with age.
Prevalence of Disease-Related MCC in Relation to Age of Patients
The prevalence of disease-related MCC among this cohort of patients in relation to their age was examined. We observed a progressive increase in the risks for SCD-related MCC (Fig. 4). By the age of 20 years or older, 28.6% (95% CI: 23.6–34.5) of SCD patients suffered at least two disease-related chronic morbidities. The prevalence increased to 40.7% (95% CI: 32.7–50.2) (P = 0.01) by age 40 years or above, and 55% (95% CI: 36.1–81.1) by age 60 years or above (P = 0.002). The increases observed between age 20 years and above and age 30 years and above, and between age 40 years and above and age 60 years and above were not statistically significant. By age 60 years or above, 55% of SCD patients were inflicted with at least two disease-related chronic conditions, 36% from at least three, and 17% from four or more disease-related MCC (Fig. 5).
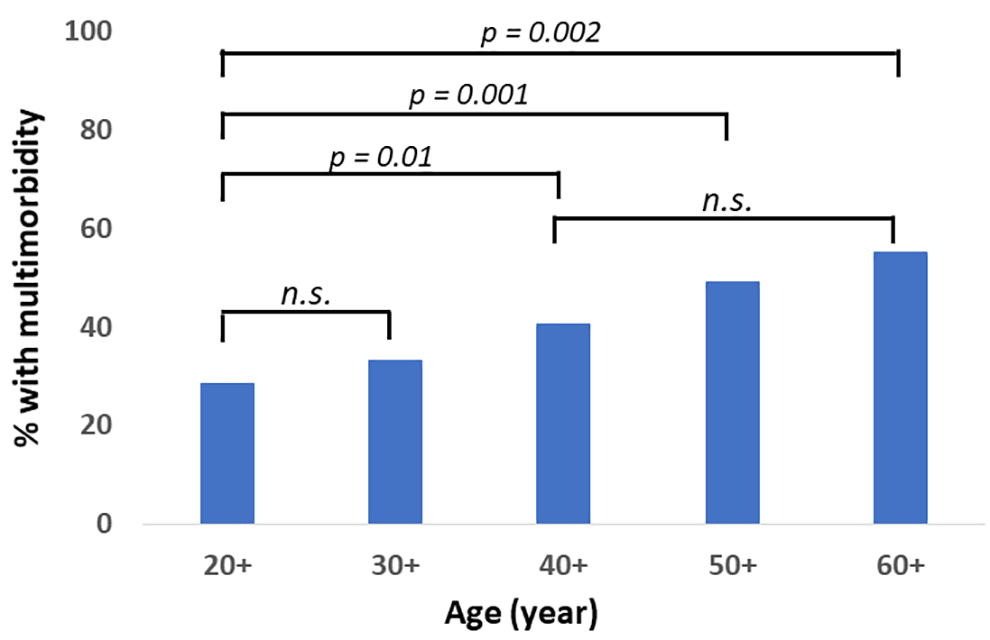
Prevalence of MCC at different age groups.
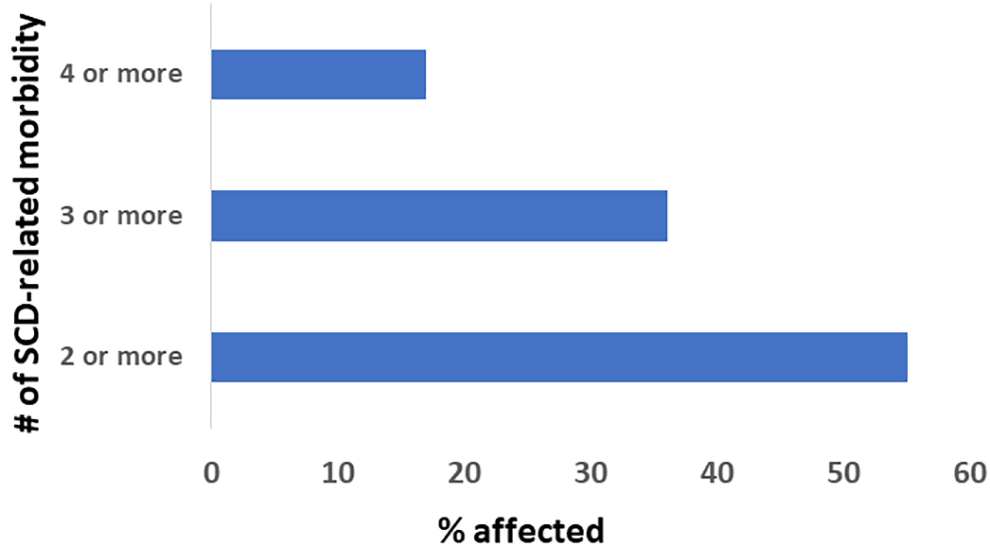
Proportions of SCD patients with two or more, three or more, or four or more disease-related morbidities by the age of 60 years.
Risks for Disease-Related MCC in Relation to First SCD-Related Chronic Complication
We next investigated the risk for developing SCD-related MCC after the patient was affected by a SCD chronic condition. The risk for developing another SCD-related morbidity was high once a patient is affected by one disease-related chronic condition (Fig. 6a). For those who developed one disease-related chronic complication before the age of 50 years, the probability of being affected by SCD-related MCC was nearly 50%.
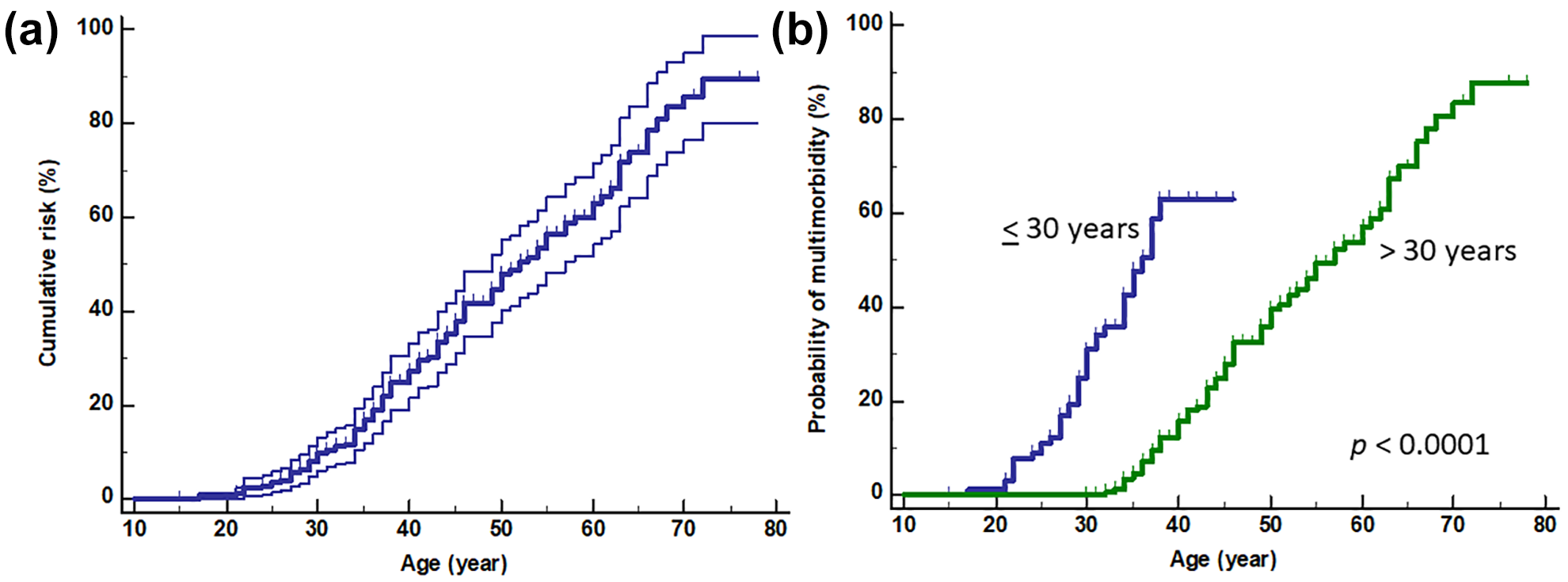
Development of MCC after the first disease-related chronic complications. a). The predicted cumulative risks (+/− 95% CI) for the whole group of SCD patients. b). Probability of developing disease-related MCC was significantly higher in those who developed the first chronic conditions before the age of 30 years.
Age of the first SCD-related chronic condition also predicted for the time of onset of disease-related MCC (Fig. 6b). The age to disease-related MCC was significantly younger (P < 0.0001) if the first SCD-related morbidity occurred at age 30 years or younger than if it occurred later. The hazard ratio for developing disease-related MCC is 19.1 (95% CI: 9.85–37.26) (P < 0.0001).
Discussion
Patients with SCD are particularly at risks for MCC. SCD is associated with chronic inflammation triggered by factors such as activation of neutrophils, macrophages and platelets, chemokines, and reactive oxygen species, that affect multiple organs. The progressive increase in inflammation due to recurrent VOC drives MCC. Thus, in addition to sharing the risks factors of the general population, SCD causes its own distinct disease-related chronic conditions. These compounding effects may explain why the life expectancy of adult SCD patients in this country has not increased in the last two decades 2 . Accordingly, HSCT is an appropriate therapeutic approach for SCD patients. Although it is the only cure currently available, not all SCD patients need HSCT. As highlighted in our data, some SCD patients live into their eighth or ninth decade of life. More than 10% of the patients in our cohort were more than 60 years old.
A number of models have been used to predict the risk of death in SCD patients 12 –18 and so have been proposed for use when discussing HSCT to SCD patients and families. However, they only provide the estimated mortality due to SCD in the near-term, between 2-5 years. Yet, these rates increase over time as multiple organ damage occurs. Unlike patients with hematologic malignancies who personally experience near-death situations at the time of diagnosis and, hence, are most likely to appreciate and accept the potential benefits of HSCT, SCD patients may be less motivated to do so. This may explain the low uptake of the procedure, even in the pediatric setting. This is especially the case if the patients have only been afflicted primarily by acute events such as painful crisis that ultimately resolve. How applicable HSCT is to SCD patients may, therefore, depend on the balance between the physician being able to transplant the patients safely prior to the occurrence of multiple organ damage and the patients being able to accept that they need the procedure based on their experience during their disease course.
We have chosen to examine SCD-related MCC as a potential method for patient selection for HSCT by the physicians and likelihood to accept the procedure by the patients before multiple organ damage occurs to address the common dilemma faced by patients, families, and physicians. We argue that MCC is an appropriate benchmark to use for patient selection since MCC affects not only life expectancy but also functionality of the patients. Therefore, SCD patients who experience MCC are more likely to die at a younger age and with poorer quality of life compared to their peers. The disease-related chronic conditions we have included in our analysis not only overlap with some of the parameters in HCT-CI but also impact functionality of the patients.
We found in this current study that MCC induced by SCD is prevalent, with more than one quarter of the patient population being affected by the age of 20 years and above. This is in keeping with our findings previously that although a high proportion of adult SCD patients fulfilled the entry criteria for the three large multicenter studies (https://Clinicaltrials.gov Identifiers: NCT01565616, NCT02766465, and NCT03263559) of HSCT for SCD 7 , the majority of the patients had high HCT-CI, predicting for high 2-year TRM 11 . The data underscore the need to identify the patients most at risks for MCC before they develop high HCT-CI scores to reduce the TRM.
We did not find any difference in the probability of developing disease-related MCC between patients with HbSC disease and those with HbSS or HbSβ0thal despite lower risks for the development of chronic kidney disease, chronic leg ulcers and pulmonary hypertension in patients with HbSC disease, suggesting that HSCT may be an appropriate therapeutic option for patients of either disease genotype as long as they are at high risks for MCC. Not surprisingly, disease-related MCC is significantly more prevalent in SCD patients as they get older so that at age 60 years or above, disease-related MCC is twice as common as when they were 20 years old. This group of patients are, therefore, clearly not the best candidates for HSCT due not only to their age but also to the presence of multiple organ damage.
In conclusion, despite the shortfalls of a cross-sectional retrospective study, our data identifies a distinct group of SCD patients who are particularly at high-risks for developing MCC early in their disease course. The data, however, would be much strengthened with a validation cohort of patients in future. Nevertheless, based on the results of this retrospective study, we have proposed the inclusion of risks for the development of MCC when discussing HSCT with SCD patients. SCD-related MCC is common among these patients. MCC impacts quality of life and shortens lifespan. The decision to propose HSCT after the occurrence of the first SCD-related chronic conditions, especially if this occurs before age 30 years, and before MCC develops may render the procedure more acceptable to the patients and families, than if HSCT is offered when the patients have not experienced any chronic symptoms. To avoid the development of disease-related MCC, patients who develop the first SCD-related chronic conditions before the age of 30 should be priority candidates for HSCT early in the course of their disease and before multiple organ damage occurs. In these patients, the use of higher-risk donors such as unrelated donors, mismatched donors, and umbilical cord blood may be justifiable.
Footnotes
Ethical Approval
This study was considered minimal risks and was given exemption by the Institutional Review Board of State University of New York Downstate Health Sciences University in Brooklyn, New York, United States of America.
Statement of Human and Animal Rights
All the data was collected in accordance with the Institutional Review Board guidelines of State University of New York Downstate Health Sciences University, Brooklyn, New York.
Statement of Informed Consent
This study was considered minimal risks by the Institutional Review Board and so informed consent was not required.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.