
Abstract
Radiation enteritis is the most common and serious complication of abdominal or pelvic radiation therapy. Mesenchymal stem cells (MSCs), as well as cell protection agents, inhibit apoptosis and promote the proliferation of injured tissues. 3 human umbilical cords MSCs (UCMSCs) were injected into the tail vein or peritoneal cavity of a rat model of radiation enteritis. The temporary protective effect was assessed by identification of donor cells, detection of cellular immune parameters and inflammatory cytokine levels, quantitation of jejunum mucosal preservation and examination of the rat remaining life. Only the rats in the intraperitoneal injection group exhibited a few positive donor cells 7 days after transplantation. CD4 +/CD8 + T cells, a cellular immune parameter, decreased in the abdominal exudate of intraperitoneal injection group, compared with the model-only control and tail vein groups (both P < .05). Both serum and abdominal exudate TNF-α and IL-6 levels in the intraperitoneally injected rats rapidly decreased and were significantly different from those in the model-only control and tail vein injection groups (all P < .05). Mucosal surface area and survival time increased in the intraperitoneal injection group compared with the vehicle and tail vein injection groups (all P = .000). Therefore, the administration of UCMSCs with intraperitoneal injection approach postponed death in a rat model of radiation enteritis, which was associated with reduced serum levels of proinflammatory cytokines (TNF-α, IL-6). However, UCMSCs injected via the tail vein triggered an intense cellular immune response in the serum that adversely affects their survival. This treatment failed to suppress circulating serum and abdominal exudate levels of TNF-α and IL-6 and could not provide a therapeutic benefit for prolonging life against acute radiation enteritis.
Introduction
Radiotherapy in cancers is being used with increasing frequency 1 . The intestinal mucosa is very sensitive to ionizing radiation. The small intestine is the most vulnerable abdominal organ to radiation 2 . Radiation enteritis is the most common complication of radiotherapy for intraperitoneal or pelvic tumors 3 ; it occurs at a rate of more than 20% 4 , the morbidity is increasing year by year globally 5 .
Based on radiation dosage, exposure time extension and clinical onset, radiation enteritis is classified as acute or chronic. The clinical manifestations are nausea, vomiting and abdominal pain after a patient receives a dose of 800-1000 cGy radiation. If symptoms are evident and persist for 8 weeks, acute radiation enteritis is diagnosed 6 . At present, the treatment of acute radiation enteritis is merely symptomatic 7 . Along with the development, it causes intestinal fibrosis and endarteritis obliterans and leads to high mortality 3,8 . More than 20% of patients who receive pelvic or abdominal radiotherapy will progress to chronic radiation enteritis 5,8,9 . This condition is the most common and troublesome complication of radiotherapy for intraperitoneal and pelvic tumors 3,10 .
Thus, the prevention of acute radiation enteritis is the key for decreasing the morbidity of chronic radiation enteritis.
The therapeutic benefit of MSCs in increasing proliferation or reducing apoptosis to rescue injured organs has been broadly described in vivo 11,12 . MSCs maintain stem cell niches and protect damaged organs directly or indirectly 13 . Clevers et al. showed that MSC treatment-induced partial rescue of intestinal stem cells could be sufficient for recovery of small intestinal integrity 14 . Parekkadan et al. reported that MSCs can retard liver fibrosis development 15 .
We previously showed that a single intraperitoneal injection of multiplacenta-derived cells can effectively improve the survival time of a mouse model with radiation-induced bone marrow damage 16,17 . In this experimental model, we assessed the survival and transient effects of intraperitoneally injected human multiumbilical cord-derived exogenous MSCs without immunosuppressant intervention.
Materials and Methods
All experimental protocols were approved by the Institutional Animal Care and Use Committee for Medical Sciences of Kunming University.
Multiumbilical Cord-Derived UCMSCs
First, a human umbilical cord was collected from a full-term cesarean section donor free of hepatitis B and C viruses, human immunodeficiency virus, Treponema pallidum and other contagious disease histories in accordance with the sterile procurement guidelines in the 920th Hospital of Joint Logistics Support Force of Chinese People’s Liberation Army. Next, Wharton jelly from 3 umbilical cords was mixed together, minced, and filtered with Nutrient Mixture F-12 Media through a 200-eye cell filter. Then, UCMSCs from the filtrate were repeatedly reproduced and isolated by adherent culture and density gradient centrifugation procedures (Ficoll-Paque Premium, 1.073 g/mL). Finally, passage 2 UCMSCs were identified and marked with Hoechst 33258 16 –18 .
Animals
Three hundred female Wistar rats weighing 170-200 grams (40-50 days of age) were equally divided randomly into three groups: the model-only control group (vehicle), the tail vein injection group, and the intraperitoneal injection group. Then, each group was equally divided into two subgroups: detection and lifespan (n = 50). Post-transplantation survival time was only observed in rats in the lifespan subgroup. At the same time, donor cell localization, host cellular immunity state, serum inflammatory cytokine levels and mucosal surface area were assessed in rats in the detection subgroup. All rats were synchronized before any treatment.
Experimental Procedure
Induction of an acute radiation enteritis model
Rats in the 3 experimental groups were subjected to local radiation in the abdominal region at a sublethal dose of 10 Gy (total dose) as we previously described 16–17 . Then, the rats were ready for treatment.
UCMSCs Treatment
Given of our previously published articles related to the dose of injected MSCs and the sublethal effect of radiation, P2 generation UCMSCs in 1 mL of DMEM/F-12 were intraperitoneally injected into Wistar rats of the intraperitoneal injection group at 1 × 106 cells per rat a single time within 4 h after radiation. And so were the rats in the tail vein injection group via the lateral tail vein. First, we locked the rats in a device similar to a large conical centrifuge tube to keep the body immobile, and then, an infant scalp venous needle was used for the injection of 1 mL of cells via the tail vein. The model-only control rats received the same volume of Nutrient Mixture F-12 Media via intraperitoneal injection as a vehicle 16 –18 .
Assessment of the Treatment Response
Donor cell localization, cellular immunity function, exudate and serum inflammatory response and mucosal surface area assessments were performed in the detection subgroup.
Rats in the detection subgroup were initially bled for detection of donor cell engraftment in peripheral blood to trace donor UCMSCs before the death of the rats. Ten milliliters of 0.85% normal saline was used to flush the abdominal cavity three times for every rat in the detection subgroup and exudate fluid sample was collected from the very bottom of the abdomen. Then, the rest of the blood was collected via cardiac puncture. The abdominal exudate fluid and serum were used to measure CD4+/CD8+ T cells and the inflammatory cytokines IL-6 and TNF-α. Finally, the rats were sacrificed, and jejunum specimens were collected and fixed in 10% formaldehyde solution for mucosal surface area quantitation.
Post-transplantation survival time was observed only in the rats in the lifespan subgroup to prevent other detections affecting this assessment.
Donor Cell Engraftment Was Examined in Peripheral Blood Smears
All peripheral blood samples in the detection subgroup were diluted with the same volume of DMEM/F-12 at a proportion of one to one to examine donor cell expressed blue fluorescent. Each sample was smeared on a slide and observed with fluorescence microscopy within a few hours. The image of blue fluorescent protein-positive cells per visual field was acquired at 400× magnification 16–17 .
Measurement of Cellular Immune Parameter
CD4 +/CD8 + T cells are a reliable index to show the functional state of the host cellular immune response. Serum and abdominal exudate fluid CD4 +/CD8 + levels of the three groups were detected after treatment.
Proinflammatory Cytokine Measurement
Rat proinflammatory cytokines such as TNF-α and IL-6 can facilitate epithelial cell apoptosis and inhibit intestinal mucosa repair. Serum and abdominal exudate fluid values of TNF-α and IL-6 were measured with ELISA kits as described previously 19 .
Histological Evaluation with Quantitative Morphometry
The jejunum mucosal surface area was measured with vertical section stereology described by Gundersen in 1986 20,21 .
Statistical Analysis
Data are given as the mean ± standard deviation. Statistical comparisons of variable differences among groups were carried out by one-way ANOVA followed by post hoc LSD, S-N-K, and Dunnett tests for multiple comparisons. Cumulative survival was assessed by a Kaplan–Meier plot and differences were analyzed by the log-rank (Mantel-Cox), Breslow (generalized Wilcoxon) and Tarone-Ware tests. SPSS19 was used for statistical analyses. A P value < .05 was considered statistically significant.
Results
Identification of donor cells
All the rats in the detection subgroup were bled for detection of UCMSCs engraftment, on the 7th day, at the time when some rats were dying.
Only 3 of 50 samples of rats in the intraperitoneal injection group of the detection subgroup exhibited a few positive donor cells in peripheral blood smears at day 7 after transplantation. In contrast, other rats in the detection subgroup did not reveal any cells (Fig. 1).
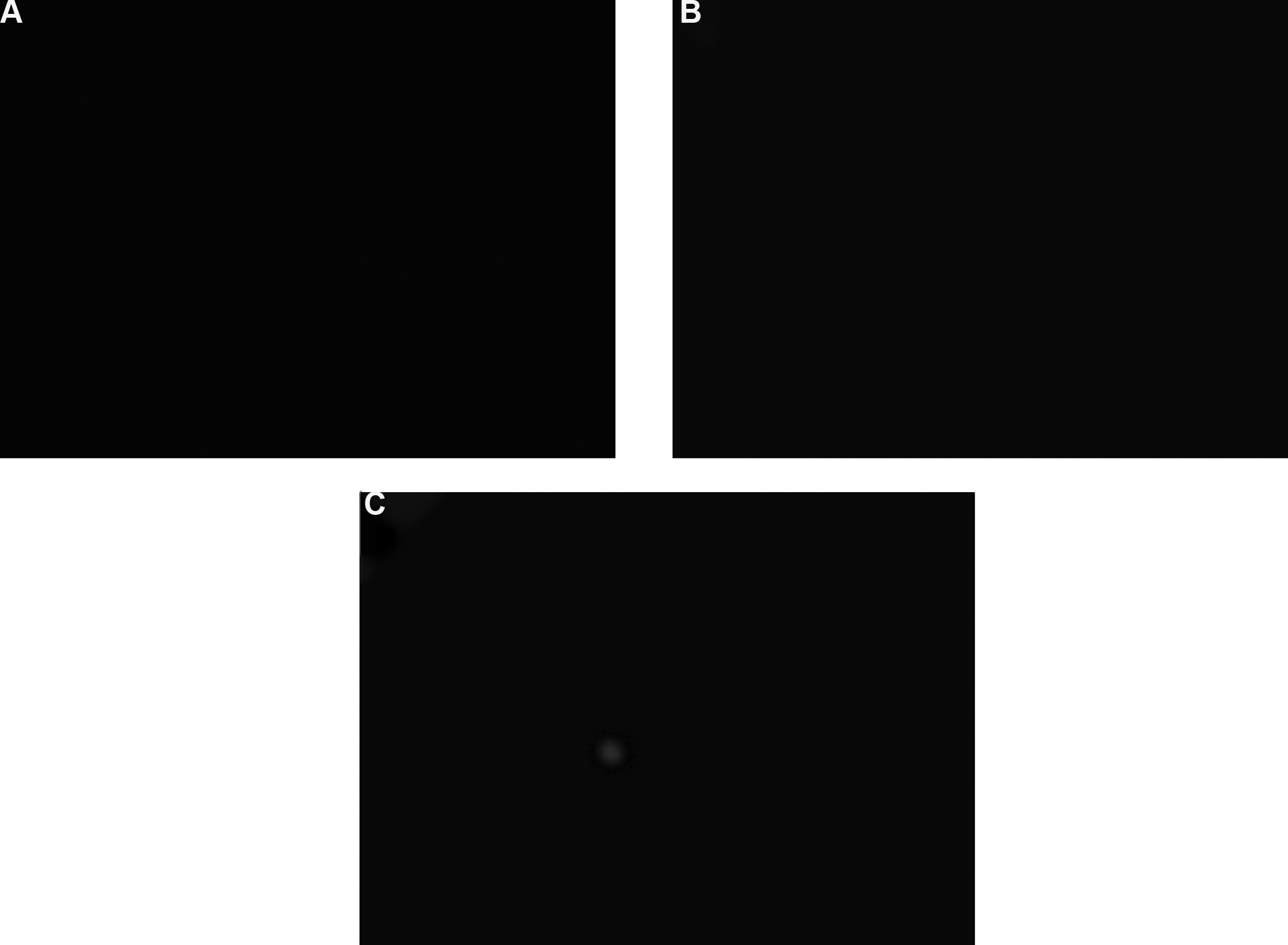
Donor cells with blue fluorescence in peripheral blood smears of the detection subgroup at day 7 after transplantation. (A) The model-only control group. (B) The tail vein injection group. (C) The intraperitoneal injection group. The intraperitoneal injection group rats exhibited positive donor cell engraftment, while the other groups of rats did not exhibit any positive cells (400×, n = 50).
The serum CD4+/CD8+ T cell number was detected 7 days after treatment.
The value of the serum cellular immune function parameter in the tail vein injection group was higher than that in the control group and the intraperitoneal injection group (2.7898 ± 0.44392 vs. 2.5058 ± 0.31596, P = .000; 2.7898 ± 0.44392 vs. 2.5322 ± 0.39792, P = .001, respectively). However, there was no significant difference in this parameter between the intraperitoneal injection and control groups (P = .735, Fig. 2)
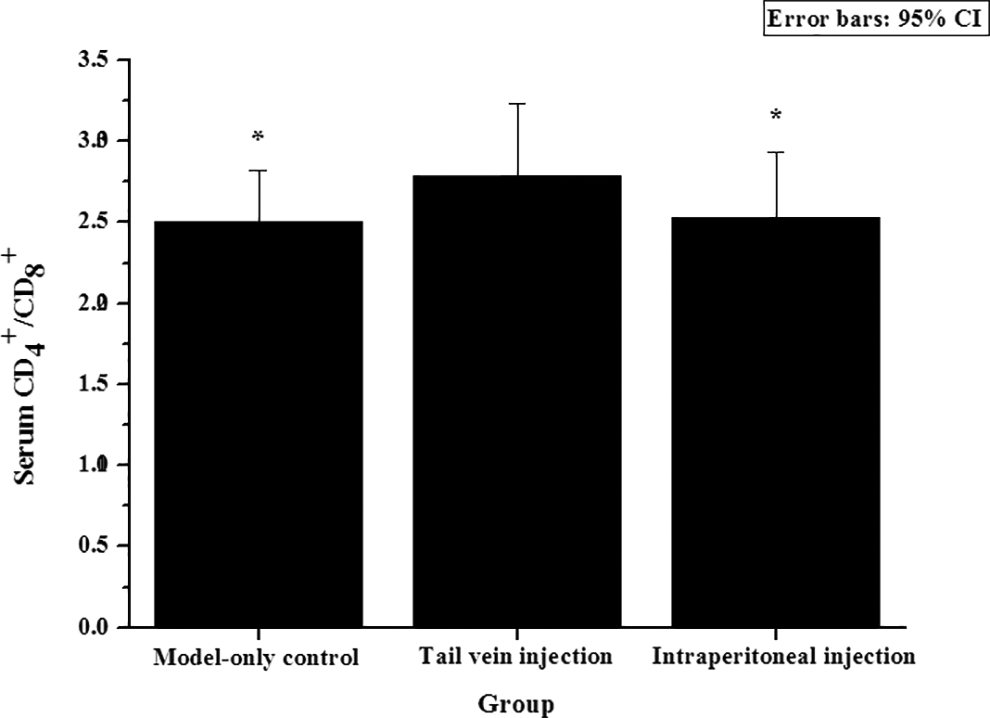
The serum CD4+/CD8+ T cell number in the three detection subgroup at day 7 after transplantation (n = 50). The value of the cellular immune function parameter in the tail vein injection group was higher than that in the other two groups.
The serum levels of TNF-α and IL-6 were measured 7 days after treatment.
The serum TNF-α and IL-6 levels in the intraperitoneal injection group rapidly decreased on day 7 after treatment. These values were significantly different from those of the model-only control and tail vein injection groups (all P = .000, n = 50). However, when the latter two groups were compared, we found that administration of UCMSCs with a tail vein transplantation approach did not suppress serum proinflammatory cytokine production (Figs. 3 and 4).
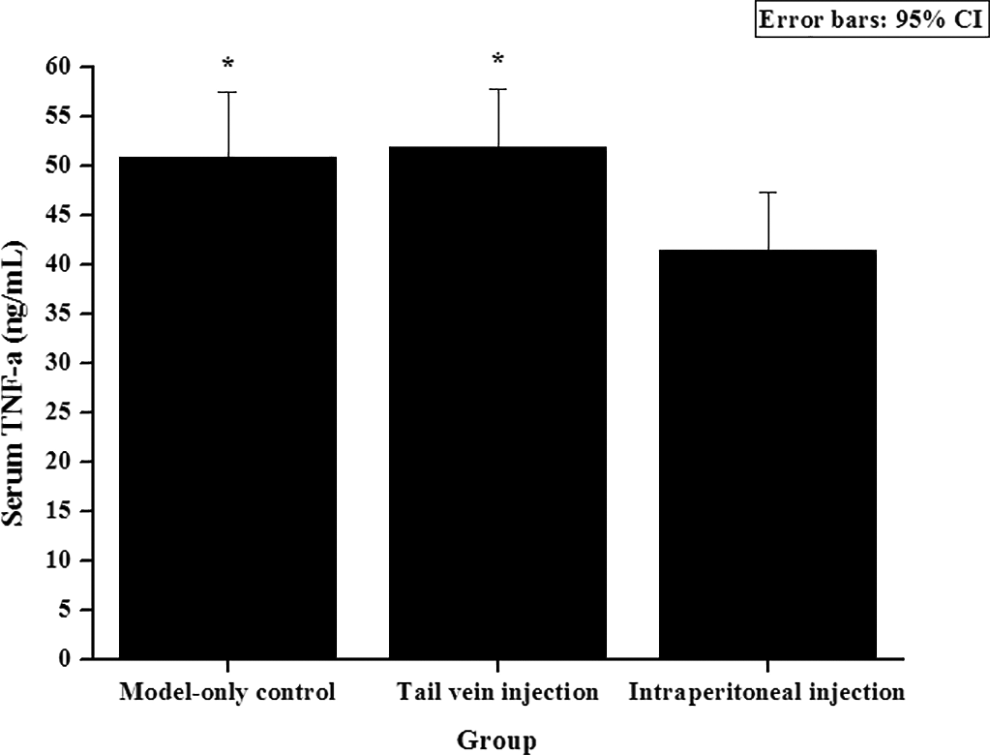
Inflammatory cytokine TNF-α levels in serum. UCMSCs of the intraperitoneal injection group suppressed proinflammatory cytokine TNF-α production in vivo 7 days after treatment (n = 50, *P < .001 vs. the intraperitoneal injection group).
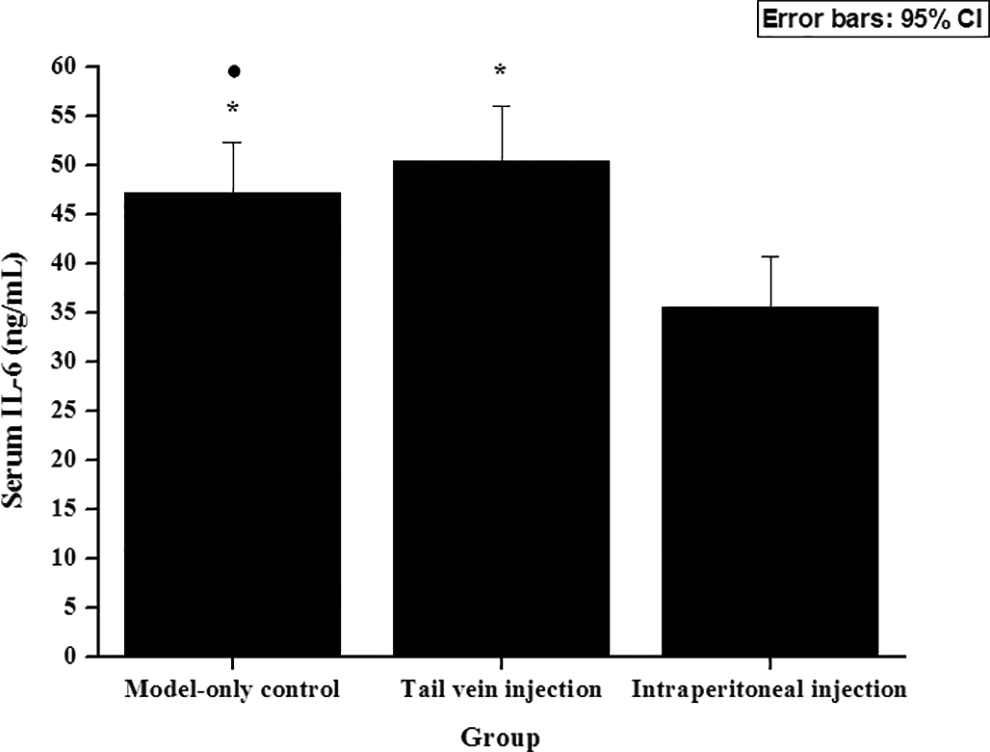
Serum inflammatory cytokine IL-6 levels on day 7 after treatment (n = 50). UCMSCs suppressed proinflammatory cytokine IL-6 production induced in vivo in the intraperitoneal injection group. Notably, UCMSCs in the tail vein injection group adversely affected the serum level of IL-6.
The serum TNF-α level in the intraperitoneal injection group was significantly decreased compared with that in the model-only control and tail vein injection groups (41.50 ± 5.807 vs. 50.84 ± 6.656, P = .000; 41.50 ± 5.807 vs. 51.84 ± 5.884, P = .000, respectively). However, there was no significant difference in this parameter between the tail vein injection and model-only control groups (P = .735, Fig. 3)
The serum IL-6 level in the intraperitoneal injection group was significantly decreased compared with that in the model-only control and tail vein injection groups (35.62 ± 5.154 vs. 47.12 ± 5.282, P = .000; 35.62 ± 5.154 vs. 50.38 ± 5.696, P = .000, respectively). Interestingly, the IL-6 level was significantly increased in the tail vein injection group compared with the model-only control group (P = .003, Fig. 4).
Abdominal exudate fluid was collected 7 days after treatment.
The intraperitoneal injection group had lower exudate fluid CD4+/CD8+ values than the model-only control and tail vein injection groups on day 7 post-transplantation (1.5254 ± 0.39534 vs. 1.7418 ± 0.39223; 1.5254 ± 0.39534 vs. 1.7098 ± 0.41852, both P < .05, Fig. 5). However, the difference between the other groups did not reach statistical significance.
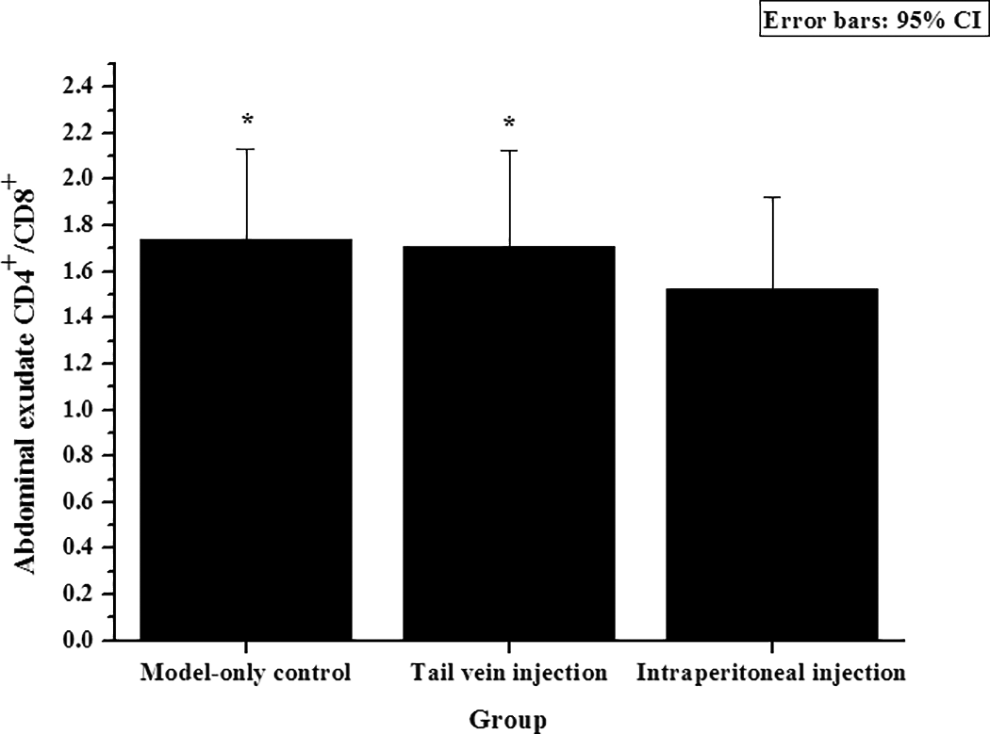
Intraperitoneally injected UCMSCs alleviated the cellular immune response in abdominal exudate (n = 50).
The abdominal exudate fluid TNF-α and IL-6 levels were measured 7 days after treatment.
The abdominal exudate fluid TNF-α of the intraperitoneal injection group was significantly decreased compared with that of the model-only control and tail vein injection groups (30.34 ± 6.100 vs. 33.84 ± 6.594; 30.34 ± 6.100 vs. 35.42 ± 6.004, both P < .01). However, there was no significant difference in this parameter between the other groups (Fig. 6)
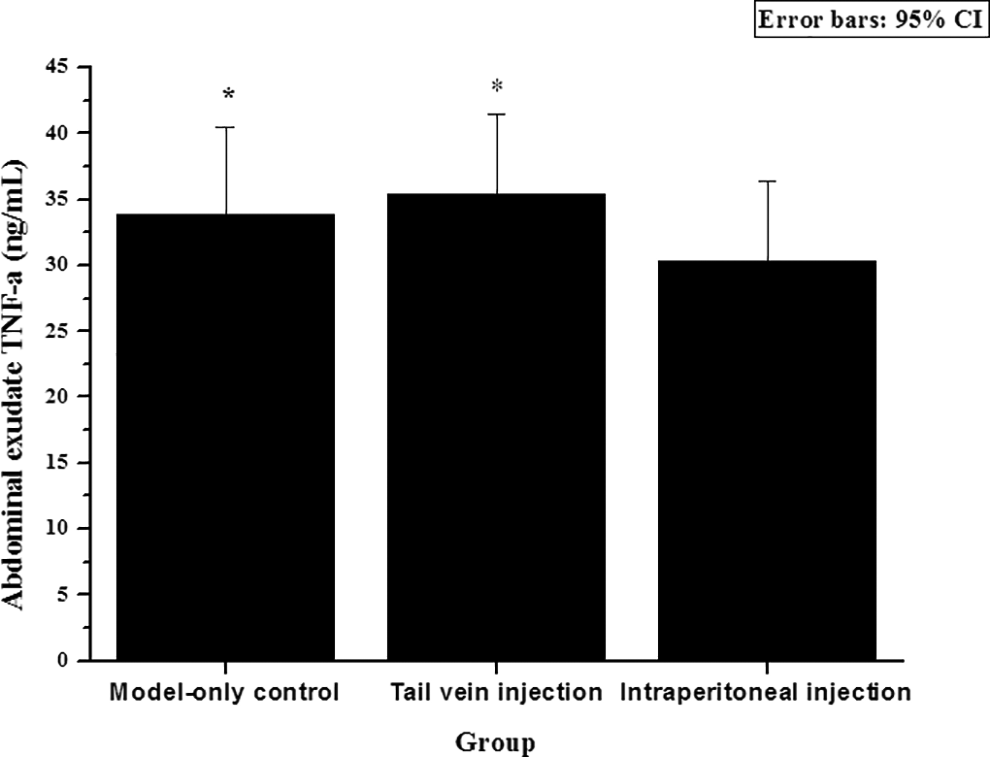
Levels of the inflammatory cytokine TNF-α in the abdominal exudate. UCMSCs of the intraperitoneal injection group suppressed proinflammatory cytokine TNF-α production 7 days after treatment (n = 50, *P < .01 vs. the intraperitoneal injection group).
The abdominal exudate fluid IL-6 level of the intraperitoneal injection group was significantly different from that of the model-only and tail vein injection groups (244.20 ± 51.353 vs. 267.80 ± 48.991, 244.20 ± 51.353 vs. 273.80 ± 56.960, both P < .05). When the latter two groups were compared, we found that administration of UCMSCs with a tail vein transplantation approach did not suppress exudate IL-6 production (P > .05, Fig. 7).
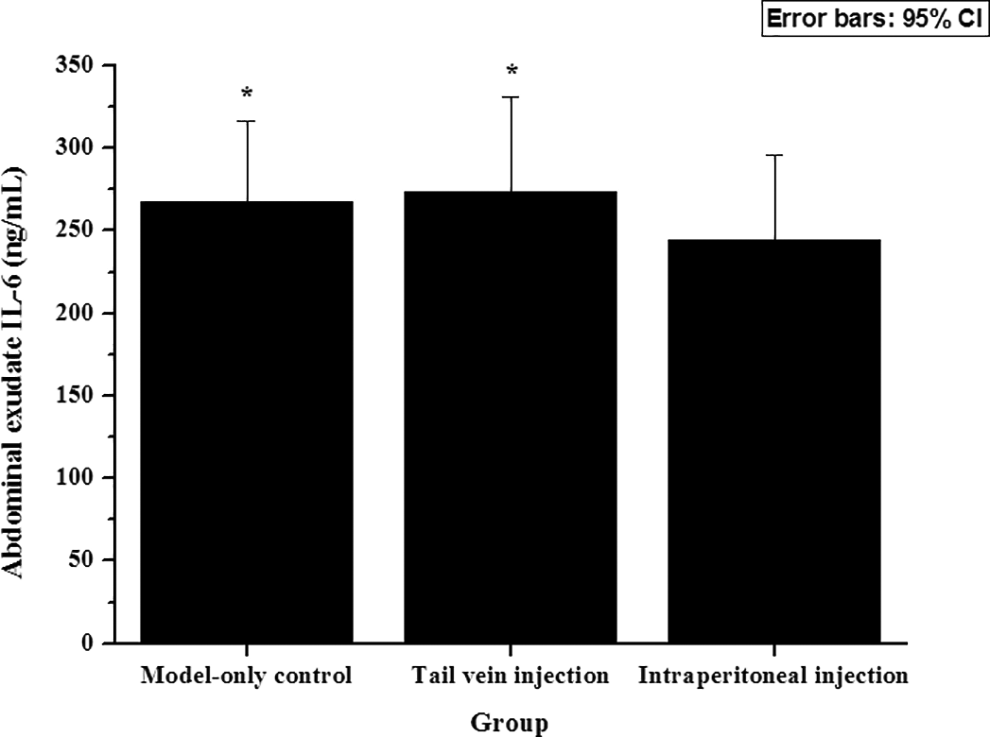
Inflammatory cytokine IL-6 levels of the abdominal exudate on day 7 after treatment (n = 50).
Preservation of the Mucosa
Loss of integrity in the epithelium of jejunal mucosa was observed. Congested hyperemic (erythematous) mucosa was the most frequent lesion. Notable differences in mucosal surface area were observed in the intraperitoneal injection group compared to the model-only control and tail vein injection groups (0.3700 ± 0.04647 versus 0.3966 ± 0.02994, 0.4882 ± 0.07417, all P = .000) at day 7 after transplantation. However, the increase in mucosal surface area of the tail vein injection group was not significantly different from that of the model-only control group (P = .173, Fig. 8).
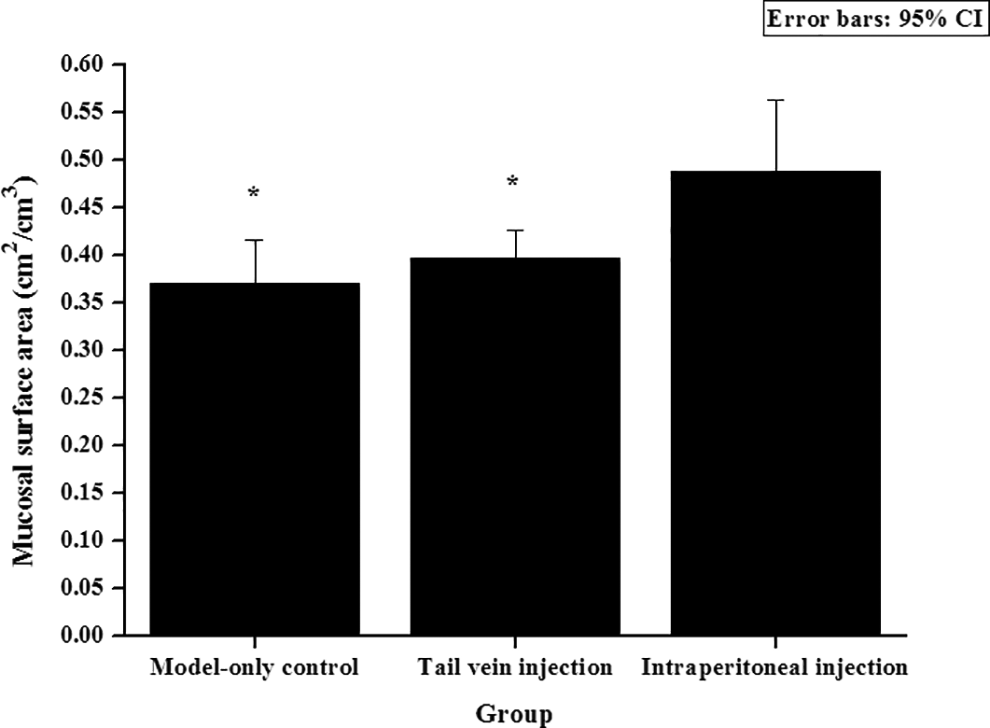
Preservation of the mucosa at day 7 after transplantation (n = 50). Notable differences in mucosal surface area were observed in the intraperitoneal injection group.
After cell injection, the rats in the lifespan subgroup were maintained until the day of their natural death for determination of post-transplantation survival time.
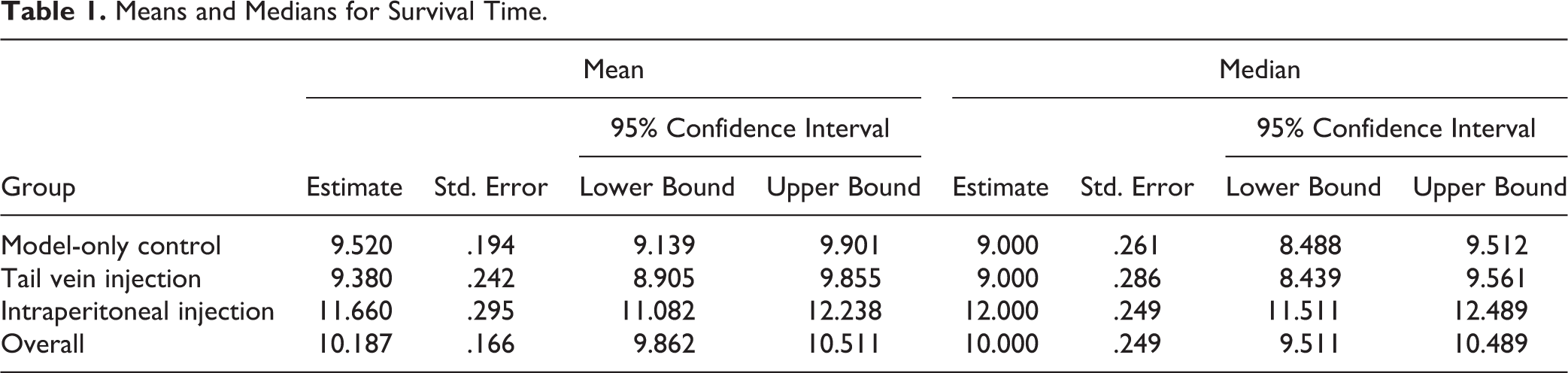
Death of the animals occurred after 7–16 days. All three tests revealed a significantly longer survival of the rats of the intraperitoneal injection group compared to those of the other groups (all P = .000). However, the Kaplan–Meier survival plot showed overlapping survival curves for the vehicle and tail vein injection groups, which demonstrated similar survival of these groups (Table 1, Fig. 9).
Means and Medians for Survival Time.
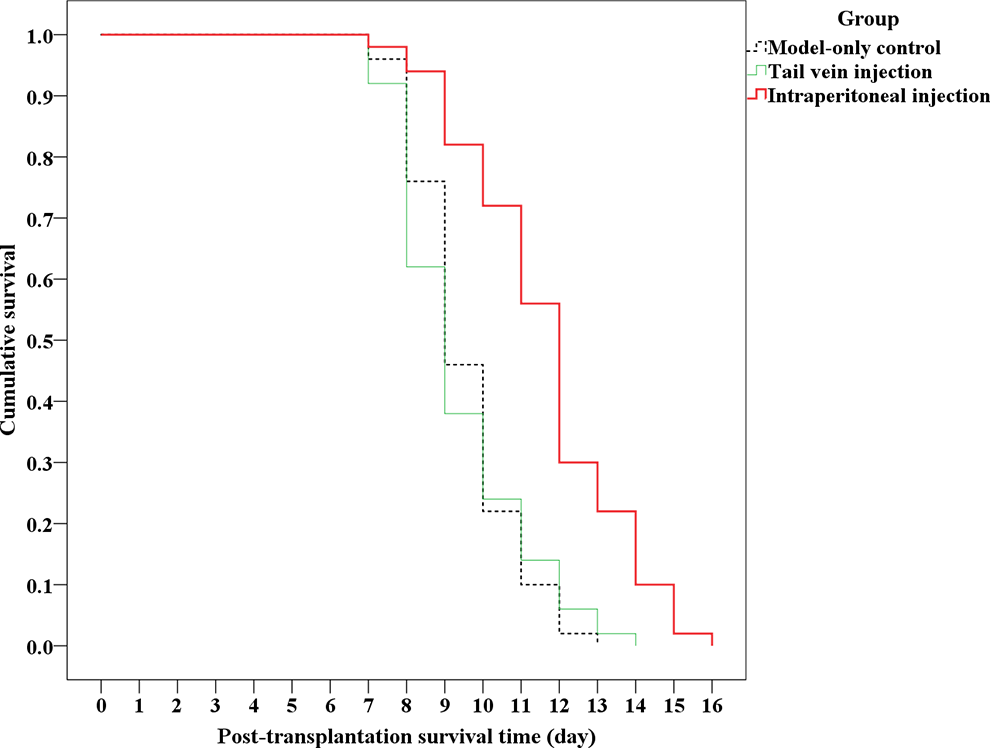
Cumulative survival curve of rats in the lifespan subgroup (n = 50).
Discussion
UCMSCs can suppress inflammation and modulate the host immune system and are immunosuppressive. Our results revealed that human multiumbilical cord-derived exogenous UCMSCs administered through a single intraperitoneal injection increase survival time in a rat model of acute radiation enteritis. The therapeutic mechanism of UCMSCs was analyzed in this model of severe and irreversible small intestinal disorders leading to death without intervention with immunosuppressants.
Trounson A described that there appears to be very little difference between autologous and allogeneic MSCs with regard to clinical effects 22 . MSCs act as cell protective agents by secreting paracrine factors such as anti-inflammatory and immunoregulatory cytokines 23 . The cotransplantation of double- or multiumbilical cord-derived stem cells can improve the allograft engraftment rate 24 . Repeated administration of allogeneic cells can enhance the host immune response 25 –27 . In addition, a sublethal dose of irradiation can destroy the donor immune system. All of these factors suggest the possibility for transient survival of singly transplanted xenogeneic UCMSCs.
UCMSCs injected intraperitoneally are anchorage-dependent cells that can adhere to the peritoneum or are packed into the greater omentum 28 , which provides an environment for the cells to grow and enter the blood circulation one by one, according to the principle of “desensitization treatment”. Although transitory in their existence following transplantation, these cells potentially alleviate the cellular immune response, which suggests that xenogeneic stem cells transiently survive. All these results agreed with the findings that intraperitoneally injected UCMSCs did not enhance the serum cellular immune response and alleviated it in the abdomen. Occasionally, UCMSCs in the intraperitoneal injection group were detected in peripheral blood smears at day 7 after transplantation. Our data showed that administration of Wharton jelly MSCs with a single intravitreal injection can result in engraftment into the host body through the blood system, survival for 7 days, and suppression of proinflammatory cytokine TNF-α and IL-6 production; thus, these cells play a protective role in the inflammation and necrosis of mucosa over time, as long as they postpone death elicited by acute radiation enteritis.
Both xenogenic cell transplantation and radiation damage can provoke an inflammatory reaction and immune response, which result in the production of TNF-a, IL-6 and other cytokines.
In the serum, the levels of the two inflammatory cytokines in the model-only group were significantly higher than those of the intraperitoneal injection group. This result indicated that the high proinflammatory cytokine levels of the model-only control were primarily related to sublethal radiation damage. However, the serum levels of inflammatory cytokines in the tail vein injection group were not lower than those in the model-only group, which indicated that the immune response reaction to xenogenic cell transplantation might participate in provoking an inflammatory reaction. The serum CD4+/CD8+ value of the tail vein-injected rats was higher than that of the other two groups. These results also suggested that xenogenic cell transplantation contributed to the high serum IL-6 level of the tail vein injection group.
The differences in abdominal exudate proinflammatory cytokine and CD4+/CD8+ levels between the model-only and tail vein injection groups were not significant. These values were significantly different from those of the intraperitoneal injection groups. This finding directly implied that the high inflammatory cytokine values of the model-only control and tail vein-injected rats were mainly related to radiation damage.
In this study, all of the UCMSCs injected at a draught via the tail vein entered the blood and circulated throughout the body, triggering a cellular immune response in the serum, which adversely affected their survival. UCMSCs injected via the tail vein did not survive for one week, failed to suppress TNF-α and IL-6 levels and were unlikely to provide a therapeutic benefit against acute radiation enteritis despite their cell protective effect. All of these results agreed with the finding that the differences in mucosal surface area and the survival time between rats in the tail vein injection and the model-only control groups were not significant.
In our study, we did not observe any donor cells in peripheral blood smear of tail vein injection group at day 7 after transplantation. This finding also indicates that the early death of UCMSCs in the tail vein injection group might generate numerous cell decomposition products etc. inflammatory chemicals, which might explain why the serum IL-6 level was significantly higher in the tail vein injection group than in the other two groups.
This research also suggests that some stem cell transplantation failures in clinical trials might be related to the strategic design and suggests administration of P2 generation human multiumbilical cord-derived MSCs with Nutrient Mixture DMEM/F-12 Media by a single intraperitoneal injection as a better therapeutic protocol with potential benefits.
Conclusion
Human multiumbilical cord-derived UCMSCs were administered via a single intraperitoneal injection into rats, and rat proinflammatory cytokine levels, mucosal surface area, and survival time improved significantly in this model. UCMSCs can be carried through the blood circulation and engraft into the host body, and some even survive for 7 days. The safety as xenogenic cell transplants might be closely related to their short-term presence. The transient therapeutic benefit of UCMSCs for prolonging life might be the consequence of their anti-inflammatory action. Other mechanistic studies are needed to elucidate this issue.
Footnotes
Author Contributions
Wei Xue conceived the study. Jun Li and Yinghong Jiang designed the experiments. Hua Yu, Lejiang Liu, Qiang Wang, Hongpin Ju, Xuemei Zhang, Wenqi Wang, Xudong Yin, Qiong Wu, Jianzhong Xiao, Jianrong Miao, Xiao Ye, Tianyu Li and Hui Tian performed the experiments. Jun Li wrote the manuscript. Wei Xue reviewed and revised the manuscript. All authors read and approved the final manuscript.
Authors Contribution
Jun Li and Yinghong Jiang contributed equally to this article.
Ethical Approval
All experimental protocols were approved by the Institutional Animal Care and Use Committee for Medical Sciences of Kunming University.
Statement of Human and Animal Rights
All of the experimental procedures used in this study were conducted in accordance with the Institutional Animal Care Guidelines of Kunming University, and were approved by the Ethics Committee on Animal Experiments of the Institutional Animal Care and Use Committee for Medical Sciences of Kunming University.
Statement of Informed Consent
Written informed consent was obtained from the full-term uterine-incision delivery donors for their anonymized information to be published in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from Yunnan provincial basic research joint projects with local undergraduate colleges and universities (2017FH001-086), the youth project of applied basic research of Yunnan Provincial Science and Technology Department (2018FD031), and the research start-up project of the first batch of talents introduced by Ningde Normal University in 2021 (2021Y11).